
Abstract
Undifferentiated small round cell sarcoma is an extremely rare and highly aggressive tumor touching the soft tissues and bones. Here, we report the case of a 7-month-old girl who presented to our department with respiratory distress due to a hypopharyngeal mass causing airway obstruction. The patient underwent a tracheotomy and had a direct laryngoscopy. Histological examination confirmed the diagnosis of an undifferentiated small round cell sarcoma. The patient received chemotherapy and radiotherapy and underwent neck dissection. One year later, the patient was diagnosed with local recurrence as well as metastatic cervical nodes and liver and pulmonary metastases. The case is original by the tumor’s location and the age of onset. To the best of our knowledge, this could be the first case in English and French literature reporting an undifferentiated small round cell sarcoma affecting the hypopharynx among infants. The purpose of this article is to report our case and discuss its clinical and anatomopathological features as well as its prognosis and treatment options.
Keywords
Introduction
Undifferentiated small round cell sarcomas (USRCSs) are extremely rare sarcomas that mainly affect soft tissues and bones. 1
Compared to other sarcomas, they have a poorer prognosis and tend to have a bad response to treatment. 1
Because USRCSs share similar morphological features to Ewing’s sarcoma (ES), they are often considered as Ewing-like sarcoma (ELS) and are usually treated similarly. 1
In this article, we report a new case of an USRCS in an unusual anatomic site.
To the best of our knowledge, this could be the first pediatric case in English and French literature reporting an URSCS affecting the hypopharynx.
