
Abstract
Carcinoma showing thymus-like differentiation (CASTLE) is a rare malignant tumor that accounts for 0.1%–0.15% of all thyroid cancers. More than half of the patients have tumor extension to adjacent organs, including the recurrent laryngeal nerve, trachea, and esophagus. The diagnosis of CASTLE is based on histology and immunohistochemistry. A 58-year-old female patient complained of hoarseness for one and half years. Right side vocal cord palsy was diagnosed by fiberscopy. Thyroid sonography revealed right thyroid tumors, which were reported to be papillary thyroid carcinoma through FNAC. Total thyroidectomy with central lymph node dissection was performed. Pathologist found 2 isolated malignancy tumors. One patient in the right thyroid lobe had papillary thyroid carcinoma features. The other extrathyroid tumor seemed to be separated from the first tumor and invaded the thyroid capsule. After multiple immunohistochemical studies, PTC synchronous CASTLE was the final diagnosis. Coexisting PTC and CASTLE is very rare. This is the first report to describe a case showing PTC at first, while subsequent pathologic examination revealed the presence of CASTLE in addition to PTC. Since the prognosis of CASTLE is favorable, the treatment is different from other aggressive thyroid cancers, such as poorly differentiated or anaplastic thyroid carcinoma.
Keywords
Introduction
Carcinoma showing thymus-like differentiation (CASTLE), which is a rare malignant tumor, accounts for 0.1%–0.15% of all thyroid cancers. 1 It was first described by Miyauchi et al 2 as intrathyroidal epithelial thymoma in 1985 and then was reported to exist in either thyroid tissue or extrathyroid area. Thymus tissue is derived from the third and fourth branchial pouch and descends into the mediastinum. This tumor arises from either ectopic thymus tissue or remnants of branchial pouches or thymopharyngeal duct.3,4 In 1991, Chan and Rosai morphologically classified neck tumors derived from ectopic thymus into 4 groups, including ectopic hamartomatous thymoma, ectopic cervical thymoma, spindle epithelial tumor with thymus-like differentiation (SETTLE), and CASTLE. The first two are considered to be benign, and the last two are malignant. 5 In 2004, this disease was designed as an independent clinicopathologic entity among thyroid carcinomas according to the World Health Organization classification. 3 CASTLE usually affects middle-aged adults in approximately fourth and fifth decades of life. It has a slight female predominance. 1 The most common symptoms are slowly growing and painless neck tumors. Patients also complained of hoarseness due to recurrent laryngeal nerve involvement. 6 Dyspnea, dysphagia, or rapidly growing tumors rarely occur. Patients usually have a normal range of serum thyroxine, thyroid-stimulating hormone, and thyroglobulin concentrations. 7 Because CASTLE is a favorable prognostic neoplasm, the treatment varies from other aggressive thyroid cancers, such as poorly differentiated or anaplastic thyroid neoplasms. We present a case of fine needle aspiration cytology (FNAC) showing papillary thyroid carcinoma (PTC) at first, while subsequent pathologic examination revealed the presence of CASTLE in addition to PTC.
