
Abstract
Clinically, it may be very difficult to differentiate between benign branchial cleft cyst (BCC) and malignant BCC with papillary carcinoma preoperatively. Radiological features were reviewed retrospectively between benign BCC and malignant BCC with papillary carcinoma using computed tomography (CT) and magnetic resonance (MR) images. All patients had only a mass on the right upper lateral neck without lesion in the thyroid gland. Two patients had a mass in the upper medial part of BCC on CT images and one patient showed a well-circumscribed mass in the upper portion of BCC on MR image. Two patients received BCC removal only and one patient underwent total thyroidectomy including removal of BCC. As results, most cases of papillary carcinoma in the BCC were detected incidentally after surgical resection of BCC. However, we can differentiate between benign BCC and malignant BCC with primary papillary carcinoma by carefully reviewing radiologic images before surgery.
Introduction
Cystic mass in the lateral neck is generally considered as a benign mass such as branchial cleft cyst (BCC). Based on computed tomography (CT) appearances, BCC could be differentiated from various cystic neck masses including metastatic lymphadenopathy. Various means of differentiating these cystic masses largely depend on the location in the neck, displacement of adjacent structures, and characteristics of the cyst itself. 1 -3 A carcinoma in the cystic mass is almost always a manifestation of cervical metastases from squamous cell carcinoma of head and neck or thyroid papillary carcinomas. A metastatic lymph node from thyroid carcinoma is frequently changed to cystic degeneration, very similar to a benign cervical cyst. 4,5 Thus, initial evaluation for patient presenting with a cystic neck mass should include identification of thyroid cancer. Detailed evaluation of other head and neck regions including endoscopic examination should also be performed. 5
Branchial cleft cyst in adult patients may cause diagnostic dilemma on whether it contains carcinoma or not before surgery. Although carcinoma arising from the BCC is very rare, it is very difficult to distinguish between a benign and a malignant BCC with papillary carcinoma or between a primary lesion and a metastatic lesion in BCC. Diagnosis in most cases is incidental after surgical resection. It is also very difficult to differentiate between them in the absence of primary lesion of the thyroid gland. 6,7 Fine needle aspiration cytology under ultrasound guidance may be valuable for proper sampling from solid part of the cyst. 8 In recent years, CT and magnetic resonance (MR) images have been shown to be of great value in evaluating solid and cystic neck masses. Reviewing radiologic images in detail may be useful to differentiate benign BCC from malignant cystic lesions preoperatively. Therefore, the objective of this study was to retrospectively review CT and MR images of patients with papillary carcinoma of the BCC and compare radiologic features between benign BCC and malignant lesions in BCC.
Patients
A 42-year-old man visited our department with a 6-month history of palpable mass in the right lateral aspect of the neck. He had no past history of surgery or trauma in the head or neck. On physical examination, a firm and nontender mass was palpable in the right lateral neck. It was measured at 4 cm × 5 cm in size at the level of the cricoid cartilage without associated cervical lymphadenopathy (Figure 1A and B). On CT images, a single cystic mass was identified on the upper lateral neck without other cervical lymphadenopathy in either side of the neck. The patient was initially diagnosed with presumed benign BCC with some granuloma in the cystic wall. The patient underwent simple excision of BCC. Intraoperative findings included a 4 cm × 5 cm-sized dark brown fluid-filled cystic mass lateral to the internal jugular vein without cyst rupture at the time of operation. On permanent section biopsy, histopathologic examination was cystic lesion with lymphocytic infiltration. A papillary carcinoma was noted in a BCC. After surgery, we reviewed enhanced CT images and found a single lesion that was hyper-echoic in the upper portion of BCC. After the surgery, ultrasonographic study every 6 months revealed normal thyroid absolutely without any evidence of malignancy. The patient is being followed up with disease-free status for 8 years after the surgery.
