
Abstract
Retained needles are frequently observed in intravenous drug users. However, an incidental discovery of multiple needles at the neck seldom occurs. These foreign bodies remain either asymptomatic or cause local and central complications that can be fatal. We report the case of a 43-year-old male having a medical record of human immunodeficiency virus and hepatitis C who presented to our department with a 3-day history of a febrile lateral neck swelling. He reported a history of repetitive intravenous drug use and previous abscesses that were surgically drained. We noted a left and tender 8 cm neck swelling with torticollis. Computed tomography scan showed a collected myositis of the sternocleidomastoid muscle in association to multiple metallic foreign bodies at the neck that were compatible with the aspect of broken needles. Imagery also showed a thrombosis of the ipsilateral jugular vein. No central embolism of a foreign body was noted. We performed a surgical drainage of the muscular abscess and managed to retrieve a 1 cm broken needle that was retained at the level of the collection. We did not retrieve the other needles since they were asymptomatic. The patient was placed under intravenous antibiotics for 1 week followed by oral amoxicillin-clavulanate with a total regression of the cellulitis. At the further follow-ups, the rest of the foreign bodies remained asymptomatic. Our study emphasizes on the importance of suspecting a retained foreign body in intravenous drug users to ensure an adequate management of the possible complications and to protect the medical team from incidental needle injuries.
Introduction
Retained broken needles is one of the observed complications in intravenous drug users (IVDUs). The risk of its occurrence at the neck is increased by the repetitive use of needles in difficultly-accessible deep veins leading to their bending and breaking.1,2 These foreign bodies can remain asymptomatic. However, they occasionally lead to infectious and noninfectious complications such as deep neck infections (DNIs), internal jugular vein thrombosis as well as central embolism that can be fatal.3,4
We report a rare case of multiple retained foreign bodies at the neck that were incidentally discovered through a radiological exploration of a neck swelling caused by one of the retained needles. We aim to determine the clinical presentation of this entity, the possible complications, and their management modalities.
Case Report
A 43-year-old male, with a history of human immunodeficiency virus and hepatitis C treated with antiviral therapy, presented to our department with a 3-day history of a febrile neck swelling. He reported a well-documented history of intravenous buprenorphine and cocaine use over the past 2 years and prior episodes of peripheral abscesses that required a surgical drainage. On further questioning, the patient reported intravenous cocaine injection 2 days prior to the onset of the swelling. Neither dyspnea nor chest pain were reported.
Physical examination showed a firm and tender left lateral cervical swelling measuring 8 cm without an inflammatory aspect of the skin. The rest of the physical examination was normal.
Cervical computed tomography (CT) scan showed a cervical and facial cellulitis with a collected myositis of the left sternocleidomastoid muscle associated with a thrombosis of the ipsilateral jugular vein. CT scan also revealed the presence of 6 foreign bodies, dispersed bilaterally; their radiological aspect was similar to fragments of broken hypodermic needles (Figures 1 and 2). No radiological signs of a central migration of one of the foreign bodies were recorded.

Cervical contrast-enhanced computed tomography scan, frontal slide, showing a collection at the sternocleidomastoid muscle (red arrow) associated to multiple needle-shaped foreign bodies having a metallic density (red arrow heads).
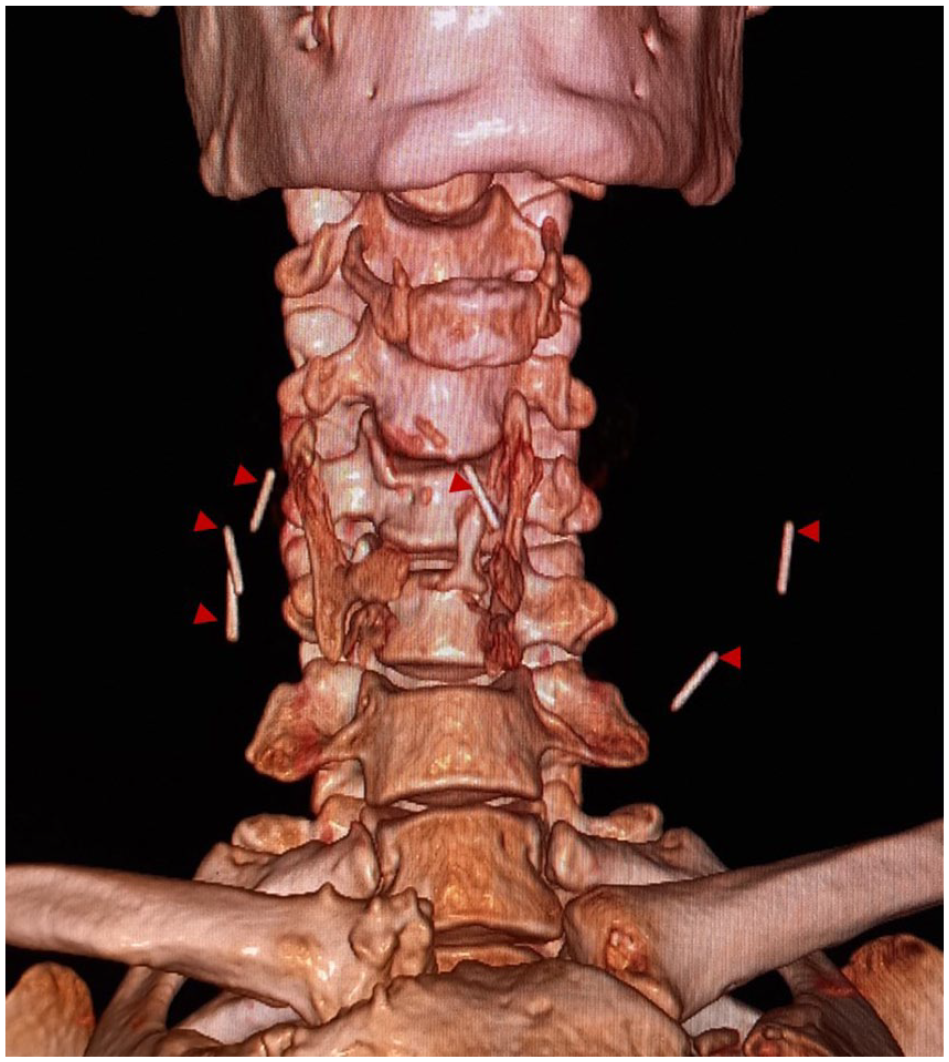
Cervical computed tomography scan with a 3D reconstruction showing the 6 retained needle-shaped foreign bodies (red arrow heads).