Case Report
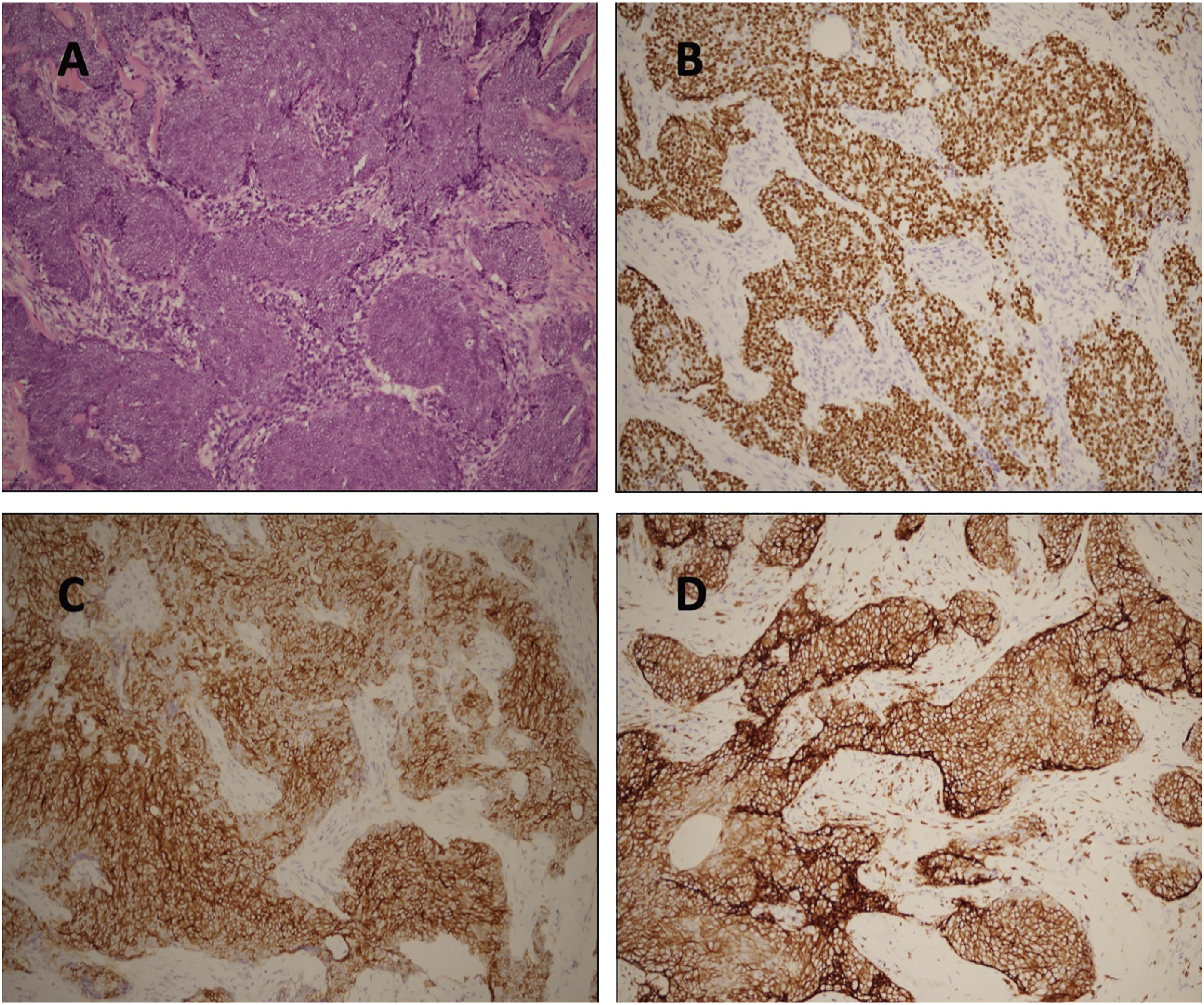
This is a 58-year-old female with a past history of Sjogren syndrome who presented hoarseness for one and half years. She denied dysphagia or dyspnea. Right side vocal cord palsy was diagnosed by nasolaryngoscopy. Thyroid sonography was performed and revealed multiple hypoechoic and heterogeneous intrathyroid masses maximal measuring 18 × 24 mm in the right thyroid lobe. Ultrasound-guided fine needle aspiration cytology (FNAC) was performed in one of the masses in the right thyroid lobe that showed PTC. Head and neck computed tomography (CT) revealed an extrathyroid soft tissue tumor measuring 20 × 25 mm located in the right paratracheal region and inferior to the right thyroid gland (Figure 1A, B). Thyroid function tests, including T4, T3, and TSH, were all in the normal range. Then, the patient underwent total thyroidectomy and central lymph node dissection. During the operation, the extrathyroid soft tissue tumor adhesive to the right thyroid gland was found to encase the right recurrent laryngeal nerve and trachea. Shave excision of the tumor was performed. (Figure 2). Histopathologic analysis of the specimen showed two different malignant tumors. The intrathyroid mass represented by PTC, another separate with involvement of thyroid and adjacent soft tissue, was composed of syncytial sheets of tumor cells with round vesicular nuclei and indistinct nucleoli accompanied by dense infiltration of lymphoplasmacytic cells. (Figure 3A). Immunohistochemical staining was positive for P40 (Figure 3B), AE1/AE3, CD117 (Figure 3C), and CD5 (Figure 3D) and negative for PAX8, CEA, and NUT. EBER in situ hybridization was negative as well. The final pathological diagnosis was PTC with synchronous CASTLE involving the right thyroid lobe. The patient received radioactive iodine (I131) after surgery. However, she still hesitated about adjuvant radiotherapy. We closely followed her condition for the chance of recurrence. (A and B) Head and neck CT showed a 2 cm soft tissue tumor located at right paratracheal region and inferiorly to