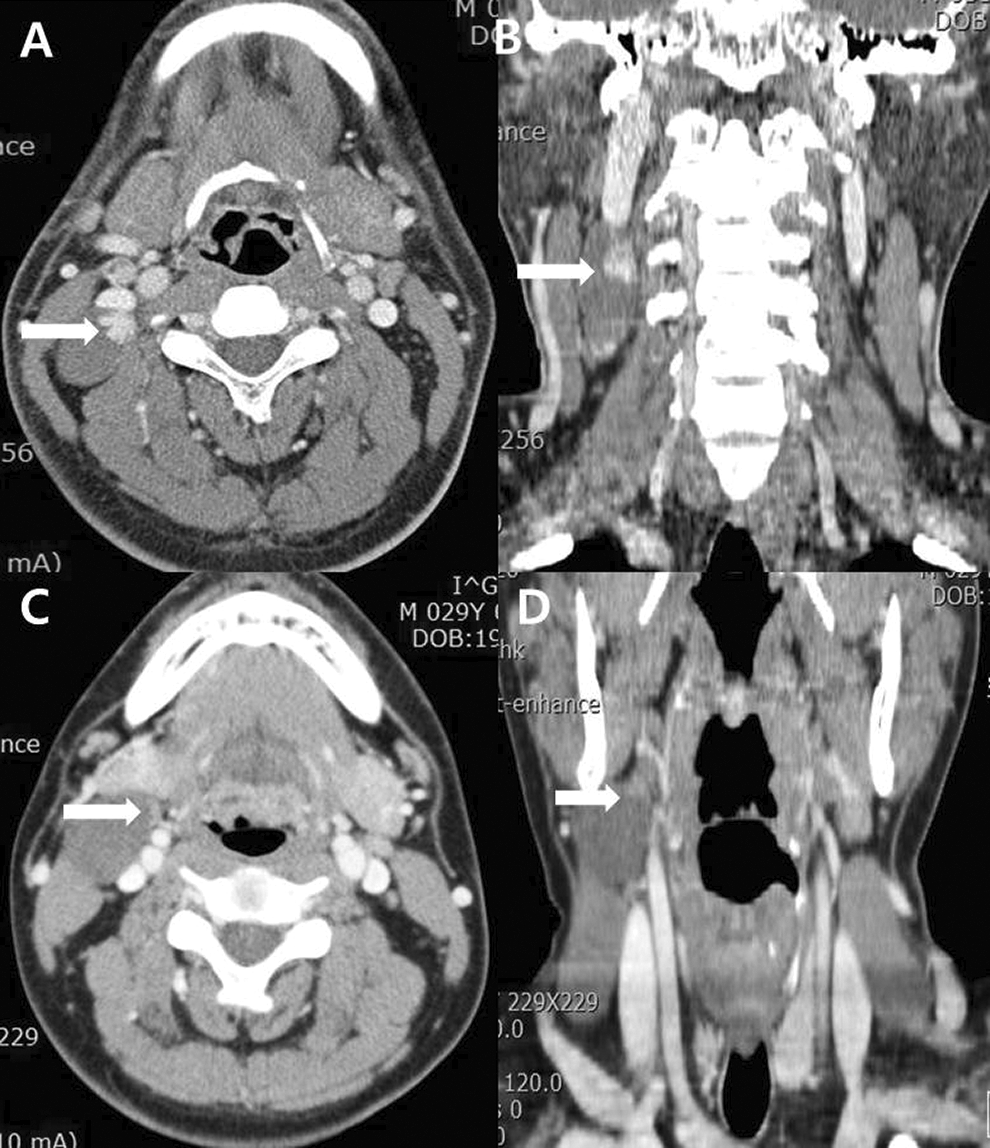
Axial (A and C) and coronal (B and D) CT images showing a single cystic mass on the upper lateral neck without other cervical lymphadenopathy in either side of the neck. Arrows stand for a single hyperechoic lesion in the upper portion of BCC. BCC indicates branchial cleft cyst; CT, computed tomography.
A 29-year-old man also had a palpable mass in the upper right neck for 3 months. On physical examination, a soft and nontender mass of 3 cm × 4 cm size was palpable without abnormal findings in the thyroid gland on ultrasonography (Figure 1C and D). The patient was initially diagnosed with presumed benign BCC. He underwent simple excision of BCC. Intraoperative findings included a dark brown fluid-filled cystic mass lateral to the internal jugular. Histopathologic examination was typical cystic lesion with lymphocytic infiltration. A papillary carcinoma was noted in the wall of the BCC. We also reviewed enhanced CT images after surgery and found a single lesion that was hyper-echoic in the upper portion of BCC. The patient is being followed up with disease-free status for 6 years after the surgery.
A 43-year-old man visited our hospital with an incidental detection of palpable mass in the right lateral neck measuring at 3 cm × 4 cm in size. The patient underwent spine magnetic resonance imaging (MRI) due to cervical spine disease. Magnetic resonance imaging of the patient demonstrated a 1.6 cm × 3.0 cm × 1.8 cm sized well-circumscribed cystic mass in the right lateral aspect of the neck at level II (Figure 2A). Intracystic solid component with intermediate signal intensity was found in the upper pole of the cystic mass. On ultrasonic images, there were small multiple thyroid goiters without suspicious malignancy. We performed simple excision of BCC. There were typical cystic lesion (Figure 2B) and a papillary carcinoma in the wall of the BCC (Figure 3). We performed total thyroidectomy and histopathologic results were multiple nodular hyperplasia without evidence of malignancy. The patient is being followed up with thyroid hormone replacement and disease-free status for 4 years after the surgery.
