
Abstract
Objectives:
To propose a management algorithm for adult patients with sharp-pointed esophageal foreign-body impaction (EFBI) who have rigid endoscopy (RE) indications and to conduct a retrospective analysis of their data.
Methods:
All adult patients who received RE at the Department of Otorhinolaryngology in Beijing Shijitan Hospital between January 2017 and May 2019 were enrolled. The demographics, clinical characteristics, and management data were collected and analyzed.
Results:
A total of 130 patients were identified, 56.9% were female with median age 60 years. More than half (56.9%) of patients had foreign-body (FB) ingestion on holidays. The most frequent FBs were jujube pits (66.9%) and bones (23.8%). There is a significant female predominance in ingestion of jujube pits (65.5%, P = .005). The most common symptoms were odynophagia (49.2%) and sore throat (47.7%). The majority (96.8%) of FB founded were lodged at upper esophagus. In all, 74 patients were categorized as having mild complications and 54 having significant complications. Time interval from ingestion to presentation longer than 15 hours was an independent risk factor for significant complications, while esophagogram with barium as a protective factor.
Conclusions:
Long-time interval from ingestion to presentation will lead to high risk of significant complications. Computed tomography should be a prioritized imaging method for all patients suspected with EFBI, and multidisciplinary collaboration is recommended. Besides, mass education on eating habits is necessary.
Keywords
Introduction
Esophageal foreign-body impaction (EFBI) is commonly encountered in the department of gastroenterology and the department of otorhinolaryngology, which generally occurs in children between the ages of 6 months and 6 years. 1,2 Approximately 80% to 90% ingested foreign bodies (FBs) pass through the gastrointestinal tract spontaneously without complications, while 10% to 20% require endoscopic treatment and less than 1% require surgery. 2 -5 With the advancement of endoscopic technique, more than 95% of EFBI in the upper gastrointestinal tract could be removed via flexible endoscopy (FE) successfully with only less than 5% complication rates. 2 -5 Rigid endoscopy (RE), which require general anesthesia, longer operation time, and higher procedural costs, is recommended only after FE failure or in challenging situations, especially sharp-pointed/proximal impactions and pediatric cases. 2,3,6,7 However, in clinical practice, the decision to perform RE or FE depends largely on the personal judgment of the on-call triage nurse in the emergency department—gastroenterologists prefer FE, while otorhinolaryngologists advocate RE. Most patients suspected of sharp-pointed FB ingestion were referred to the department of otorhinolaryngology to initially evaluate the upper aerodigestive tract above the cricopharyngeus. When EFBI were detected, subsequent RE removal may be performed by otorhinolaryngologists without multidisciplinary collaboration. This makes RE widely used unnecessarily. 8,9 Furthermore, ingested FB could be classified into certain types according to their features, including food bolus, blunt objects, sharp-pointed objects, long objects, and special objects (ie, magnets, coins, and disk batteries). 2,3,7,10 -12 Most previous researches have studied them together, although the clinical characteristics and management differ greatly from each other. 13
Herein, a tailored management algorithm was proposed, following which adult patients with sharp-pointed FB who require RE were distinguished. We retrospectively analyzed their clinical characteristics and comment on management of EFBI with RE from the perspective of otolaryngologists, trying to share our experiences with gastroenterologists and other otolaryngologists.
Patients and Methods
To properly diagnose and treat sharp-pointed FB ingested adult patients, as well as prevent unnecessary RE, a multidisciplinary management algorithm applicable for Chinese adult patients was established based on the latest consensus and guidelines (Figure 1). 13 This procedure was then strictly enforced since January 2017.