right thyroid gland (star). The specimen of total thyroidectomy and the extrathyroid soft tissue tumor (arrow). The tumor cells were arranged in syncytial sheets with mildly pleomorphic, vesicular nuclei and small nucleoli (A). Immunostaining showed nuclear expression of P40 (B), and membranous expression of CD117 (C) and CD5 (D) in tumor cells, respectively (×200).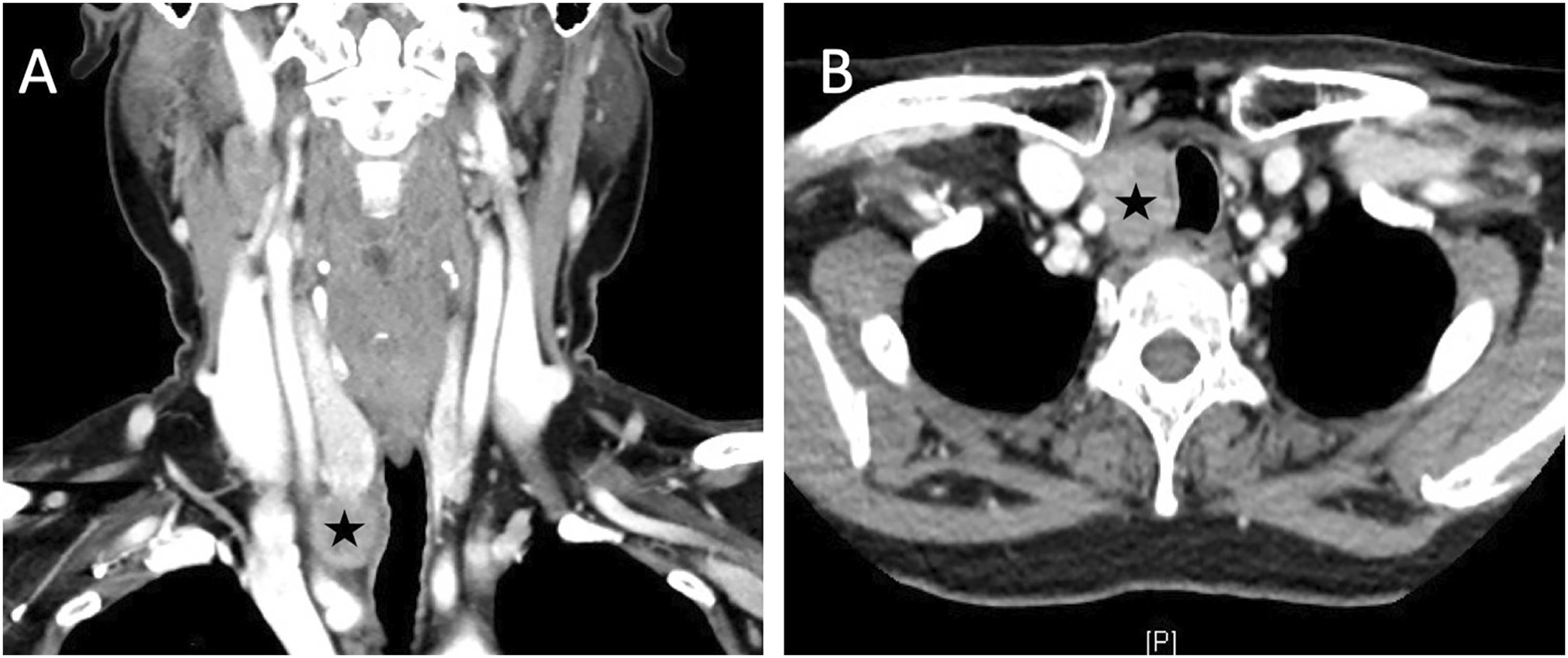

Discussion
The differential diagnosis of CASTLE includes primary squamous cell carcinoma of the thyroid, papillary thyroid carcinoma, follicular thyroid carcinoma, anaplastic carcinoma, metastatic lymphoepithelioma-like carcinoma, undifferentiated carcinoma with squamous features, metastatic squamous cell carcinoma from other organs, and Hurthle cell carcinoma.3,4,8,9 CASTLE tumors usually occur at the lower pole of the thyroid gland. The extrathyroid area between the inferior pole of the thyroid and upper mediastinum is relatively rare. 7 We reviewed previous reports of CASTLE thyroid tumors, and a series of 62 patients is listed (appendix). The most common symptoms are neck mass followed by hoarseness. Among 62 patients, 8 (12.9%) patients had extrathyroid CASTLE, and the other 53 (85.5%) patients had intrathyroid CASTLE. One patient did not mention the CASTLE tumor location. Among these 62 patients, 4 (6.5%) patients had recurrent laryngeal nerve invasion. Twelve (19.4%) patients had trachea invasion. Two (3.2%) patients had esophagus invasion. Twenty (32.3%) patients had tumor extension to adjacent soft tissue. Four (6.5%) patients had distant metastasis.
Ultrasonography of CASTLE usually shows solid, lobulated, hypoechoic, heterogeneous, and moderate vascularity masses without calcification.3,4,8,10,11 Fine needle aspiration cytological examinations had limited diagnostic value for CASTLE. 11 CT of CASTLE reveals a well-defined mass without calcification, soft tissue density similar to muscle, and slight heterogeneous enhancement after contrast medium injection.4,8,11
