
Abstract
Hemangiomas are rare and benign tumors originating from the pterygopalatine fossa (PPF). In this study, we report a rare case of PPF hemangioma in a 66-year-old male, for which he underwent surgical resection via the anterior nasolacrimal recess after preoperative arteria maxillaris embolization. To enhance our understanding on this rare condition, we conducted a comprehensive review of existing literature on this disease to discuss its clinical characteristics, differential diagnoses, and potential treatment approaches.
Keywords
Introduction
Hemangiomas are rare benign tumors originating from the pterygopalatine fossa (PPF). Given their rare occurrence and surgically difficult-to-access anatomical location of occurrence, studying hemangiomas in the PPF can provide valuable insights into their clinical presentation, diagnostic challenges, and treatment strategies. In this study, we report a rare case of a PPF hemangioma and conduct a literature review from PubMed Central to elucidate the associated characteristics and treatment modalities for PPF-derived hemangiomas, which can lead to advancements in patient care and the optimization of treatment outcomes for individuals afflicted by such rare condition.
Method
Case Description
A 66-year-old woman presented at the Otorhinolaryngology Outpatient Department of our hospital with a chief complaint of right facial numbness for the past year.
After admission, the patient underwent several examinations. Computed tomography (CT) scanning detected an oval nodule in the right palatine fossa (Figure 1A-C), enhanced magnetic resonance imaging (MRI) revealed an abnormal oval signal shadow (approximate size, 2.3 × 1.8 cm) displaying increased signal intensity on T2-weighted imaging, lipid-pressure imaging and diffusion-weighted imaging, and contrast enhancement resulted in the progressive enhancement of the lesion (Figure 1D-F).
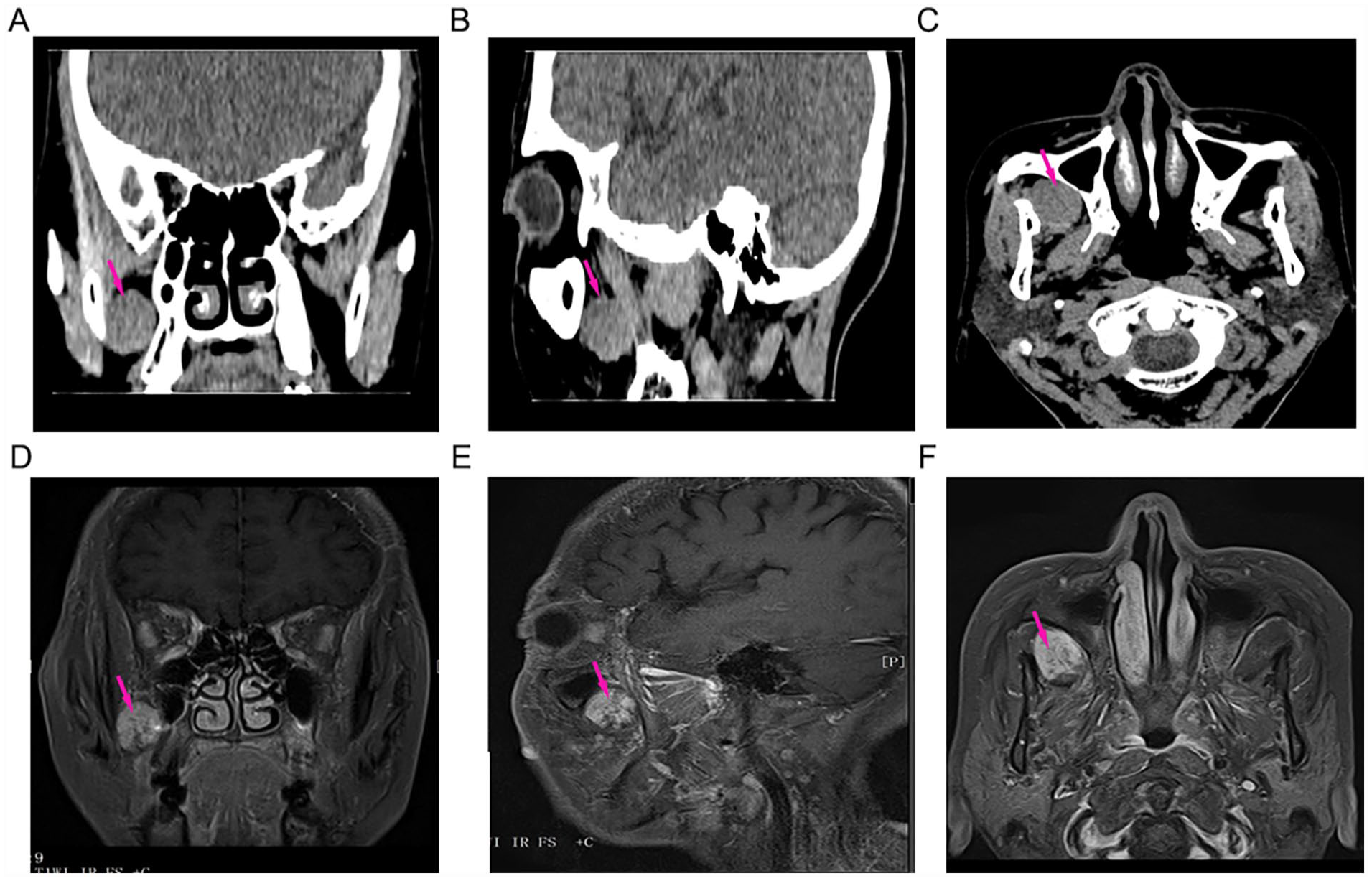
Radiological evaluation of the right palatine fossa hemangioma. (A-C) CT and (D-F) Enhanced MRI showing oval nodules with smooth margins in the right palatine fossa measuring approximately 2.3 cm × 1.8 cm. CT, computed tomography; MRI, magnetic resonance imaging.
After team discussion, surgical resection of the hemangioma was performed to alleviate the patient’s facial numbness, which was preceded by embolization of the maxillary artery via femoral artery puncture using the Seldinger method. Briefly, a 5F arterial sheath was introduced to facilitate the insertion of a 5F single-bent catheter into the right maxillary artery. Angiography showed arterial thickening in the right maxillary branch, with areas of blood supply displaying dispersed sheet staining (Figure 2A). Subsequently, distal vascular embolization was performed using 2 ml of embolization microspheres, which resulted in a substantial reduction in the preoperative prominence of blood vessels (Figure 2B). The procedure involved the expansion of the anterior lacrimal recess to access the maxillary sinus cavity, followed by the incision of the posterior lateral wall mucosa of the maxillary sinus, exposing the bone wall, PPF, and subtemporal fossa. Low-temperature plasma assistance was also employed, and the lesion was completely excised (Figure 3).