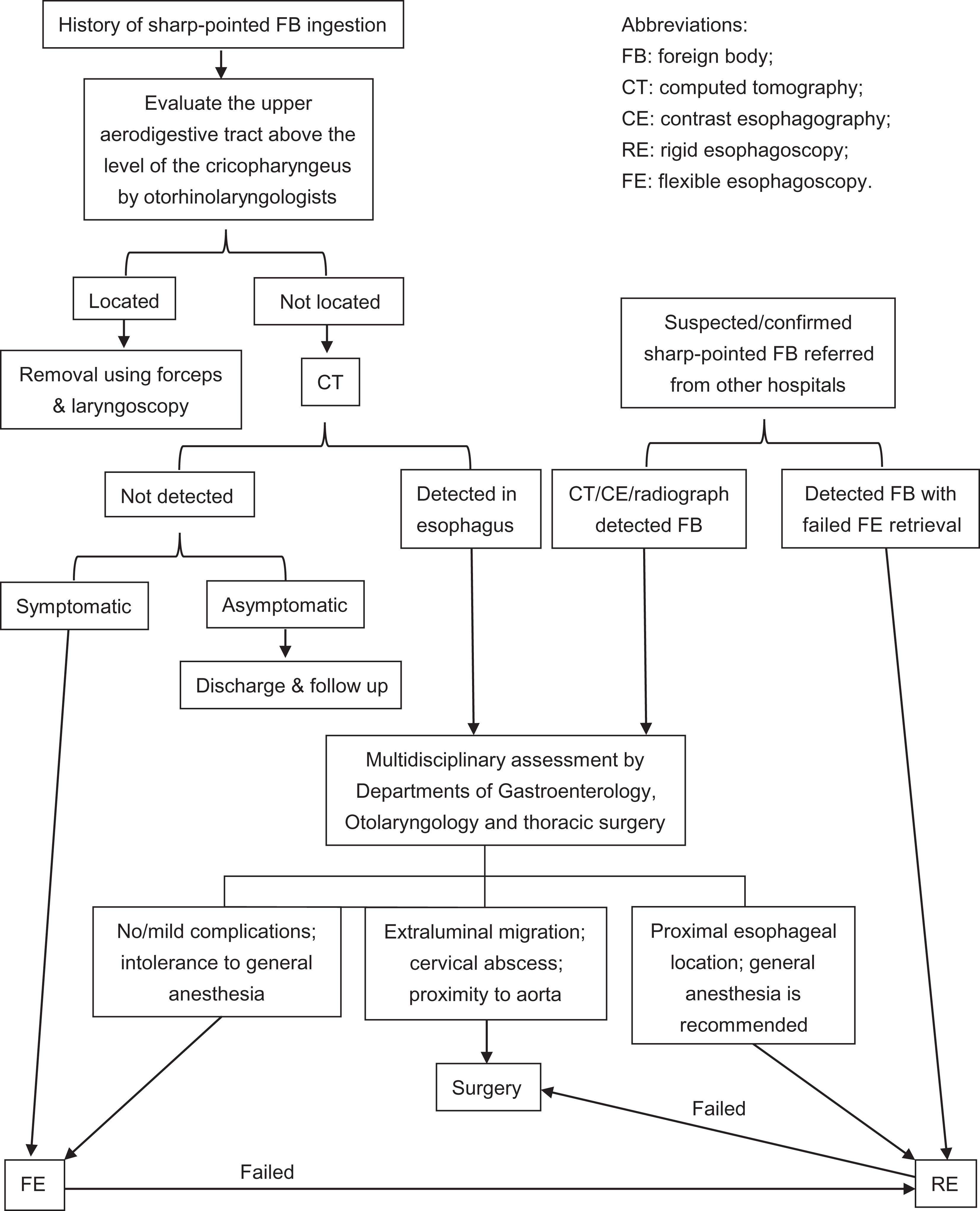
Management algorithm for sharp-pointed esophageal foreign-body ingestion in adults.
