
Abstract
Liposarcoma is extremely rare in the parotid gland. In this article, we report the case of an 87-year-old man who presented to our department with swelling in the left parotid region. Magnetic resonance imaging (MRI) revealed a tumor in the superficial lobe of the parotid gland. Total parotidectomy and ipsilateral lymph node dissection were performed. Histologic examination confirmed the diagnosis of myxoid liposarcoma of the parotid gland. On imaging, there was no evidence of nodal or distant metastasis. Radiation therapy was planned, but the patient refused to receive treatment. After a follow-up of 3 years, MRI showed no sign of tumor recurrence and the patient remained symptom-free. The case is original by the tumor’s location. Only 8 cases of primary parotid liposarcoma have been reported in the literature. The purpose of this article was to discuss, through our case, clinical and anatomopathological features of parotid gland liposarcomas as well as its treatment options and prognosis.
Introduction
Liposarcoma is the most common type of sarcoma in adults, 1 representing 20% of all soft tissue malignancies.1,2 It usually arises in the deep soft tissue of the lower extremity, particularly the thigh. 3 In the head and neck region, liposarcoma is extremely rare and only a few cases have been reported in the literature. 1 Among major salivary glands, the parotid gland is the most frequent site for liposarcoma. 3 Only 8 cases of primary parotid liposarcoma have been reported. As for cases of liposarcomas metastasizing to the parotid gland, the primary tumor was located in the thigh.4-6
In this article, we report a case of primary myxoid liposarcoma in an unusual anatomic site.
The purpose of this article was to discuss, through our case, clinical and anatomopathological features of parotid gland liposarcomas as well as its treatment options and prognosis.