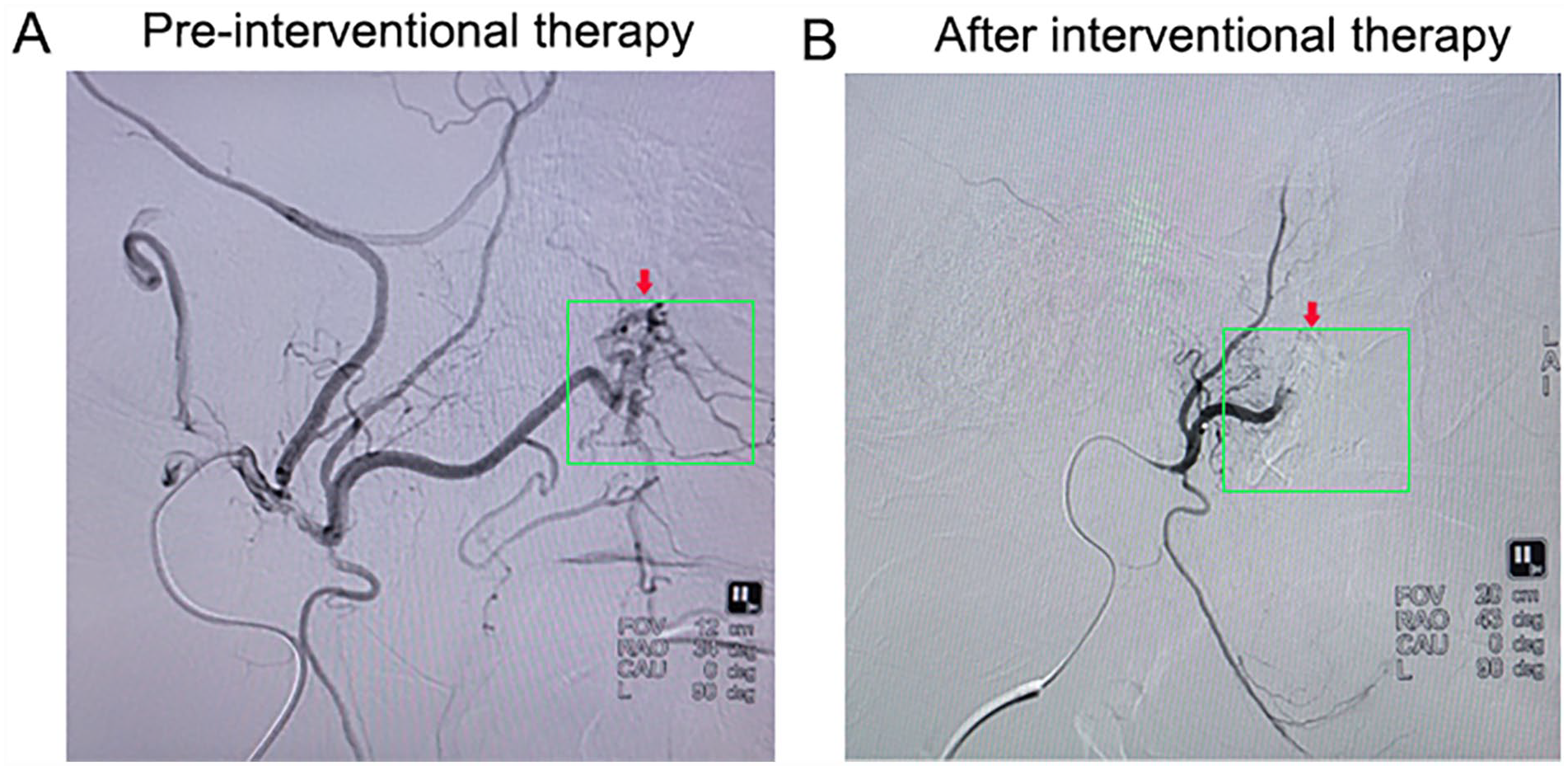
Angiographic assessment of maxillary artery and postoperative outcome. (A) Angiography demonstrating arterial thickening in the right maxillary branch, with scattered sheet staining indicating blood supply. (B) Postoperative angiography showing a significant reduction in focal vessels.