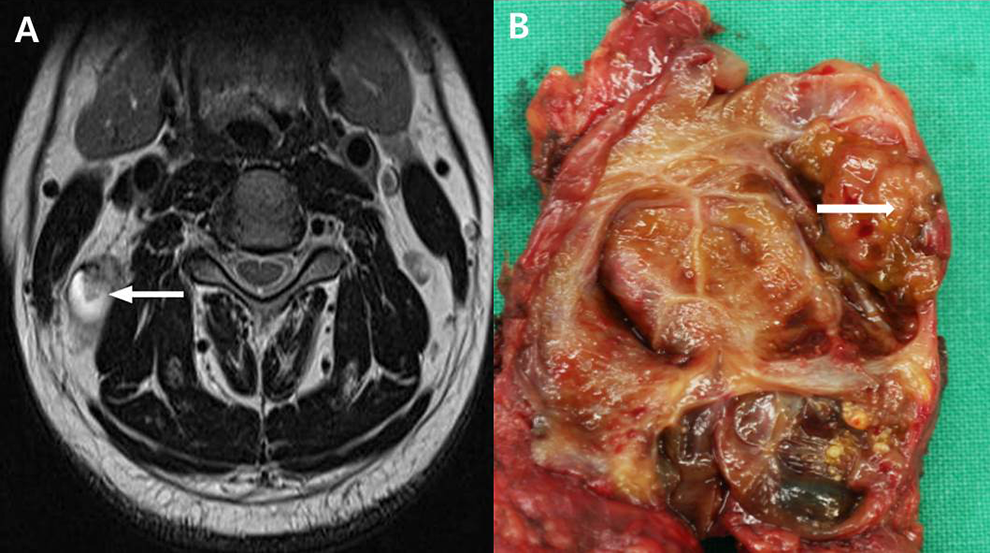
A, Axial T2-weighted spin-echo images showing a cystic mass adjacent to the carotid space anteriorly and the sternocleidomastoid muscle laterally. The intracystic solid component of intermediate signal intensity (arrow) measuring at about 0.8 cm in diameter (A) is obviously identified. It is located anteromedially in the cyst. Excised surgical specimen (B) showing an irregular margined mass in the cyst (arrow).
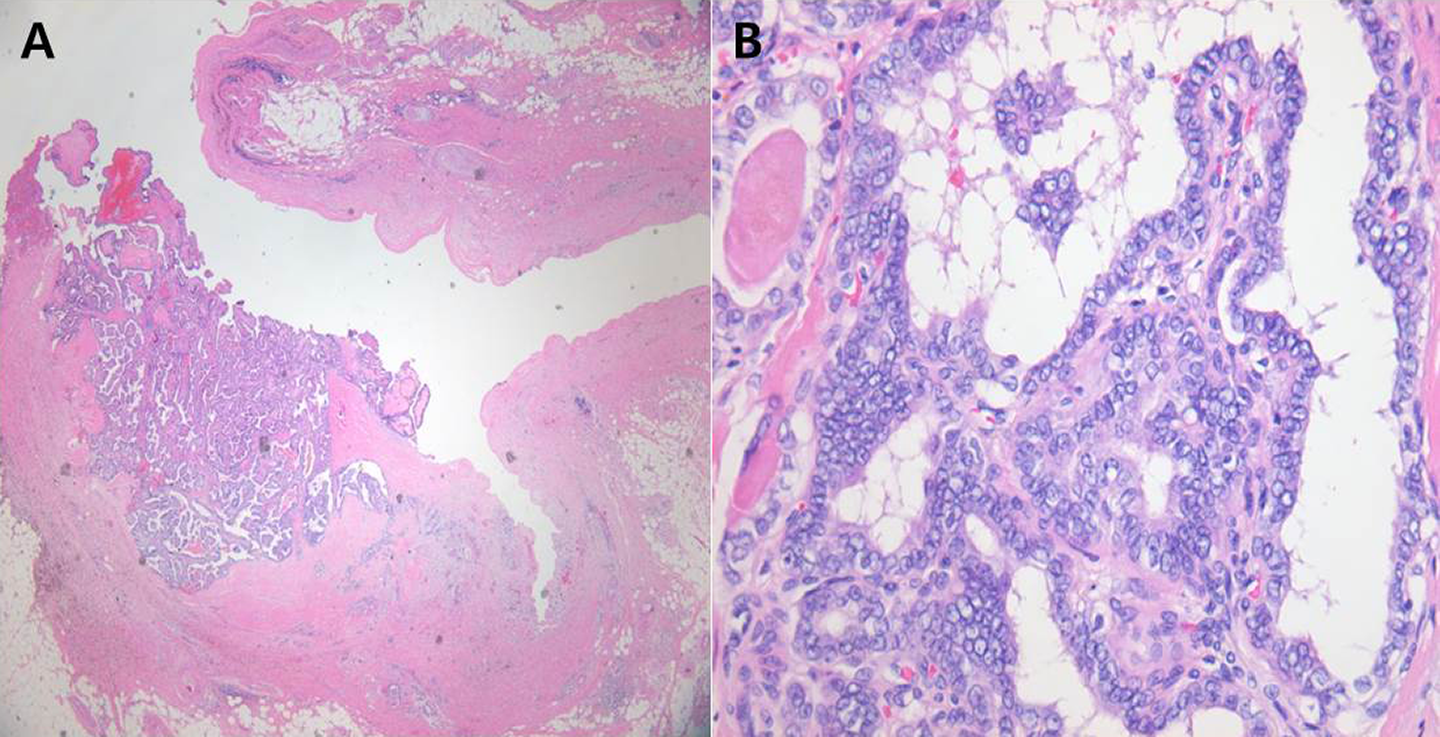
Intracystic papillary projection suggesting papillary carcinoma originated from a branchial cleft cyst at 8 mm in size (A, H&E, ×20). Typical papillary carcinoma (B, H&E ×400). H&E indicates hematoxylin and eosin.