Case Report
An 87-year-old male patient, with no medical history, presented with painless swelling in the left parotid region that developed over the past 3 months.
Physical examination revealed a firm, regularly-shaped swelling, located in the left parotid region. On palpation, it was firm, painless, fixed to the underlying structures, and measuring 4 cm with normal overlying skin. Facial movements were normal on examination. Intraoral and cutaneous examinations were unremarkable. No cervical lymphadenopathy was palpated. Magnetic resonance imaging (MRI) revealed a tumor occupying the superficial lobe of the left parotid gland (Figure 1). It had regular margins and was measuring 4 cm. The tumor was heterogeneous with high signal intensity on T1- and T2-weighted images. It had also areas showing an intermediate signal on T1-weighted images and hyposignal on T2-weighted images.
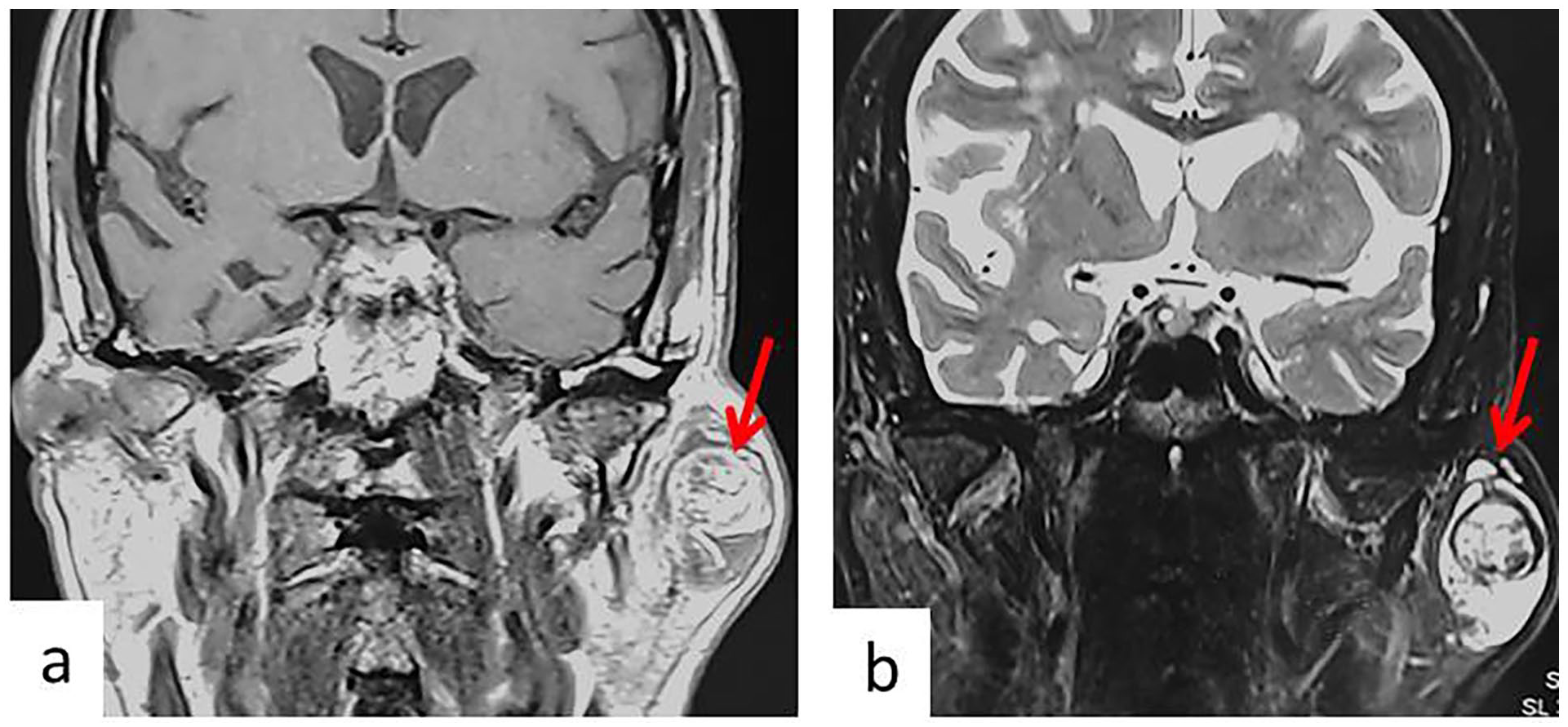
MRI of the parotid gland with frontal (a) T1 section and (b) T2 section, showing a tumor occupying the superficial lobe of the left parotid gland. It has regular margins. The tumor (red arrow) is heterogeneous with high signal intensity on T1- and T2-weighted images. It has also areas of intermediate signal on T1-weighted images and hyposignal on T2-weighted images.
A left superficial parotidectomy was conducted. On frozen section examination, it was a malignant tumor. Excision of the deep lobe and ipsilateral lymph node dissection (level II-IV) were performed (the patient provided informed consent before surgery). After surgery, the patient developed a transient facial palsy.
Histologic examination confirmed the diagnosis of myxoid liposarcoma of the parotid gland (Figure 2). It showed a proliferation of fusiform cells, lipoblasts, and myxoid stroma.