The microscopic features often indicate that tumor cells are polygonal, squamoid, or spindle shaped with eosinophilic cytoplasm and oval nuclei and well-defined nucleoli. Prominent nucleoli with low mitotic counts are usually seen.3,7,12 Immunohistochemical analysis revealed that the majority of CASTLE cells were positive for CD5, CD117, and p63. The sensitivity and specificity of the pathologic diagnosis of CASTLE by immunohistochemical staining with CD5, a marker of thymic origin, were 82% and 100%, respectively. 3 CASTLE and thymic carcinoma are usually CD5−and CD117-positive, whereas the majority of thymoma and thyroid follicular cell tumors are negative for these markers. 8 However, the lack of CD5 expression does not completely rule out CASTLE. The final diagnosis should be based on the H&E findings. 3 Other studies analyzed CASTLE markers and found that some CASTLE patients were also positive for cytokeratin protein, carcinoembryonic antigen (CEA), Bcl-2, cyclin D-1, cytokeratin 34bE12, chromogranin-A, and synaptophysin. Some CASTLE tumors are negative for thyroglobulin, TTF-1, calcitonin, cytokeratin 7, cytokeratin 20, vimentin, and parathyroid hormone.3,8,13
Prognosis of CASTLE is good. The 5- and 10-year cause-specific survival rates were 90% and 82%, respectively. Nodal metastasis and tumor extension are poor prognostic predictors. 3 The time of recurrence ranged from 1 month to 17 years.10,12,14 The recurrence rate is approximately 24% to 32%.3,9,14 Locoregional recurrence includes cervical lymph nodes and muscle. 3 Common distant metastasis sites are the lung, liver, bone, mediastinum, and pleura. 11 The most effective treatment for CASTLE is tumor resection and lymph node dissection followed by radiotherapy. 3 Gao et al. (2018) found that neck dissection prolonged the survival of patients with extrathyroidal extension in subgroup analysis. 11 Some reports have revealed that if neck dissection had positive lymph nodes, adjuvant radiotherapy could reduce the recurrence rate from 100% to 57%. Several reports have suggested that chemotherapy has no evidence of benefit.4,11 Chemotherapy could be used in patients with advanced or metastatic disease.