Discussion
The second BCC accounts for 95% of branchial anomalies and most patients in the young adult population have been performed surgical excision without suspicion of the existence of a carcinoma within the cyst. A papillary carcinoma in the BCC is extremely rare. It is very difficult to distinguish between a benign BCC and a malignant BCC preoperatively. Most cases are detected incidentally after surgical resection of BCC. On CT images, benign BCC is typically well-circumscribed, homogeneously hypoattenuating, and unilocular cystic lesion. On MRI, BCC can be T1 hypointense to intermediate intensity relative to muscle and typically T2 hyperintense. Mural thickness, the degree of cyst wall enhancement, complexity of the lesion, and adjacent soft-tissue edema all depend on the extent of associated inflammation or infection. Metastatic squamous cell lymph nodes can have an appearance similar to second branchial cleft cysts. There is a propensity for such cystic lymph nodes in cases of tonsillar carcinoma and/or human papillomavirus-related squamous cell carcinomas.
Because papillary carcinoma of the BCC is also cystic in radiologic images, all lining walls of the cyst must be carefully reviewed. In our cases, after carefully reviewing the lining wall of the cyst, we found an isolated and solitary lesion with irregular margins in BCC. Interestingly all cases showed malignant lesions located on the upper portion of BCC. This location is the distal end of the second branchial cleft that is obliterated. We could not explain why malignant lesions are located in this area. In addition, when papillary carcinoma is found in the BCC, primary carcinoma needs to be differentiated from ectopic thyroid and metastatic carcinoma from thyroid gland in the BCC. 5 The most frequent site of ectopic thyroids is the thyroglossal remnant in the base of tongue. However, whether ectopic thyroid tissues in the BCC are extremely rare remains controversial. 9 Sidhu et al 3 have suggested the following criteria for primary papillary carcinoma in BCC: (1) an epithelial lining layer or subepithelial lymphoid tissue collection, (2) normal thyroid tissue adjacent to the focus of papillary carcinoma within the wall, and (3) no evidence of papillary carcinoma in the thyroid or other area.
In our study, all patients of papillary carcinoma in the BCC showed no primary lesion of the thyroid gland. They might have developed in ectopic thyroid tissues in BCC because there was no normal thyroid tissue adjacent to the papillary carcinoma within the wall. The ectopic thyroid tissue within the cyst might have been replaced by papillary carcinoma. Interestingly, they all had a single lesion in the upper part of the BCC. There are 2 options to obtain optimal treatment for papillary carcinoma in the BCC: (1) removal of BCC with careful follow-up, and (2) removal of BCC with total thyroidectomy. When there is no malignancy in the thyroid gland regardless of metastatic focus, there is no consensus for determining the extent of surgery such as total thyroidectomy. If the surgeon has the philosophy not performing total thyroidectomy in the absence of thyroid cancer, a detailed evaluation of head and neck region and thyroid gland is needed after simple excision of BCC. Papillary carcinoma arising in the branchial remnant has ability to metastasize to regional lymph nodes. This has been found in 20% of cases. 8 Regular and meticulous imaging studies should be performed for such cases.
In conclusion, it is very difficult to distinguish a benign BCC and a malignant BCC preoperatively. Most cases are detected incidentally after surgical resection of BCC. A solitary cystic mass in the lateral neck may be the only initial presenting symptom of papillary carcinoma in the BCC. Thus, all lining walls of the cyst should be carefully reviewed so that benign BCC might be differentiated from malignant BCC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.