
Abstract
Neurosynovial tumors, originating from Schwann cells within nerve sheaths, are benign entities, with 25% to 45% manifesting in the head and neck region. However, occurrences in the pterygopalatine fossa (PPF) are exceptionally rare, and only a handful of cases have been documented. In this report, we present the unique case of a 6-year-old child exhibiting a sizable soft tissue mass in the left PPF, extending into the inferior orbital fissure. The patient underwent successful intranasal endoscopic removal of PPF schwannoma utilizing the prelacrimal recess approach, with postoperative pathology confirming the diagnosis of schwannoma. Schwannomas within the PPF are particularly uncommon, and instances of such tumors in pediatric patients are even more exceptional. This case highlights the diagnostic and therapeutic challenges associated with PPF schwannomas in children, emphasizing the significance of a multidisciplinary approach for optimal management. In addition, a comprehensive literature review is presented to provide insights into the existing knowledge on this rare entity, further contributing to the understanding of pediatric PPF schwannomas.
Introduction
Neurosynovial tumors, arising from Schwann cells within nerve sheaths, represent benign entities with a distribution spanning the entire body. Notably, 25% to 45% of cases are localized to the head and neck regions.1,2 Remarkably uncommon, these tumors, comprising less than 4% of occurrences, may manifest within the nasal cavity, sinuses, and the intricately confined pterygopalatine fossa (PPF). 3 Among neurosynovial tumors, vestibular neurosynovial tumors predominate, followed by trigeminal neurosynovial tumors. 4
The PPF is a narrow, inverted, conical gap that poses clinical accessibility challenges due to its intricate anatomy. Functioning as a pivotal conduit between the orbit, middle cranial fossa, oral and nasal cavities, and the infratemporal fossa, it serves as a potential anatomical pathway for the dissemination of head and neck tumors. Tumors within the PPF can exert influence on adjacent regions. 5
Tumors originating in or involving the PPF are exceptionally rare, constituting merely 0.5% of all head and neck tumors. 6 Primary tumors in the PPF, especially PPF schwannoma, are even more elusive. 7 A thorough exploration of the pertinent literature underscores the scarcity of documented cases of PPF schwannoma, with an especially limited number involving pediatric patients. This scarcity highlights the uniqueness and clinical significance of our reported case.
Case Report
A 6-year-old child presented to the ophthalmology clinic at Wuhan Union Hospital with a recent physical examination indicating reduced vision in the left eye accompanied by a central dark spot. The patient reported experiencing decreased vision in the left eye for 1.5 months, along with the discovery of an orbital mass in the same eye persisting for 1 month. There was no history of trauma, sinus, or dental symptoms. Following thorough imaging tests, the patient was referred to the head and neck surgery department for further evaluation and management.
A paranasal sinus and orbit computed tomography (CT) scan unveiled a rounded hypodense shadow occupying the left PPF-superior orbital fissure, measuring approximately 45 mm × 33 mm × 40 mm, with a CT value of 37 Hu (Figure 1). Subsequent magnetic resonance imaging (MRI) revealed an expansile soft tissue mass in the inferior orbital fissure of the left PPF, displaying iso-intensity signals in T1-weighted images and hyperintensity signals in T2-weighted images. The mass exhibited a well-defined boundary with a few liquefied necrotic areas, notably enhanced on the MRI scan (Figure 2). The lesion partially extended upward into the left orbit, obscuring the demarcation of the left suborbital rectus muscle. This resulted in compression of intraorbital structures, with the left ophthalmic bulb protruding and partial resorption of the left infraorbital wall. The pressure exerted on the walls of the left maxillary and pterygoid sinuses led to a narrowing of the sinus cavity, along with a slight constriction of the left postnaris and nasopharyngeal cavities. The neurologic origin of the lesion was strongly suspected.