In a collaborative study in Japan, almost 84% of CASTLE tumors did not coexist with thyroid nodules among a total of 25 patients. 3 Two (8%) patients had CASTLE with papillary or follicular carcinoma, which was found incidentally. 3 Compared with anaplastic thyroid carcinoma (ATC), approximately 50% of ATCs coexist with well-differentiated thyroid carcinoma. 15 The possible theory is that ATCs transform from well-differentiated tumors, while CASTLE arises from ectopic thymus tissue or remnants of branchial pouches. This is the first report to describe a case showing PTC at first, while subsequent pathologic examination revealed the presence of CASTLE in addition to PTC. It is worth noting that I131 may be performed before adjuvant radiotherapy. Magnetic resonance imaging (MRI) and positron emission tomography (PET) may be applied rather than CT scans for radiotherapy planning to avoid the effect of iodine-based contrast agents on I131 radioablation therapy.
Conclusion
Coexisted PTC and CASTLE is very rare. Clinicians and pathologists should keep CASTLE as a differential diagnosis in lower thyroid neoplasms invading the recurrent laryngeal nerve, trachea, and esophagus. Because CASTLE is a favorable prognostic neoplasm, the treatment varies from other aggressive thyroid cancers, such as poorly differentiated or anaplastic thyroid neoplasms. Tumor excision and selection neck dissection with postoperative radiotherapy are first-line treatments. Clinicians should closely follow-up for the chance of recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Case Review of 62 Patients Diagnosed with CASTLE
Abbreviations: LN, lymph node; yr, year; mon, month; wk, week; RLN, recurrent laryngeal nerve; MRND, modified radical neck dissection; ND, neck dissection; RT, radiotherapy; NER, no evidence of recurrence; FDC sarcoma, follicular dendritic cell sarcoma; SOB, shortness of breath; CR, complete remission; CCRT, chemoradiotherapy.
Author
Case Number
Age/Sex
Symptoms
Tumor Location
Treatment
Outcome
Willis, 1960
1
25/F
Neck swelling for 3 yr
Soft tissue of left anterior neck
Excision
LNs(+) local recurrence after 6 mon; died 2 yr later
Miyauchi, 1985, 1989
2
51/F
Right lower neck mass for 1 mon
Right thyroid lobe lower pole
Right thyroid lobectomy with dissection of cervical LNs
LN (−) NER at 17 yr
3
59/F
Left low anterior cervical nodule for 3 yr
Middle to lower portion of the left thyroid lobe
Partial lobectomy
Slow-growing local recurrence 17 yr later; died of a cerebrovascular disorder 1 yr later (not treated because of age)
4
47/F
Goiter and pressure on her neck for 4 months
Middle to lower portion of the left thyroid lobe, left recurrent laryngeal nerve invasion
Left thyroid lobectomy, MRND, left RLN resection
NER at 14 yr
5
65/F
Neck mass for 1 yr
Lower left thyroid, with palpable LN
Subtotal thyroidectomy, ND, RT
NER at 14 yr
6
52/M
Hoarseness for 11 mon
Lower left thyroid, fixed to the trachea, palpable LN
Subtotal thyroidectomy, ND, tracheoplasty, RT
LN metastasis (1 of 32 LNs), tumor recurrence in the mediastinum at 6 yr, treated with additional RT; died of disease at 8 yr
7
29/F
Neck mass for 1 mon
Middle-lower right thyroid, fixed to the trachea, palpable LN
Subtotal thyroidectomy, ND, tracheoplasty + RT
LN metastasis (3 of 67 LNs), tumor recurrence in the lung at 3 yr, treated by partial resection of lung, alive with pleural effusion at 8 yr
Kakudo, 1988
8
59/M
Left neck mass
Left thyroid lower pole, palpable LN (+)
Subtotal thyroidectomy, MRND + RT