The purpose of this article is to discuss through our case the clinical and anatomopathological features of USRCS as well as its prognosis and its treatment options.
Case report
A 7-month-old female baby presented with respiratory distress at rest lasting for 2 months, becoming severer since 3 days. She also had dysphonia and feeding difficulty.
The baby was born healthy and had appropriate development for her age. The pregnancy had been uncomplicated. She did not have a family history of cancer.
On physical exam, she had upper-airway dyspnea. The oropharyngeal exam was normal. There was no evidence of cervical lymphadenopathy.
Indirect laryngoscopy showed a white nodular mass arising from the right pyriform sinus causing airway obstruction.
Magnetic resonance imaging (MRI) was performed showing a right hypopharyngeal mass measuring 27 -mm × 20 mm × 23 mm extending to the oropharynx and to the supraglottis. It showed intermediate signal on T2-weighted sequence, hyposignal on T1-weighted sequence, and contrast enhancement (Figure 1).
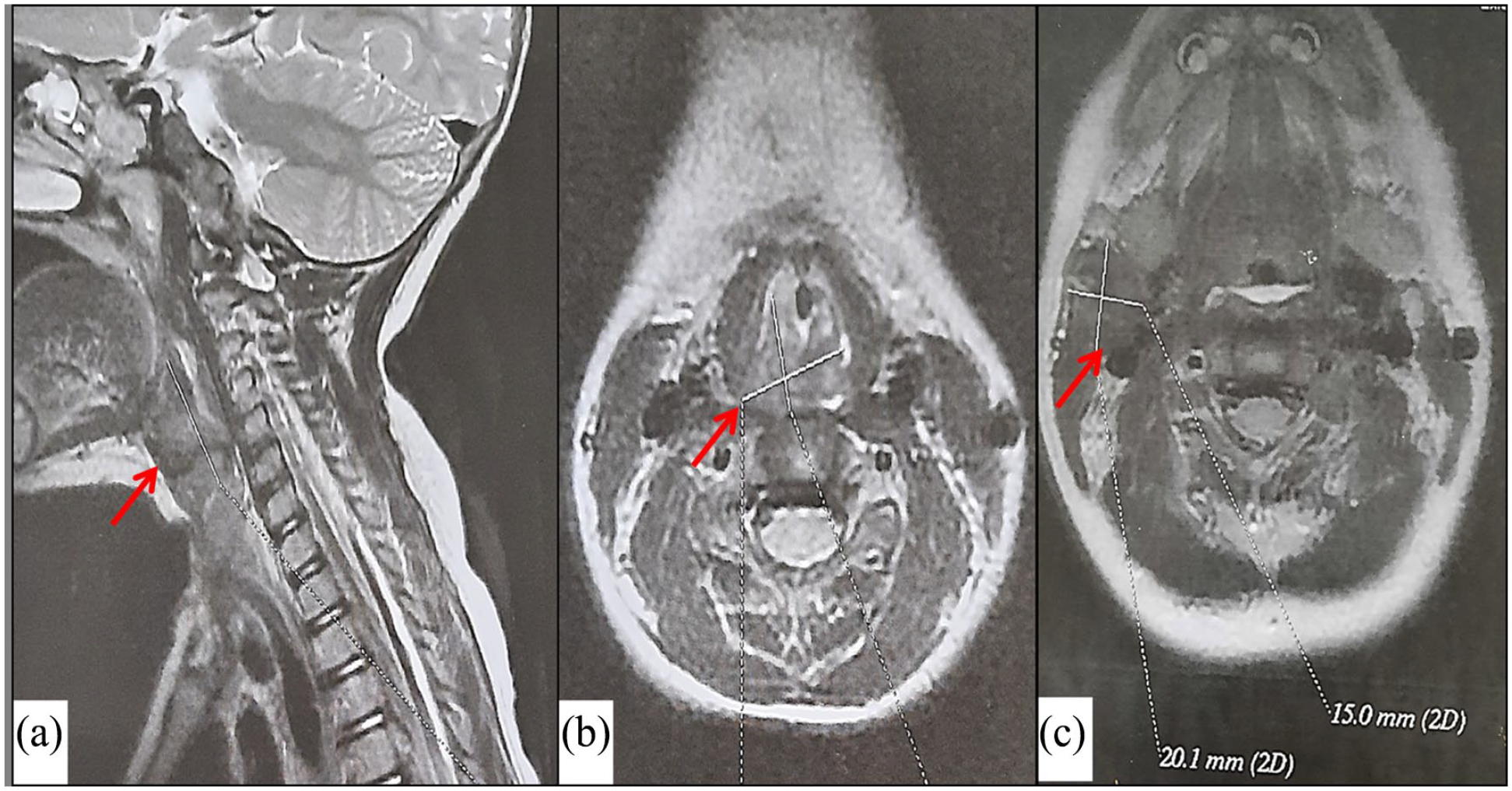
Magnetic resonance imaging of the neck (sagittal section (a), axial section (b and c)) shows a right hypopharyngeal mass, on intermediate signal on T2-weighted sequence, extending to the oropharynx and to the supraglottis. It also shows a right cervical lymph node measuring 20 mm × 15 mm (c).
MRI also showed bilateral cervical lymphadenopathy (level II-IV).
During direct laryngoscopy, a biopsy was taken. On histopathological examination, hematoxylin and eosin-stained sections of the tumor showed small round blue cells (Figure 2). The cells had small regular round nuclei and small nucleoli. The tumor had a mitotic rate of 4 mitoses per 10 HPF. It also showed small areas of necrosis and apoptosis.