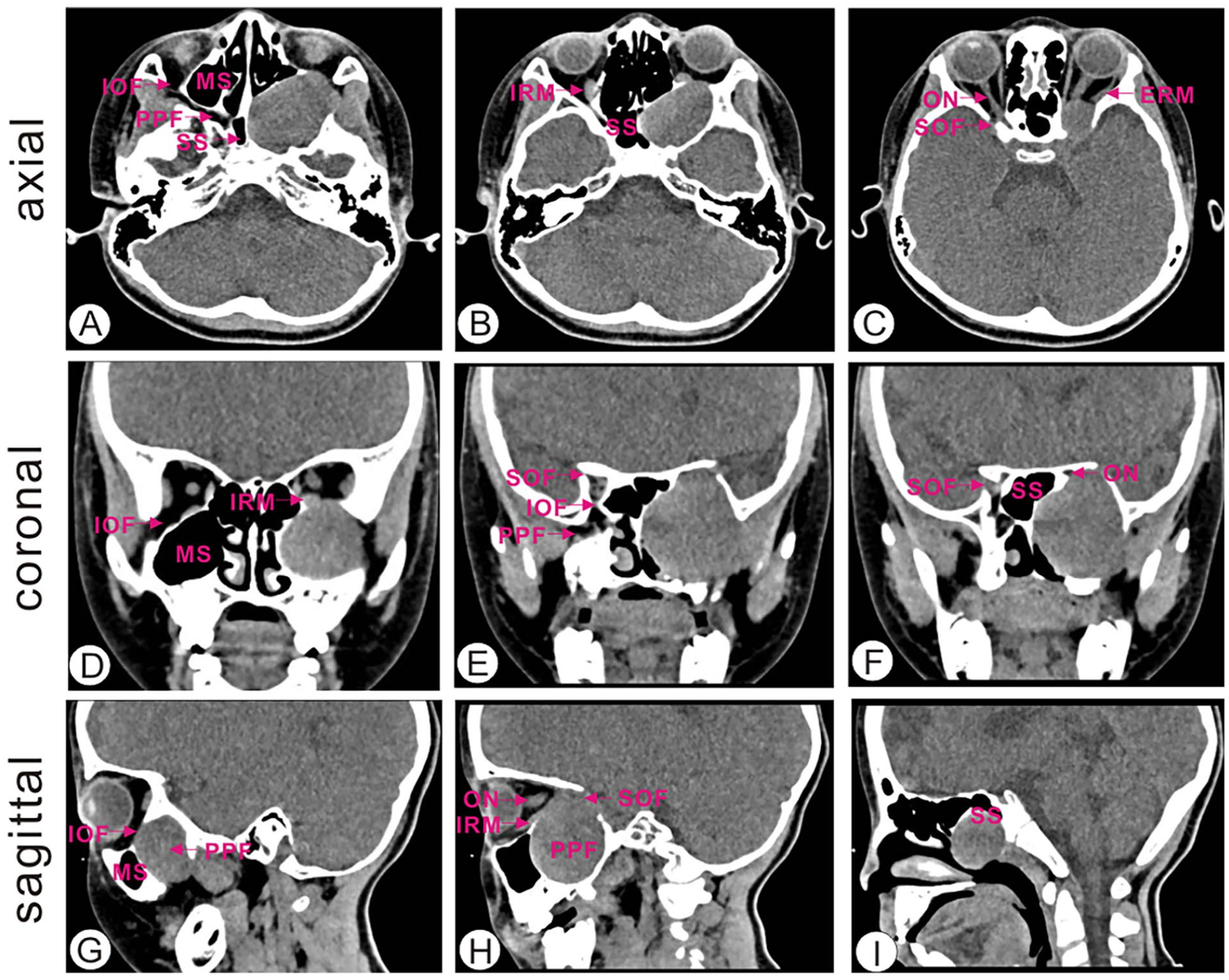
Axial CT scan shows that the lesion protruded upward into the left intraorbital part and involved the supraorbital fissure (A, B, C). Coronal CT scan shows a soft tissue density shadow in the left maxillary sinus and pterygopalatine fossa. The sinus walls of the left maxillary and sphenoid sinuses were compressed and the sinus cavities narrowed (D, E, F). Sagittal CT scan reveals a circular low-density shadow with a size of about 45 mm × 33 mm × 40 mm in the left pterygopalatine fossa-supraorbital fissure (G, H, I). MS, maxillary sinus; PPF, pterygopalatine fossa; SS, sphenoid sinus; IOF, inferior orbital fissure; IRM, inferior rectus muscle; ON, optical nerve; SOF, superior orbital nerve; ERM, extrinsic rectus muscle.