Pulmonary metastasis at 14 mon, treated with chemotherapy, died of carcinomatosis (bone and liver metastases) at 17 mon (autopsy)
Asa, 1988
9
35/M
Right thyroid mass
Majority of the right thyroid lobe
Subtotal thyroidectomy, right RLN resection
Subglottic recurrence at 9 yr, treated with RT, then remained asymptomatic; right lower neck recurrence with extension into the trachea and right vocal paralysis at 15 yr, treated with salvage surgery, NER for at least 3 yr
Chan, 1991
10
43/F
Recurrent left neck mass
Left upper jugular region
Excision first, after recurrence, re-excision, left RND, RT
Ethmoid-sphenoid recurrence at 4 yr, treated with surgery, chemotherapy and RT; lung metastasis at 12 yr, treated with surgery, diagnosis was corrected with FDC sarcoma (local recurrence after 15 yr)
11
69/M
Neck swelling for yrs
Almost entire thyroid and surrounding soft tissue, trachea invasion
Excision, RT
NER at 2 yr
Damiani, 1991
12
47/F
Anterior neck nodule for 18 mon with increasing dyspnea and difficulty in swallowing
Central portion of the thyroid, adherent to deep soft tissues extending to the tracheal wall (inoperable)
Tracheostomy, RT 3 yr later to shrink the mass
Mass decreased slightly in size and remained unaltered for the following 7 yr; died of myocardial infarction
Mizukami, 1995
13
59/F
Right neck mass
Right thyroid lower portion
Subtotal thyroidectomy, bilateral ND
NER at 2 yr
14
71/M
Neck mass for 1 yr
Right anterior neck mass involving entire thyroid with extension into the lower neck and trachea, palpable LN
Total thyroidectomy, RND, laryngotracheal resection
LN metastasis, died of local recurrence at 6 mon
Shek, 1996
15
39/F
Right neck nodule for 1 wk, and follow-up 2 yr later
Right thyroid lower portion
Right thyroid lobectomy with isthmus resection
NER at 15 mon
Ahuja, 1998
16
67/F
Left neck mass that enlarged rapidly
Left side of neck (extrathyroid at carotid and posterior spaces), palpable LN
Resection of the mass and the LNs along the internal jugular vein. RT
LN metastasis (1 of 22 LNs), NER at 3 yr
Da, 1999
17–24
35–62/5M+3 F
Neck mass
5 at right lower thyroid, 3 at left lower thyroid
Excision
2 recurrences at 1/2 yr, treated with surgery twice, NER 9 and 11 yr; 1 recurrence at 3 mon with neck LN metastasis; died of liver and lung metastases at 3 yr; 5 NER, 14 yr longest (median, 10.5 yr)
Tai, 2003
25
34/M
Left lower neck mass for 18 mon
Left lower thyroid
Left thyroid lobectomy, RT (5000 cGy)
NER at 20 mon
Luo, 2005
26
47/M
Left neck mass for 3 mon
Extrathyroid, left parapharyngeal space with displacement of left carotid artery and submandibular gland
Left thyroid lobectomy, RT (5000 cGy), excision, RT (6600 cGy)
NER at 21 mon
Morikawa, 2005
27
38/F
Anterior neck swelling for 3 yr
Left thyroid
Thyroid lobectomy, ND
Alive and NER 3 yr
Shek, 1996
28
39/F
Neck discomfort for 2 yr
Right lower thyroid
Right lobectomy with isthmus resection
Alive and NER 15 mon
Wantanabe, 1996
29
32/F
Anterior neck mass for 3 mon
Left thyroid
Total thyroidectomy, ND
Local recurrence 5 mon
Nassar, 2003
30
39/F
––
Right thyroid
Thyroidectomy
Recurrence after 6 mon in paratracheal LN
Kusada, 2005
31
68/M
Right anterior neck swelling for 1 mon
Right thyroid and lung metastasis
Right lobectomy, adjacent lymphadenectomy
Died 11 mon after operation with lung metastasis
Yoneda, 2005
32
54/M
Hoarseness and SOB for 5 yr
Right thyroid, invade into right trachea