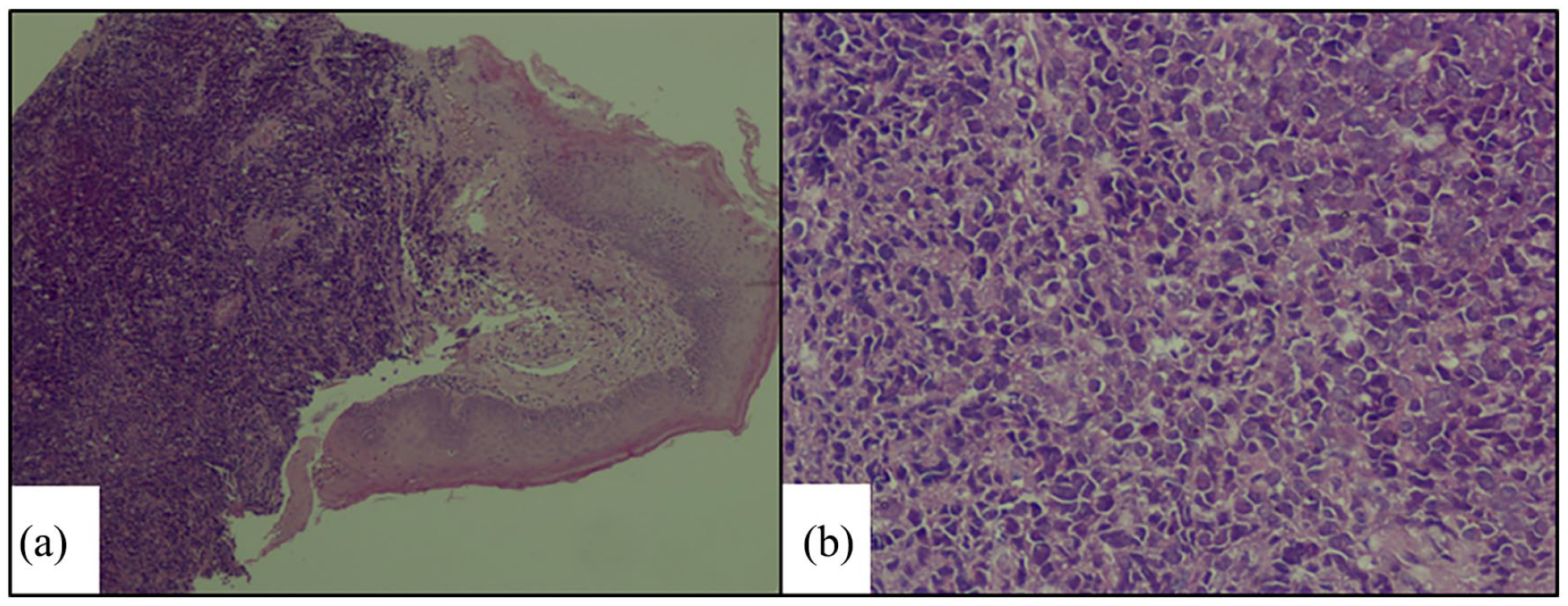
Histopathologic examination of the tumor on hematoxylin and eosin-stained sections shows small round blue cells (HE × 4) (a). The cells had small regular round nuclei and small nucleoli (HE × 20) (b).
Immunohistochemistry was performed and showed a high proliferation index (Ki-67 = 50%).
Moreover, the tumor was negative for neuroendocrine markers (NSE, CD56), synatophysin, lymphoid markers (CD20, CD3, BCL2), and cytokeratin (AE1, AE3). Other markers excluded the diagnosis of lymphoma (CD45, CD79a, CD3, CD5), leukemia (CD34), melanoma (PS100), and carcinoma (EMA). Myogenin, MYOD1, and desmin markers were also negative which made the diagnosis of rhabdomyosarcoma highly unlikely (Figure 3).