A retrospective study of all adult patients presenting with sharp-pointed EFBI to the Department of Otorhinolaryngology in Beijing Shijitan Hospital between January 2017 and May 2019 was conducted. Patients were identified by searching medical record database with the International Classification of Diseases, 10th Revision, Clinical Modification code T18.1, “foreign body in esophagus.” Patients satisfying the following criteria include the following: (1) FBs were sharp pointed, and (2) patients older than 18 years. Patients who didn’t undergo RE or transferred to other hospitals were excluded. The medical charts were meticulously reviewed about demographics, clinical characteristics, and management data. Data collected included age, gender, intention to ingestion, precise date of ingestion (classified into weekdays and holidays), time interval from initial ingestion to presentation, symptoms and complications at admission, comorbidities, procedures performed, physical examination, radiologic and endoscopic findings, type and location of FB, complications, and outcome.
The patients were divided into 2 groups according to the severity of complications resulting from the FB ingestion or endoscopic treatment. Minor mucosal injuries such as abrasions, minor hematomas/bleeding, and small erosions/edemas were defined as mild complications. While major mucosal injuries (ie, deep lacerations, abscesses, ulcers, perforations), pneumonia, mediastinitis, and mediastinal abscess/emphysema were defined as significant complications.
Descriptive statistics were used to summarize the findings. Quantitative data were presented as mean (standard deviation or median [interquartile range, IQR]), while qualitative data were presented as proportions. Means and medians were compared with independent samples t test or Mann-Whitney U test. Proportions were compared using Pearson χ2 test or Fisher exact test. Quantitative variables were transformed into qualitative variables using receiver operating characteristic (ROC) curves when necessary. Logistic regression was performed to identify independent predictive factors of significant complications. Variables with P < .20 in univariate analysis were entered in the logistic model (enter method). Adjusted odds ratios and 95% confidence intervals were reported. Two-tailed P values below .05 were considered statistically significant. All statistical analyses were performed using SPSS version 17.0 (SPSS Inc, Chicago, Illinois). The study protocol was approved by the institutional review board of the Beijing Shijitan Hospital.