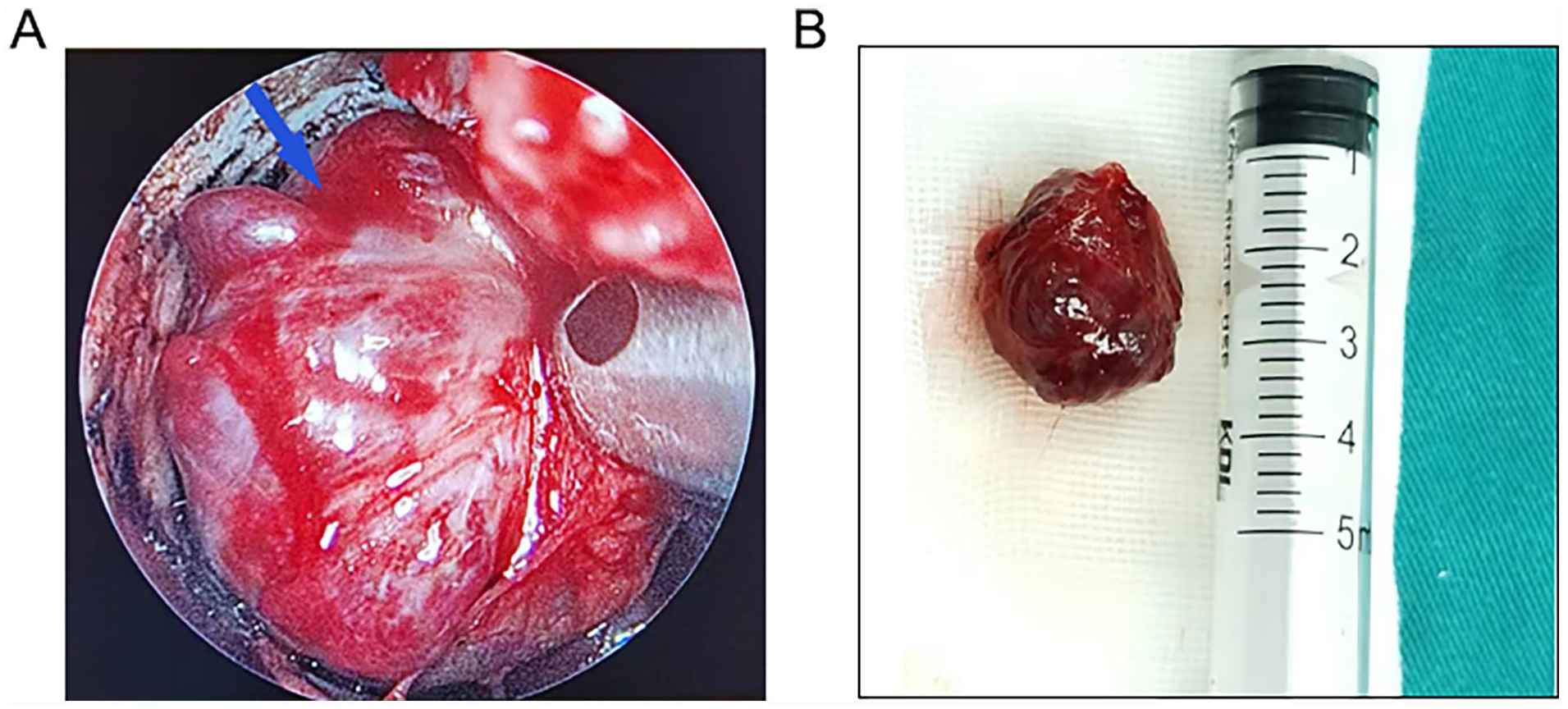
Intraoperative visualization and resection of pterygopalatine fossa hemangioma. (A) Intraoperative view showing the tumor within the pterygopalatine fossa. (B) Complete resection of the tumor and final dimensions of 2.5 cm × 2.5 cm × 1.8 cm on postoperative pathological report.
Intraoperative frozen biopsy results revealed the absence of malignant tumor cells within the PPF mass, and subsequent postoperative pathological examinations confirmed the diagnosis of hemangioma (Figure 4). After the surgery, the patient had an uneventful recovery and did not experience any symptoms such as transient V2 numbness or dry eye.