Total thyroidectomy, resection of segmental trachea + right common carotid artery + internal jugular vein, reconstruction of the common carotid artery
Alive and NER 2 yr
Roka, 2004
33
48/F
Right thyroid tumor
Right thyroid
Thyroidectomy, functional ND, chemotherapy
LN recurrence after 8 mon; liver metastasis after 19 mon; bone marrow metastasis after 30 mon, chemotherapy, alive 47 mon after diagnosis
Roka, 2004
34
31/M
Left neck mass
Left thyroid
Thyroidectomy, partial resection of innominate vein and left RLN, bilateral modified ND, trans-sternal lymphadenectomy and thymectomy, RT
Local recurrence after 19 mon in the esophagus and subclavian vein, partial resection of the esophagus, subclavian vein, clavicle, and pleura, surgery was not radical because of tumor invasion into the vertebral column, RT, =>65 mon lung metastasis, chemotherapy CR, alive
Chan, 2008
35
54/M
Left lower anterior neck 3 mon
Left thyroid
Median sternotomy, left thyroid lobectomy
Alive and NER 36 mon
Chow SM, 2007
36
43/M
Rapid growing thyroid nodule
Thyroid tumor extend to muscles, trachea, esophagus, and left laryngeal nerve
Debulking with residual disease, RT
NER at 6 yr
37
49/M
Anterior neck mass
Thyroid tumor extend to the trachea and superior mediastinum
Debulking thyroidectomy, CCRT
Recur at right tracheo-esophageal groove, s/p operation, RT, NER at 2.5 yr
38
62/F
Hoarseness and dysphagia for wks
Left thyroid tumor with superior mediastinal and tracheal involvement
CCRT then total thyroidectomy
NER at 1.8 yrs
Rodrigues TA, 2008
39
52/M
Cough, disphony, asthenia, and thyroid mass
––
Thyroidectomy, CCRT
NER at 13 mon
Yamazaki M, 2008
40
62/M
Cough with sputum, neck lump for 6 mon
Left dorsal aspect of the trachea that was connected to the inferior portion of the left lobe of the thyroid gland, extended into the submucosal layer of the esophagus, and the tracheal epithelium was ulcerated by the protruding tumor, LN metastasis
Total pharyngolaryngoesophagectomy combined with total thyroidectomy, reconstruction with a free jejunal graft
NER at 5 mon
Chan LP, 2008
41
54/M
Left lower anterior neck 3 mon
Inferior left lobe of the thyroid gland and left upper mediastinum. The mass displaced and compressed the trachea
Left thyroid lobectomy
NER at 36 mon
Youens KE, 2010
42
52/F
Intermittent neck pain, mild swelling for 1 yr
Left thyroid tumor with left RLN and extended into the extra-laryngeal soft tissue and tracheal cartilage
Thyroidectomy with primary tracheal resection and left paratracheal node dissection, RT
NER at 5 mon
Chang S, 2012
43
34/F
Sore throat for 2 mon
Lower pole of the right thyroid, with vascular and extra-thyroidal extension, one regional LN metastasis
Total thyroidectomy
NER at 27 mon
Geraci G, 2013
44
63/M
Slow enlargement of the thyroid and dysphagia
Lobulated nodules in the lower part of the bilateral thyroid
Total thyroidectomy, RT
NER at 1 yr
Huang C, 2013
45
41/F
Right lower anterior neck mass 6 months
Lower portion of the right thyroid lobe
Thyroidectomy, right sternothyroid muscle, bilateral modified ND, and trans-sternal lymphadenectomy, RT
NER at 1 yr
Hsu HT, 2014
46
50/F
Right side neck non-tender mass for 5 wks
Right thyroid gland with retrosternal extension
Total thyroidectomy
-
Zhang G, 2014
47
37/F
Right neck tumor
Right thyroid lower portion
Right thyroid lobectomy
NER at 6 mon
48
38/M
Hoarseness for 2 mon
Inferior half of the right thyroid with tracheal displacement to the left
Right thyroid lobectomy with MRND
NER at 26 mon
49
29/F
Lower half of the neck anteriorly 7 mon