Results
A total of 130 patients with sharp-pointed EFBI were identified from this research (Table 1). The median age was 60 years (IQR: 52-69 years), and 74 (56.9%) patients were female. More than half (74/130, 56.9%) of patients had FB ingestion on holidays, which is noticeably higher than the proportion of holidays in the whole year (115/365, 31.5%; P < .001). All patients ingested FB accidentally, except 1 prisoner who had intentional ingestion for secondary gain. Only 9 (6.9%) patients fast spontaneously after ingestion. The median time interval from initial ingestion to presentation was about 16 hours, ranging from 1 hour to 14 days.
Patient Characteristics (n = 130).
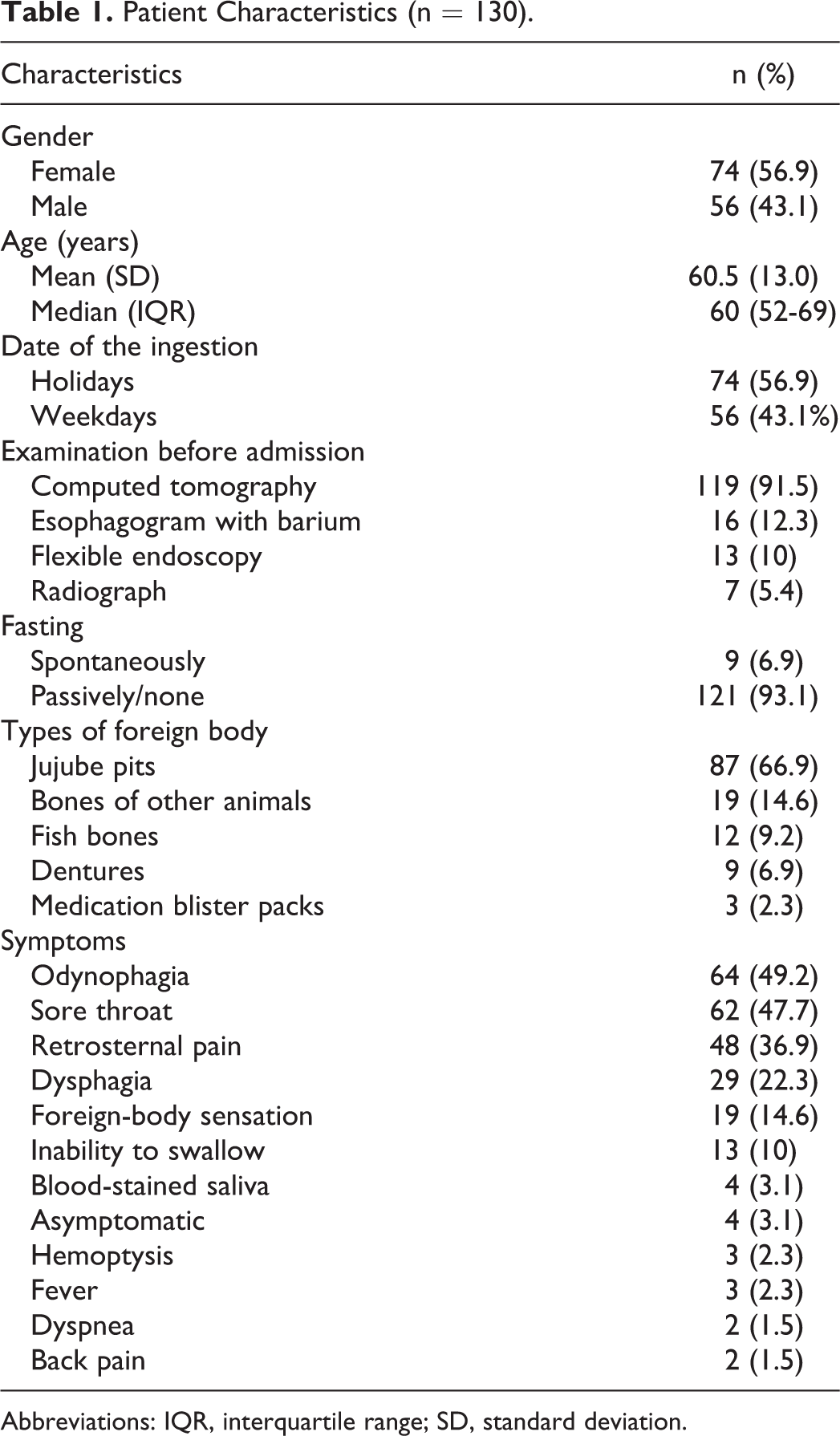
Abbreviations: IQR, interquartile range; SD, standard deviation.
The most frequent FB encountered were jujube pits (87, 66.9%), followed by bones (31, 23.8%), dentures (9, 6.9%), and medication blister packs (3, 2.3%). All of 9 ingested dentures were found embedded into the cricopharyngeal region with one edge. A significant female predominance in ingestion of jujube pits was observed (57/87, 65.5%; P = .005). Clinical symptoms at presentation varied greatly, the most common symptoms were odynophagia (64, 49.2%) and sore throat (62, 47.7%).
Sixty-three (48.4%) patients were referred from other hospitals. Among those patients, 16 patients underwent esophagogram with barium, 13 patients underwent failed FE removal, and 2 patients underwent failed laryngoscopy removal. Computed tomography (CT) was performed on all patients, except those with history of esophagogram with barium. All patients received RE. The FBs were located in 124 (95.4%) patients. The majority (120/124, 96.8%) of FB founded lodged at upper esophagus, including 80 around the cricopharyngeal sphincter. All visualized FB were successfully removed, including one patient with pneumonia, mediastinal abscess, and mediastinal emphysema who was referred to the intensive care unit after successful removal of FB with the assistance of cardiothoracic surgeons. Foreign bodies were not found in 6 (4.6%) patients and were excreted in stool afterward in 4 days. Of the 6 patients, 4 had received esophagogram with barium. Only 2 (1.5%) patients underwent biopsy during RE; pathologically confirmed granuloma and esophageal cancer, respectively. Endoscopy findings of esophageal and pharynx injury are listed in Table 2.
Endoscopic Findings (n = 130).