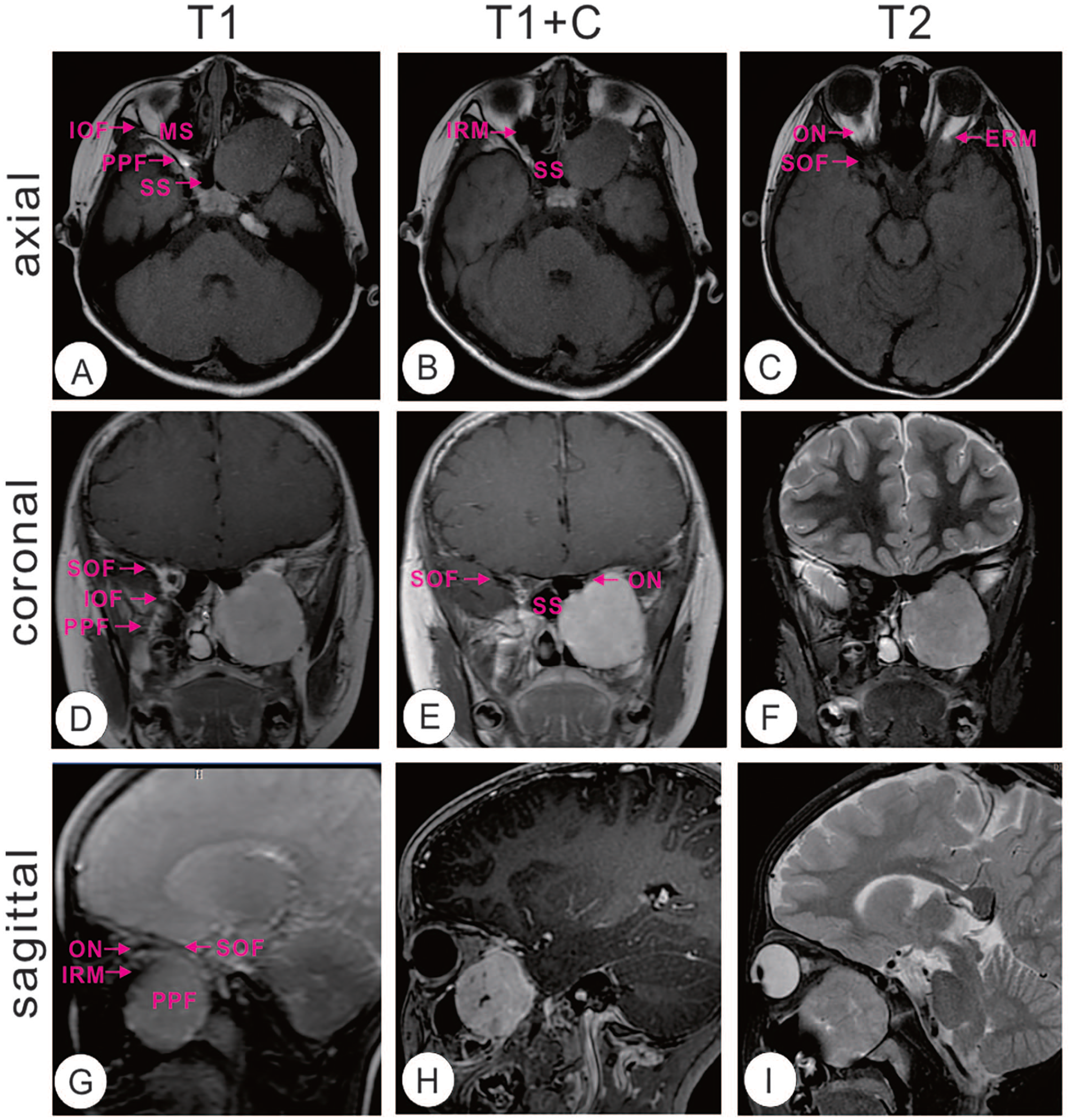
Axial MRI showed that the boundary between the lesion and the inferior rectus muscle of the left eye was not clear, the intraorbital structure was compressed and pushed (A, B, C). Coronal MRI shows a few liquefaction necrotic areas in it, and the mass was significantly enhanced after enhancement (D, E, F). Sagittal MRI reveals an expansile soft tissue mass in the inferior orbital fissure of the left PPF, displaying iso-intensity signals in T1-weighted images and hyperintensity signals in T2-weighted images (G, H, I).
Under general anesthesia, the patient underwent intranasal endoscopic removal of the PPF schwannoma through the prelacrimal recess approach. The operator carefully removed the fractured left inferior turbinate fracture under nasal endoscopy to ensure a clear surgical path and complete resection of the lesion. Postoperative histopathology confirmed a schwannoma in the left nasal sinus. Immunohistochemical staining revealed positive expressions for S100 (+), SOX10 (+), and Ki67 (LI: <5%). The patient experienced a smooth recovery without any neurological deficits and did not report specific nasal or sinus symptoms postoperatively, such as congestion, runny nose, or loss of sense of smell. Vision loss was significantly improved during recovery. A comprehensive 2 year follow-up showed the patient’s satisfaction with no signs of recurrence.