Middle-to-lower portion of the right thyroid lobe and the isthmus and extended into the surrounding soft tissue
Total thyroidectomy combined with a radical ND
NER at 42 mon
Abeni C, 2014
50
26/M
minimal neck edema and throat tightness
Thyroid nodule, bilateral cervical lymph nodes, subcutaneous nodules
Total thyroidectomy, bilateral functional type lymphadenectomy, CCRT
NER at 3 mon
Iyamu I, 2015
51
30/M
Neck mass
Left thyroid to isthmus, left level IV LN, chest, abdomen, pelvis, and bone
Total thyroidectomy, bilateral cervical ND, CCRT
Died
Hanamura, 2015
52
46/M
Right thyroid nodule 6 mon
Lower part of the right lobe, lung metastasis
Total thyroidectomy with right MRND, RT, chemotherapy (lung meta)
After 13 mon lung meta, 22 mon lung meta
Zhang, 2015
53
37/F
Right neck mass
Right thyroid lobe lower portion
Right thyroid lobectomy
NER at 6 mon
54
38/M
Hoarseness for 2 mon
Right inferior thyroid lobe tumor with trachea deviation to left
Right thyroid lobectomy, MRND
NER at 26 mon
55
29/F
Neck mass for 7 mon
Middle-to-lower portion of right thyroid and isthmus, extended into surrounding soft tissue
Total thyroidectomy, radical ND
NER at 42 mon
Liu SM, 2016
56
67/F
Hoarseness and easy choking for 2 yr
Left lower neck compressing the trachea, invaded to the tracheal wall and focally infiltrated into the thyroid
Partial tracheotomy with excision of a 4.0 cm tumor
NER at 12 mon
Marini A, 2016
57
76/M
Dyspnea and severe cough for 20 days, dysphagia and cervical pain
Sternoclavicular joints to the upper borders of the thyroid gland. The mass was surrounding the trachea anterolaterally displacing it to the left and the right common artery to the right, a fracture of the first tracheal ring
en bloc tumour resection with total thyroidectomy and a regional lymph node dissection, tracheostomy
-
Tomohiro, 2014
58
52/F
Severe dyspnea, bloody sputum, and neck mass for 6 mon
Thyroid tumor invaded the trachea, obstructing 90% of the tracheal lumen
Tracheostomy, thyroidectomy, the length of the resected trachea was 6 cm, clamshell thoracotomy, end-to-end bronchial anastomosis, gastrostomy, RT
After operation 11 mon lung and bone recurrences, after diagnosis 14 mon died of pleural metastasis
Kyu Young, 2014
59
27/M
Palpable neck mass for 2 mon
Right level IIa tumor, right thyroid lobe multinodular goiter
Excision of the mass along with 6 right level IIa lymph nodes, right MRND, ipsilateral thyroid lobectomy
NER at 3 yrs after 2nd operation
Chris Lominska, 2017
60
60/M
Fatigue, dysphonia, and bilateral upper extremity weakness for 3 yrs
Left thyroid tumor encasing the left RLN and was shaved off the nerve and the trachea
Total thyroidectomy with central neck dissection, CCRT
Left medialization thyroplasty 1 yr later (left vocal palsy), NER at 3 yr after RT
TaeUk Cheon, 2019
61
58/F
Hoarseness for 1 mon
Right lower lobe of the thyroid gland to the right supraclavicular fossa, invasion of the right RLN, right vagus nerve, right internal jugular vein, and right innominate artery, central and right lateral cervical lymph nodes, metastatic nodules in both lungs
Total thyroidectomy, right selective ND (II-VI) +chemotherapy
NER at 4 yr and right vocal cord palsy
Diana, 2019
62
58/M
Progressive anterior neck swelling for 3 year hoarseness, SOB, and hemoptysis for 1 month
1. Left neck tumor from the C7/T1 to the T2/T3 vertebral level, with trachea invasion and left retrosternal extension 2. Left supraclavicular mass
Left hemithyroidectomy, curative resection, and tracheostomy, CCRT
NER at 6 mon