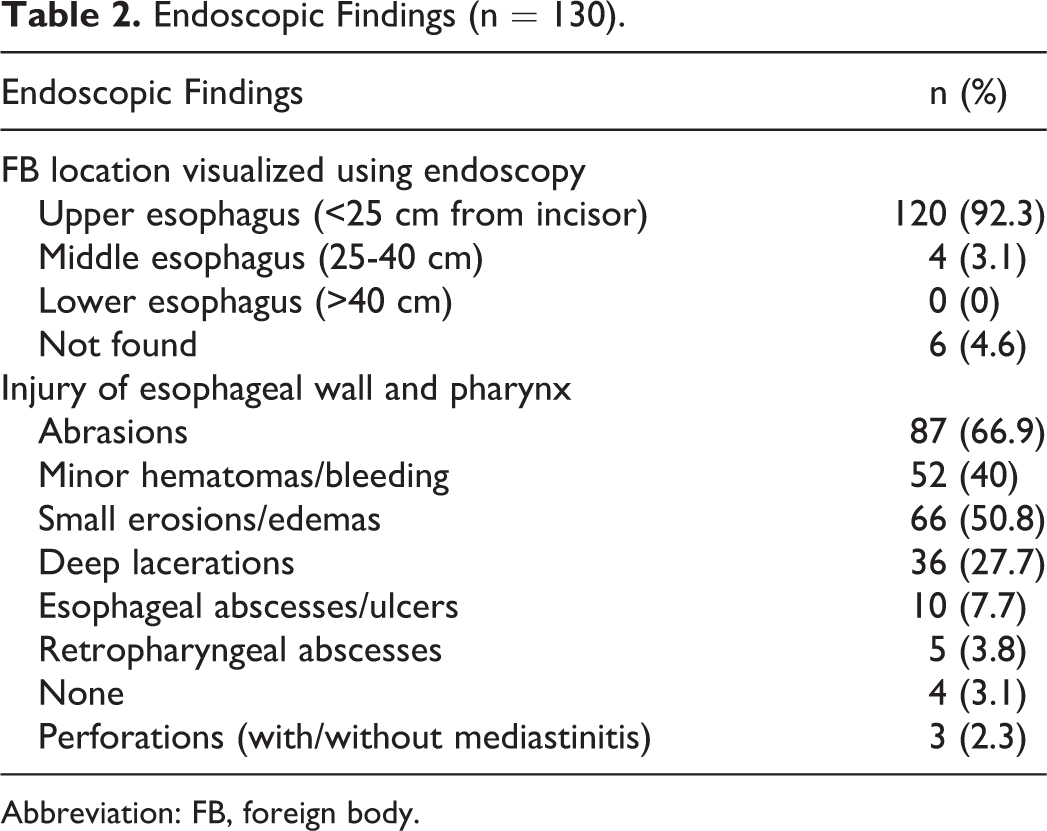
Abbreviation: FB, foreign body.
A total of 74 patients (58.5%) were categorized as having mild complications. The other 56 (41.5%) patients were categorized as having significant complications, including 2 asymptomatic patients. There were multiple differences between the 2 groups (Table 3). On univariate analysis, significant complications were associated with history of esophagogram with barium and time interval from initial ingestion to presentation. Whether fasting spontaneously after ingestion was not statistically associated with significant complications, although there was a lower proportion of significant complications in patients with spontaneously fasting than those without (22.2% vs 44.6%, P = .298). Because time interval from initial ingestion to presentation was a quantitative variable, it was transformed into 2 qualitative variables by ROC curves. A cutoff value of about 15 hours had the highest sensitivity (76.8%) and specificity (67.6%) for significant complications. On logistic regression, the only independent risk factor for significant complications was time interval longer than 15 hours, while esophagogram with barium was a protective factor (Table 4).
Comparison of Patients With Mild Complications and Significant Complications.