Discussion
Schwannomas can occur in any region of the body, yet their occurrence in the nasal cavity, sinuses, and PPF is exceedingly rare, accounting for less than 4% of cases. 3 While the highest incidence typically occurs between the age range of 20 and 50, these tumors can emerge at any age, including in young children, displaying no gender or racial preference. Verocay’s 1910 groundbreaking work established the neural ectodermal Schwann cell origin of neurosynovial tumors within cranial, peripheral, and autonomic nerve sheaths. Given their solitary and benign nature, lymph node metastasis and distant metastases are uncommon.8-10
The relatively inert and generally benign nature of schwannomas often conceals symptoms during the early stages. Patients may delay seeking medical attention until the tumor reaches a significant size, resulting in symptoms arising from compression. The presentation of symptoms varies depending on the site of compression. Diagnosis involves a combination of radiological examinations for the initial localization of the mass and histopathological examinations for the final diagnosis. On CT scan, PPF schwannomas typically appear as well-defined, homogeneous soft tissue masses. Definitive diagnosis, however, relies on histopathological examination, revealing Antoni A and Antoni B portions. The Antoni A portions exhibit compact spindle cells, while the Antoni B portions are characterized by hypocellular myxoid regions, with cells arranged in short and interlacing fascicles. Immunohistochemical staining reveals that tumor cells express positivity for S100, a finding consistent with this case. Ki-67, recognized as a cell proliferation marker, is widely supported by most studies for its predictive and survival prognostic value.11-13 In this particular case, the Ki-67 index is notably low in benign schwannoma, measuring less than 1% to 5%. This finding signifies a low level of mitotic activity within the tumor, contributing to a more favorable prognosis.
On reviewing the literature spanning from 1980 to the present day, it was revealed that the earliest documented age for a PPF schwannoma is 7 years. The patient in question presented with a gradual onset of right nasal obstruction, right exophthalmos, and a decline in right visual acuity. 14 Schwannomas are exceptionally rare in the PPF, and cases of nerve sheath tumors in the PPF occurring in children are even scarcer. The total number of reported PPF schwannoma cases is limited, not exceeding 40, with only a handful of cases documented in Chinese patients across 4 reports in the English literature.15-18 Specifically, only 4 cases involving children (age <18 years) with PPF schwannoma were reported (Table 1).14,15,19,20 Large schwannomas exceeding 50 mm in size within the PPF are uncommon. To the best of our knowledge, this investigative report marks the first instance involving the youngest patient, a critical contribution to the exploration of PPF schwannomas in the pediatric population.
Clinical Characteristics of Published Cases of Pediatric Pterygopalatine Fossa Schwannomas.