Due to the clinical presentation, we performed a surgical drainage of the abscess yielding 30 mL of pus. We also managed to retrieve a 1 cm insulin syringe needle that was retained at level of the collection.
Post-operatively, the patient received a 7-day course of intravenous antibiotics based on cefotaxime followed by oral amoxicillin-clavulanic with a total regression of the swelling and without recurrence. Further follow-up showed a favorable response without any signs invoking a delayed complication at the level of the other not-retrieved foreign bodies.
Discussion
Retained fragments of broken needles are one of the complications encountered by IVDUs.5,6 The possible causes include defective needles, hardened veins associated with chronic inflammation, sudden movement of the needle, or fainting during injection. The risk is also increased by the difficulty of self-injecting into the deep neck veins, by leaving needles without a catheter to ensure a prolonged access and by the reuse of needles leading to their bending and breaking.1,7
A retained needle with or without a further migration can remain asymptomatic and well tolerated for years with only a subtle clinical manifestation and a radiological discovery. It can also manifest by infectious and noninfectious complications.8,9 This entity should be suspected in IVDUs reporting a history of needle breaking or presenting fever and inflammatory signs at the injection sites. 1 Imaging is mandatory to confirm the presence of foreign bodies, detect associated complications, and protect the treating medical team from possible incidental needle sticks. 2 In our study, multiple neck foreign bodies were incidentally revealed by a local neck infection. A similar incidental discovery of multiple retained needles at the neck was seldom reported. 8
Infectious complications related to retained neck needles in IVDUs include DNIs; they are explained by the use of deep neck veins such as the jugular, the subclavian, or the brachiocephalic veins through the supraclavicular fossa due to the sclerosing and thrombosis of the peripheral veins.3,6 DNIs may evolve into neck abscesses mainly in the deep anterior triangle, posterior triangle, and superficial anterior triangle of the sternocleidomastoid muscle which are consistent with the injection sites. 3
Other reported complications include the thrombosis of the internal jugular vein. It needs to be suspected in IVDUs presenting a febrile neck inflammation. 10 It can be explained by the endothelial damage from the infected needles and the alteration of the blood flow. It is also majored by the lack of aseptic procedures.4,11,12 In our patient, one of the retained neck needles manifested by a cervical cellulitis with a thrombosis of the ipsilateral internal jugular vein.
Central needle embolism was occasionally reported in IVDUs. The timing of its occurrence is highly variable and was considered to be more decreased in patients performing neck injections. 7 It is caused by the escape of one of the fragmented needle pieces into the systematic vasculature through the venous system leading to fatal cardiac and pulmonary complications such as cardiac perforations, arrhythmias, tamponade, endocarditis, pericarditis, and pulmonary infections. These complications need to be suspected in IVDU presenting with fever, dyspnea, and chest pain.5,7,9,13
However, unrecognized needle foreign bodies are not only dangerous for the concerned patients but also for the clinicians due to the risk of an incidental needle stick mainly during the surgical drainage of abscesses.2,6
The management of retained needle in IVDUs remains not consensual due to the rarity of its occurrence and the scarce literature concerning the retrieval of broken needles. Undoubtedly, an early presentation after needle breakage is helpful to successfully extract it before its further migration. 14 Applying a tourniquet even by the patient himself at the moment of needle breakage can also decrease the risk of its further migration.14,15
Some studies consider an asymptomatic needle foreign body in IVDUs as a benign entity and then advocate a conservative management, especially that the occurrence of a delayed complication is very rare.1,8 It was also reported that IVDUs rarely present to emergency departments with problems related to retained broken needles. 7 In addition, the attempts to extract these needles can lead to their further intraluminal progression which exposes the patient to a further morbidity. Conducting a close observation of such foreign bodies is then possible.8,14 In our patient, we only retrieved the needle localized in the neck abscess while the rest of the foreign bodies were closely observed. Other authors rather advised to remove any retained needle, when possible, as early as possible, in order to avoid further complications related to its migration. 7
Conclusion
Although rarely reported, the retention of needles in the soft tissues of the neck is prevalent among IVDUs. It is crucial to emphasize on the importance of suspecting this entity to prevent not only the occurrence of cervical cellulitis and further fatal complications but also to ensure the safety of surgical teams by reducing the risk of blood exposure accidents.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series since we anonymously reported clinical and imaging information concerning our patient’s case.
Informed Consent
A written informed consent was obtained from the patient for his anonymized information to be published in this article.