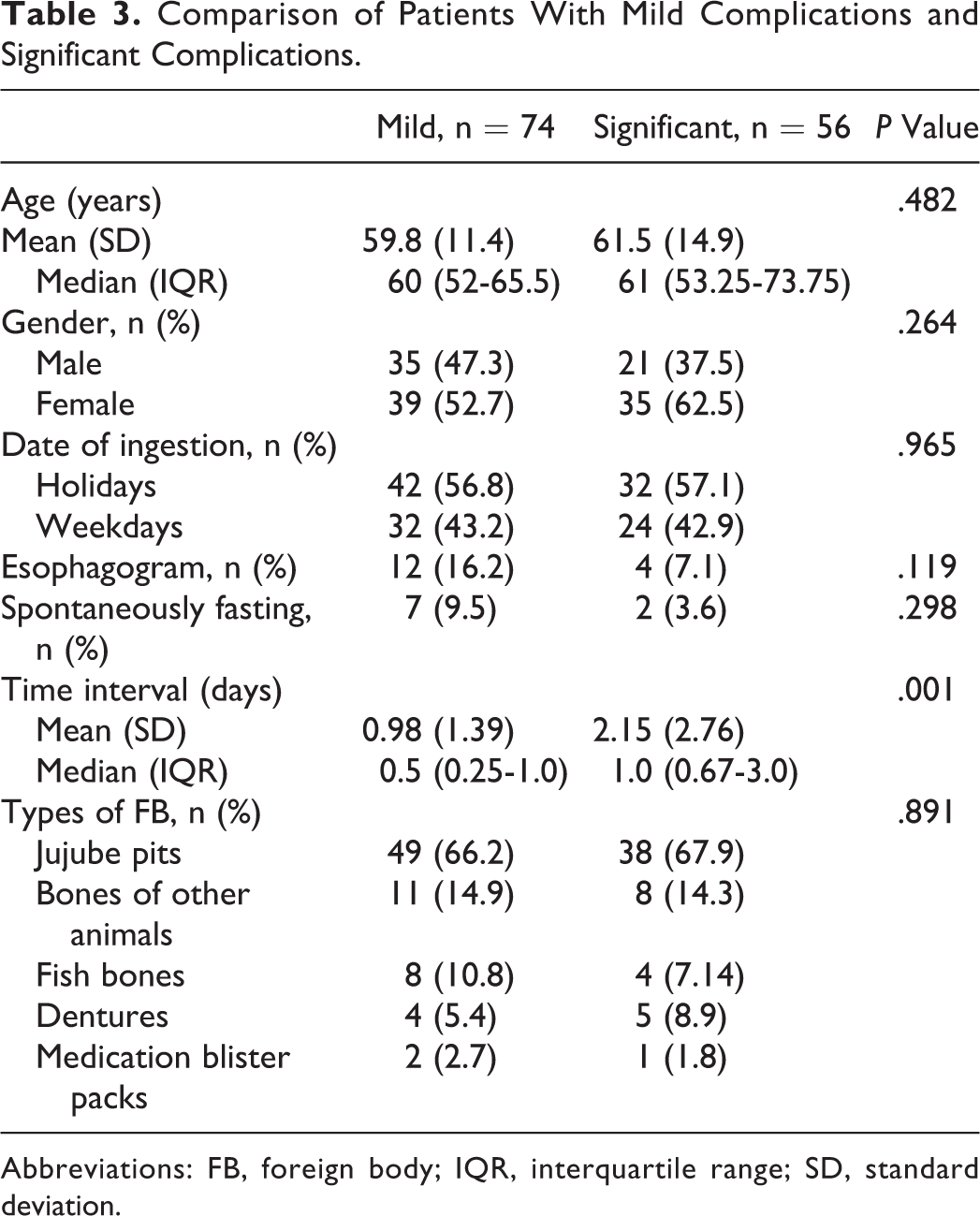
Abbreviations: FB, foreign body; IQR, interquartile range; SD, standard deviation.
Independent Predictors of Significant Complications.