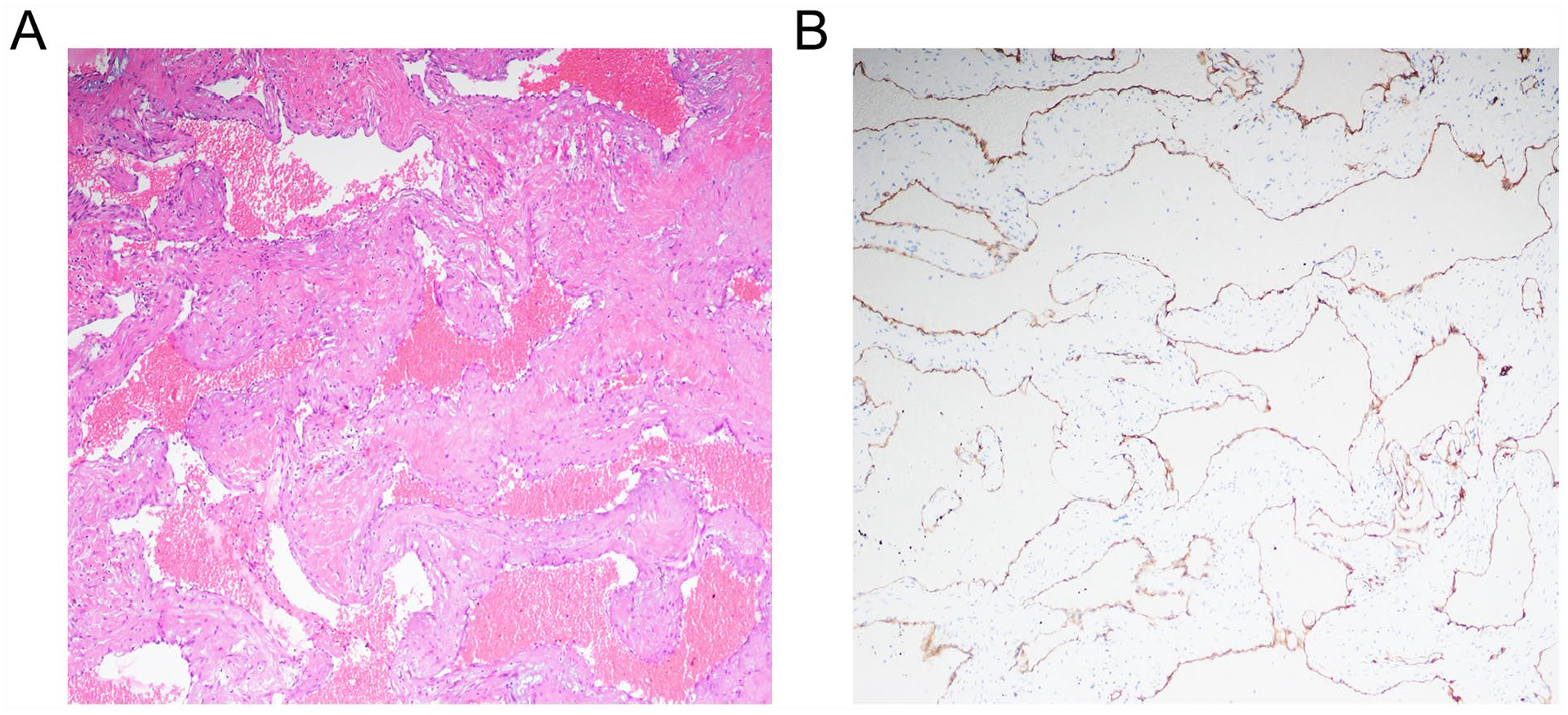
Histological examination and immunohistochemistry of hemangioma. (A) Hematoxylin and eosin staining at ×200 original magnification. (B) Immunohistochemistry revealing elevated CD34 expression in the hemangioma tissue.