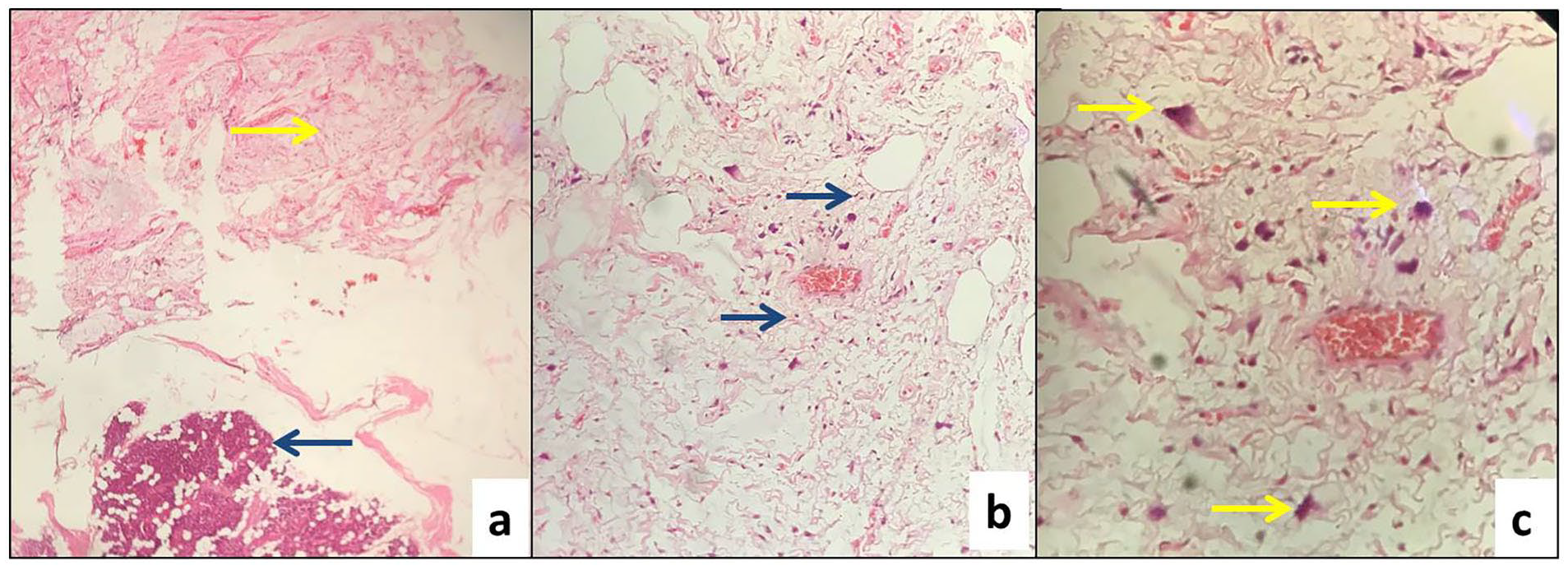
(a) Proliferation of malignant tumor cell (yellow arrow); normal parotid parenchyma (blue arrow); HE× 10. (b) Fusiform cells (blue arrow) surrounded by myxoid stroma; HE× 20. (c) Lipoblasts showing atypical and hyperchromatic nuclei (yellow arrow); HE× 40. HE, hematoxylin and eosin.
The tumor measured 5 cm. It had negative surgical margins and did not have any extraparotid extension. Vascular invasion and perineural spread were not recorded and lymph nodes were negative. On imaging, there was no evidence of nodal or distant metastasis. Radiation therapy was planned at the multidisciplinary consultation meeting, but the patient refused to receive further treatment.
After a follow-up of 3 years, MRI showed no sign of tumor recurrence and the patient remained symptom-free.
Discussion
The physiopathology of liposarcomas is not well understood, as well as the genetic mutations leading to this tumor. 7 Risk factors of liposarcoma according to the American Cancer Society were: radiation therapy, some family cancer syndromes, damage to the lymphatic system, and exposure to toxic chemicals. 7 Recent studies do not support the theory about lipomas degenerating into liposarcomas. 3
According to the World Health Organization, liposarcomas are divided into 5 major histological subtypes: well-differentiated, dedifferentiated, myxoid, round cell, and pleomorphic. 8 The histologic subtypes of the reported cases occurring in the parotid gland included: pleomorphic liposarcoma (in 3 cases), myxoid liposarcoma (in 3 cases including our case), well-differentiated liposarcoma (in 1 case), and dedifferentiated liposarcoma (in 1 case). In 1 case, the histologic subtype was not identified. Table 1 resumes the characteristics of the reported cases.
Characteristics of the Reported Parotid Gland Liposarcomas.