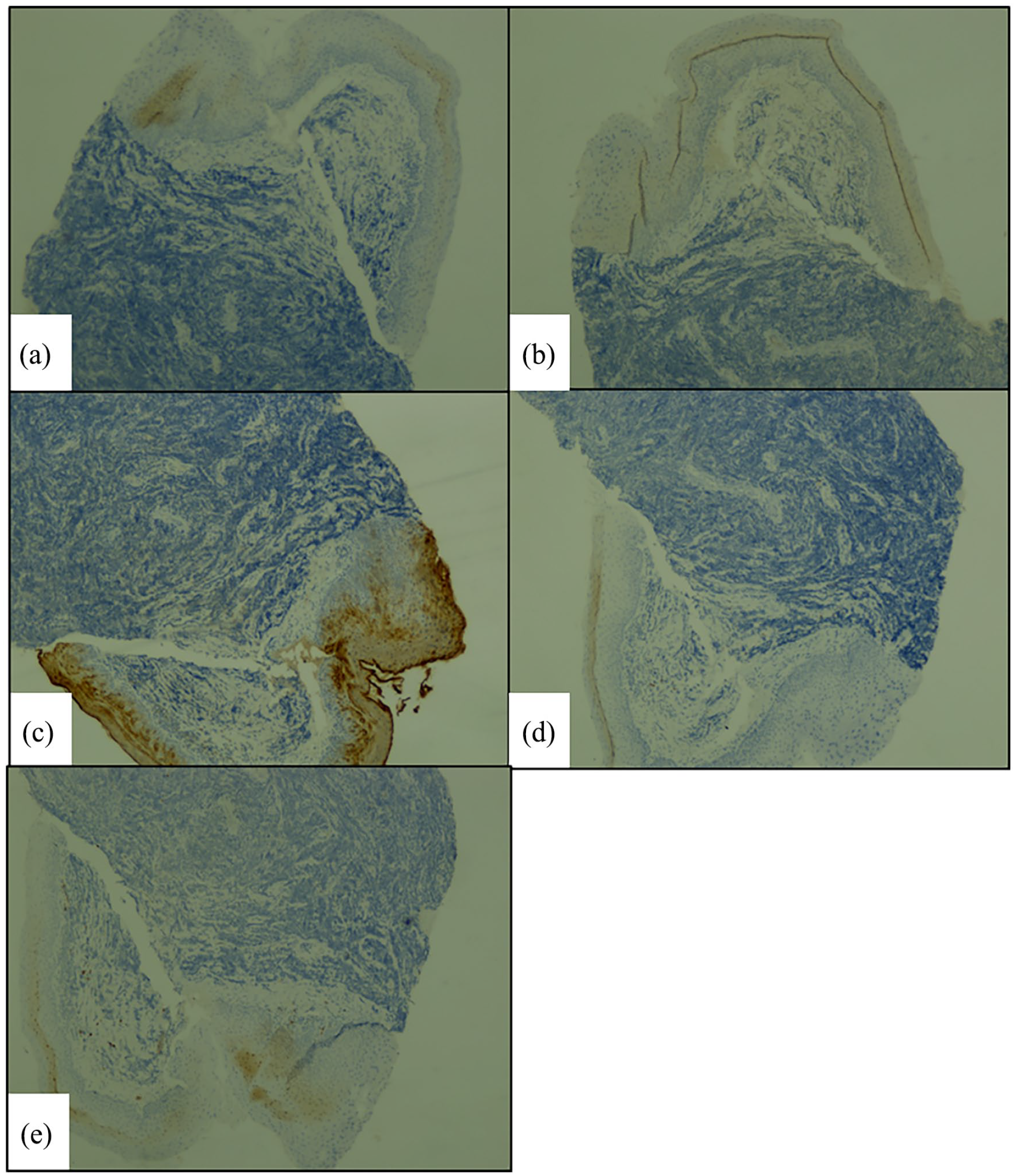
On immunohistochemistry, the tumor stained negatively for synatophysin (a), myogenin (b), EMA (c), desmin (d), and CD79a (e).
The genetic study revealed the tumor to be lacking EWSR1 rearrangement supporting the diagnosis of an USRCS not that of an ES.
The metastatic workup using computed tomography showed bilateral cervical lymphadenopathy (level II). There was no evidence of distant metastases.
A tracheotomy was performed as the tumor was obstructing the airways and the patient could deteriorate.
Treatment was decided at a multidisciplinary consultation meeting. The patient received vincristine, doxorubicin, and cyclophosphamide. Radiation therapy was started after the fifth chemotherapy cycle. The patient received a cumulative dose of 40 Gy. However, as the primary tumor regressed, the lymph nodes did not show any signs of improvement. Therefore, a bilateral lymph node dissection (level I-V) was conducted. The lymph nodes were metastatic of an USRCS.
After 5 months, the tracheotomy was removed as the patient was free of disease.