Discussion
Hemangiomas are benign vascular tumors commonly found in the head and neck region, and their occurrence in the PPF is quite rare. The PPF is a pyramid-shaped bony space deep within the facial structures, located between the maxilla, palatine bone, and the pterygoid process of the sphenoid bone. 1 This anatomical region contains essential structures such as the pterygopalatine ganglion and the maxillary nerve and its branches, as well as the pterygopalatine segment branches of the maxillary artery. 2 A unique characteristic of PPF is its absence of glands and lymph nodes. As a result, tumors occurring in the PPF are typically a result of direct invasion by peripheral tumors, with primary or metastatic tumors rarely observed in this location within clinical practice. 3
CT imaging was performed to assess the extent of bone destruction surrounding the tumor. Additionally, MRI was conducted to visualize fat within the PPF and bone marrow at the skull base, following fat inhibition via T-imaging. This method proved valuable in evaluating the tumor’s extent of invasion, including its impact on surrounding soft tissues, the orbital apex, nerves, and dura mater. More specifically, a comprehensive assessment of the involvement of important surrounding nerves, such as the pterygoid nerve, the second maxillary nerve, and the third maxillary nerve, is important prior to surgery because such tumors may often exhibit growth patterns along the pterygoid nerve. Clinically, the evaluation should also encompass determining whether the tumor has extended into the cavernous sinus and has an effect on the descending palatine nerve. In cases where the descending palatine nerve is involved, partial removal of the hard palate may become necessary. Furthermore, vigilance is required to detect any signs of orbital involvement through the infraorbital fissure and potential intracranial expansion of the tumor.
Tumors originating in the PPF continue to present significant challenges for otolaryngologists due to their deep location and proximity to critical arteries and cranial nerves. Thus, achieving the safe and complete removal of PPF-derived tumors remains surgically complex and challenging. Traditionally, various lateral approaches have been utilized in the management of PPF tumors, including transcervical, transoral, mandibular swing, transparotid, transmastoid, and infratemporal fossa approaches. 4 In 1996, Kamel reported a case involving the resection of a nasopharyngeal angiofibroma using the maxillary sinus approach. 5 Subsequently, in 2003, Alfieri et al conducted a systematic investigation into the treatment of PPF tumors through approaches involving the middle nasal passage, lower nasal passage, and maxillary sinus and reported the efficacy of the nasal endoscopic approach as a surgical method for resecting PPF tumors. 6 This marked a significant advancement in the field, as such an approach offers the advantage of reducing the incidence of functional and cosmetic morbidity associated with open approaches when managing lesions within the upper PPF. 7
The utilization of nasal endoscopy via the anterior nasolacrimal recess offers several noteworthy advantages. For instance, this contributes to the reduction in operative time, minimizes trauma to the patient, and results in shorter hospital stays. 8 Furthermore, the nasal endoscopic approach has been shown to reduce the risks of postoperative complications, 9 ultimately contributing to improving patient outcomes and overall quality of life. 10
Given the propensity of giant PPF tumors to exhibit high vascularity, often accompanied by multiple large feeder vessels, it is important to recognize the potential for significant hemorrhage during biopsy and resection in the absence of adequate preoperative investigations and precautions. Therefore, to mitigate the risk of hemorrhage, it is strongly recommended to perform preoperative embolization, a measure aimed at reducing the likelihood of hemorrhagic complications.
Conclusion
In conclusion, hemangiomas originating in the PPF are benign and uncommon tumors. In this case report, we presented the case of a patient who underwent successful complete removal of a hemangioma from the PPF via the anterior nasolacrimal recess approach in conjunction with preoperative embolization of the maxillary artery.
Footnotes
Availability of Data and Materials
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by Research Grant for Health Science and Technology of Pudong Health Bureau of Shanghai (Grant No. PW2020B-10), Pudong New Area Clinical Characteristic Discipline (Grant No. PWYts2021-15), Young Medical Talents Training Program of Pudong Health Bureau of Shanghai (Grant No. PWRq2021-06), and Subject Construction Project of Pudong Health Committee of Shanghai (Grant No. PWZy2020-06).
Ethics Approval
This project’s protocol was approved by the Ethics Committee in Shanghai Pudong Gongli Hospital.
Statement of Informed Consent
This article has obtained written informed consent from patients for their anonymized information to be published in this article.