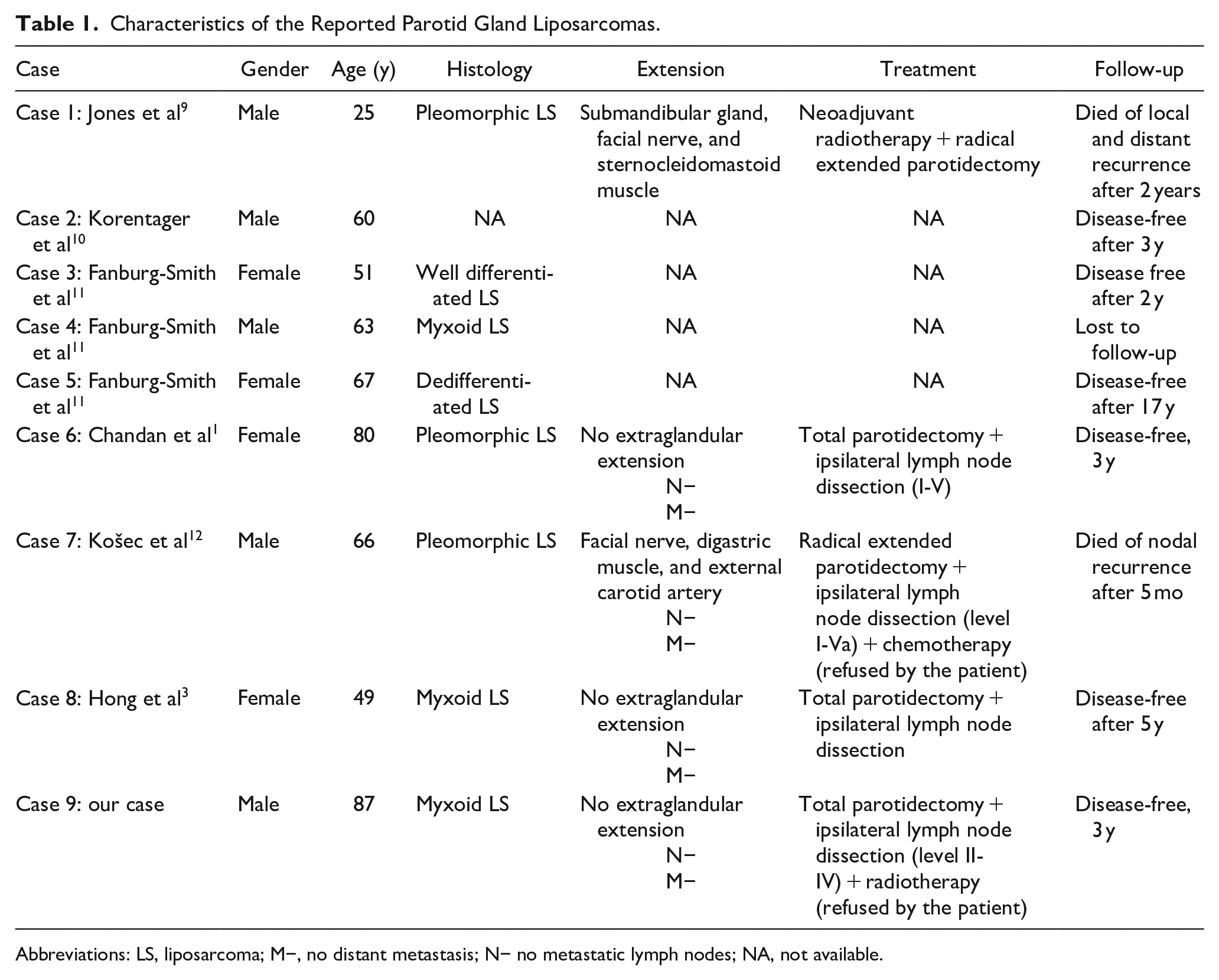
Abbreviations: LS, liposarcoma; M−, no distant metastasis; N− no metastatic lymph nodes; NA, not available.