One year later, the patient was diagnosed with local recurrence as well as metastatic cervical nodes and liver and pulmonary metastases. A tracheotomy was performed again. The patient’s parents refused to receive further treatment and the patient died after 3 months.
Discussion
Small round cell sarcomas are a diverse family of tumors that share a lot of morphological, immunohistological, and clinical similarities. 2
Prior to 2020, these tumors were classified by the WHO classification as either ES or USRCS (also referred as ELS).3,4
USRCS has many features of ES, but lacks fusions between the EWSR1 gene and one of the ETS family of transcription factors, which is known to be a pathognomonic molecular hallmark of ES.4,5
With the evolution of more advanced molecular techniques, new diagnostic categories have come out, including round cell sarcomas with EWSR1 fusion to non-ETS family members, CIC-rearranged sarcomas, and BCOR-rearranged sarcomas.3,6
In our case, the genetic study to identify the USRCS’s subtype was not conducted.
USRCS is a very rare tumor with an incidence rate of 0.1 cases per 100,000. 6
It mainly affects males. 4 It commonly arises in the bones and metastases frequently. 4
USRCS most often occurs in children and young adults but remains rare in this age range compared to rhabdomyosarcoma, especially among infants (age < 1 year). 5
To the authors’ knowledge, aside from our case, the only case involving an infant with USRCS that has been reported in the literature was that of a 2-month-old female diagnosed with an USRCS of the forearm muscles. 7 She had an amputation of the left upper extremity and received chemotherapy. Three months later, the patient died of cerebral metastasis.
Furthermore, what makes our case very unusual is the hypopharyngeal localization that has only been reported once. It was a case of a 50-year-old patient diagnosed with an USRCS in the postcricoid region of the hypopharynx with bilateral cervical metastatic lymph nodes and no distant metastasis. 6 He underwent surgery followed by radiotherapy. Nine months after surgery, the patient was doing fine.
Differential diagnosis of USRCS are mainly ES, rhabdomyosarcoma, small cell osteosarcoma, desmoplastic small round cell tumor, mesenchymal chondrosarcoma, and poorly differentiated round cell synovial sarcoma. 6
Diagnosis of USRCS is extremely difficult because of the nonspecific findings on physical examination, and imaging, and depends only on pathological examination, combining morphology, immunohistology, and molecular techniques. 6
USRCS is characterized by medium round or ovoid cells lacking differentiation. 6
It may express some special markers such as CD56, TLE-1, and Cyclin D1, but not markers of epithelial cells such as CK7, CK5/6, and EMA. 6
URSCS may spread to lymph nodes and can also metastasize to lung and brain which are the most common metastatic sites. 8 Distant metastases usually occur in high-grade undifferentiated tumors. 8
Currently, there is no unified protocol for ELS. Surgery is the best treatment option. 6 The efficacy of chemotherapy and radiotherapy has not been demonstrated though. 6
In our case, surgery was not feasible due to the tumor location. The patient was treated with radiochemotherapy. The primary tumor responded to the treatment but the metastatic lymph node did not show any sign of recovery. Therefore, neck dissection was performed. One year later the patient presented with local, nodal, and distant metastases.
In fact, it was reported that patients with USRCS showed significantly lower survival rates than patients with ES. 4 For high-grade USRCS median survival was less than 2 years. 8
Conclusion
USRCS is a very rare tumor that is commonly located in bones and soft tissues. 4 Among these locations, the hypopharynx is a very unusual site. 6 On clinical examination and imaging, this entity can mimic other tumors. 6 Histological examination combined with immunochemistry and molecular biology is an important tool to obtain the diagnosis. 6 It is also important to use sequencing technologies to recognize subgroups of these tumors. 6 Currently, there is no unified protocol for USRCSs. This condition is usually treated by surgery, chemotherapy, and radiotherapy. 6 Compared to other sarcomas, it tends to have a poor prognosis. 4
Footnotes
Acknowledgements
None.
Data availability statement
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/Consent Statement
Not applicable.
Grant number
Not applicable.
Trial registration
Not applicable.