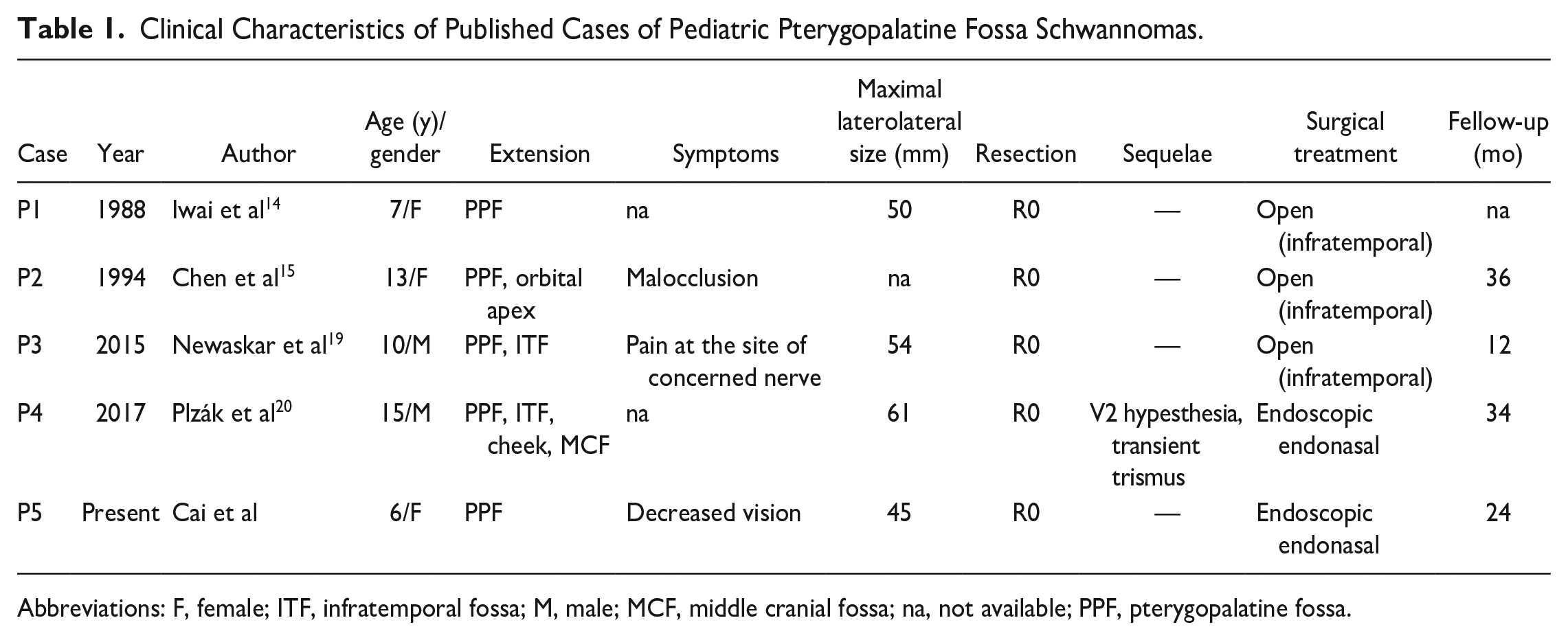
Abbreviations: F, female; ITF, infratemporal fossa; M, male; MCF, middle cranial fossa; na, not available; PPF, pterygopalatine fossa.
The primary treatment approach for benign PPF schwannoma involves comprehensive surgical resection. This approach, encompassing both the tumor and surrounding normal tissues, proves beneficial in minimizing the recurrence of PPF nerve sheath tumors. Traditional open surgeries utilizing lateral approaches (infratemporal fossa, transcervical) and anterior approaches (Caldwell-Luc, Weber-Fergusson) have been conventionally employed for this purpose. 21 The choice of a specific approach and surgical method is contingent on factors such as the size and location of the tumor. In this case, the patient underwent a fully intranasal endoscopic removal of the PPF schwannoma using the prelacrimal recess approach. This technique is renowned for its minimally invasive nature, aiming to preserve the surrounding structures of the tumor. Remarkably, this meticulous approach did not result in recurrence during the 2 years of postoperative follow-up.
In addition, beyond surgical resection, radiation therapy emerges as an alternative treatment option. Various radiation therapy approaches, including stereotactic radiosurgery, stereotactic radiotherapy, and proton beam therapy, are employed to arrest tumor growth and minimize the risk to adjacent structures. However, it is not the primary choice for patients with larger tumors and notable compression symptoms. 22
Conclusion
Schwannomas, as per current literature, can manifest at any age, and our case review has identified the youngest documented patient, a 6-year-old girl. Utilizing the intranasal endoscopic removal approach through the prelacrimal recess not only provides an optimal visualization but also ensures the protection of vessels and nerves within the PPF, ensuring a secure tumor resection of the schwannoma. Notably, this approach is not limited to schwannomas and holds potential applicability to other PPF lesions; however, further data and additional patient cases are required to validate its effectiveness. While the risk of postoperative recurrence is low, regular follow-up remains crucial. This study serves as a valuable reference for guiding the treatment of PPF schwannoma in the pediatric population.
Footnotes
Author Contributions
TZ, YT, and LQZ designed and supervised the work. AQR and HC drafted the manuscript. HC and ZYZ conceived and designed the report. JXY, YJW, MZZ, and TZ diagnosed, treated, and followed the patients, and participated in the collection of clinical data. All authors have read and approved the final version of this manuscript.
Data Availability
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the National Natural Science Foundation of China (82201301, CH), Natural Science Foundation of Hubei Province (2022CFB087, ZT), the Research Grant of Union Hospital, Tongji Medical College, HUST (F016.02004.21003.126, ZT), and Open Project of Key Laboratory of Molecular Imaging (2022fzyx015, TZ).