The myxoid subtype represents 35% to 40% of all liposarcomas.1,3 Myxoid liposarcoma is composed of round to oval-shaped nonlipogenic mesenchymal cells and small signet ring lipoblasts in a prominent myxoid stroma with a characteristic branching vascular pattern. 3 Cytology is not a helpful diagnostic tool for liposarcomas. 3 Therefore, histologic examination should be performed. 3
In some cases when the diagnosis of liposarcomas is difficult, immunohistochemistry can be useful in identifying the tumor’s histological type. 3 In sarcomas, cells are positive for vimentin and S-100, and they are negative for CK, CK7, EMA, and HMB45. 3
The clinical presentation of liposarcomas depends on the localization of the tumor and it is usually similar to other primary cancers arising in the same site. 7 Liposarcoma of the parotid gland usually presents as a swelling in the parotid region with no characteristic features on clinical examination. 3
In liposarcoma, MRI is a highly reliable and sensitive method to identify the tumor. 12 Well-differentiated liposarcomas are characterized by a high-fat content showing a high-intensity signal. 3 However, when the fat content of the tumor is low, it may not show the typical characteristics of a lipomatous tumor making the diagnosis of a liposarcoma more difficult. 6 Findings in MRI depend on the amount of myxoid component and necrosis, the cellularity, and the vascularity of these tumors. 3 The myxoid subtype usually appears as a tumor showing high-signal-intensity foci representing the fat within the tumor. 3 In our case, the tumor was heterogeneous with high signal intensity on T1- and T2-weighted images. On computed tomography (CT) scan, calcifications within the tumor can be seen. 12 CT is also useful for detecting an extension to bone structures. 12
To diagnose a primary myxoid liposarcoma of the parotid gland, a metastasis of cutaneous or mucosal liposarcoma must be excluded.1,3,12 Furthermore, it must have the appearance of a tumor originating from the parotid gland rather than a tumor invading the gland.1,3,12 Also, the diagnosis of a mixed tumor (carcinosarcoma) must be excluded.1,3,12
Liposarcomas can metastasize to bone and soft tissues. 3 In a study including 169 patients, sites of metastases were: soft tissue (84%), lung (68%), abdomen (48%), solid organ (48%), bone (45%), lymph nodes (32%), and retroperitoneal space (29%). 13
The treatment of choice for myxoid liposarcoma of the salivary gland is wide-margin surgical excision with removal of the entire tumor.3,12 Excision margins should be at least 2 cm from the palpable tumor margin to avoid leaving microscopic residual disease behind. 12 Our patient had surgery. Negative margins were achieved.
In liposarcoma, radiation therapy may be a valuable complement to surgery. 7 Postoperative radiotherapy can be done in case of high-grade tumors (pleomorphic, dedifferentiated, and high-grade myxoid liposarcoma), positive margins, locally advanced tumors, and complex anatomic subsites, such as the head and neck region.3,12 In our case, radiation therapy was planned, but the patient refused to receive further treatment.
Liposarcoma’s response to chemotherapy is not well documented. 7 Doxorubicin and ifosfamide have shown low responses limited to 20%. 12 Postoperative chemotherapy could be advantageous in high-grade tumors. 12 In the case of inoperable tumors, chemotherapy and radiation therapy can be considered. 3
In liposarcoma, the prognosis seems to be related to the histologic subtype, size, site, and stage of the tumor. 12 Among the reported cases of parotid liposarcoma, only 2 patients developed recurrence.
In the literature, the overall 5 year survival rate for liposarcoma was between 20% and 50%. 12 For myxoid liposarcoma, 5 year survival ranged from 47% to 77%. 1 In fact, in comparison to well-differentiated liposarcoma, myxoid and pleomorphic liposarcoma had a higher percentage of recurrence (up to 80%). 1 If discovered at an early stage and treated correctly, the prognosis of myxoid liposarcoma of the salivary gland is usually good. 3 Our patient had a 5 cm liposarcoma, with negative surgical margins and no extraparotid extension. He did not have any nodal or distant metastasis. After surgery, he was free of disease.
Conclusion
Liposarcoma is the most common mesenchymal tumor and is commonly located in the lower extremity. 3 The parotid gland is a very unusual site for liposarcoma. 1 On physical examination, this entity can mimic other tumors. 7 On MRI, it can exhibit characteristic features. 12 Histological examination combined with immunochemistry is an important tool to obtain the diagnosis. 3 Because liposarcoma of the parotid gland is extremely rare, there is limited research and data available on its treatment and prognosis. This condition is usually treated by surgery.3,12 Chemotherapy and radiotherapy can be considered in treating this disease. 3 The prognostic is related to the histologic subtype, size, site, and stage of the tumor. 12
Footnotes
Acknowledgements
None.
Data Availability
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.