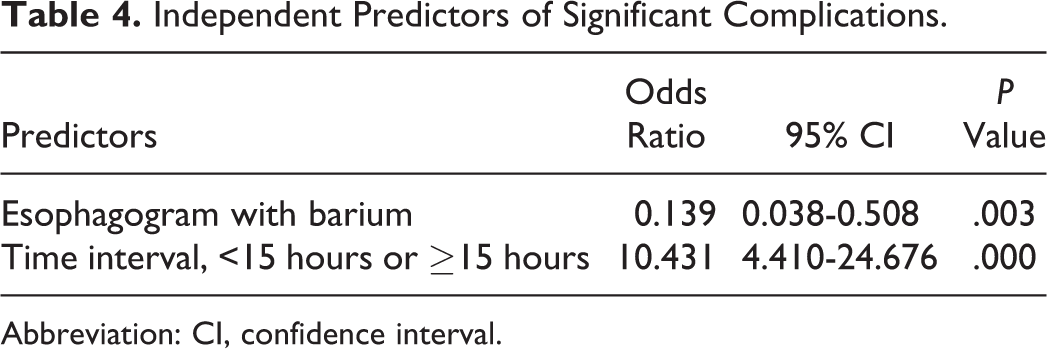
Abbreviation: CI, confidence interval.
Discussion
Sharp-pointed EFBI is a common emergency, which occurs more frequently in adults than in children. Its clinical characteristics and management differ greatly from food bolus impaction, which happens mainly in West countries. 14 However, most previous studies have confused them together. In addition, previous consensus and guidelines regarding management of EFBI have been conflicting. Endoscopy allows removal of FBs during examination, making it accepted by the majority of doctors and patients. 2,3,7,14,15 Both FE and RE could remove esophageal FB effectively, while each technique carries its own advantages and risks. European Society of Gastrointestinal Endoscopy (ESGE) and American Society for Gastrointestinal Endoscopy (ASGE) recommend FE as the first-line therapeutic option because it is cost-effective, well tolerated and less time-consuming and can be performed under sedation. Meanwhile, RE does have some advantages: (1) Muscle of esophagus could be completely relaxed under general anesthesia; (2) could reach proximal esophagus easily and provide excellent exposure, especially at the upper esophageal sphincter; and (3) provide a wider lumen and allow multiple instruments for the extraction of FB. (4) The airway is protected and (5) may be preferable for patients with inadequate cooperation such as children. 2,6,15 American Society for Gastrointestinal Endoscopy advocates RE as an alternative to FE for FB impacted at the level of the upper esophageal sphincter or hypopharyngeal region to protect the airway. 2 In contrast, RE is not even mentioned in the ESGE guidelines. 3 A most recent large system review reported that both FE and RE were performed in 65.1% and 16.8% of adult patients with EFBI, respectively, during the past 18 years. 7 It may be partially explained by the fact that FE was ignored by gastroenterologists and was vice versa abused by otolaryngologists.
In this study, a therapeutic procedure applicable for Chinese adult patients, especially in northern China, was established according to the latest consensus guidelines and doctor–patient relationship status in China (Figure 1). Following this procedure, adult patients with sharp-pointed OFEI who require RE necessarily were managed since 2017.
Previous studies demonstrate that patients >80 years are more likely to have FB ingestion. 7 In this cohort, age distribution was approximately normal distribution, with peak between 55 and 65 years. The fact that physiologically lacking of teeth and swallowing disorders occur with the increase in age may contribute to the high risk of FB ingestion in elderly patients. 7,15,16 And the custom of talking while eating may be the direct trigger. Moreover, age >50 to 60 years was identified as a risk factor for complications in several studies. 12,17 Unlike previous studies, no direct correlations were found between age and the incidence of significant complications in this cohort. A possible explanation is that most patients older than 70 to 80 years without self-care ability live with caregivers. Once they had FB ingestion, they were sent to hospital immediately, in contrast to the situation when they live alone.
Most FBs were ingested accidentally, while some were ingested intentionally such as psychiatric and incarcerated population. 18 -20 In this study, only 1 patient ingested FB intentionally—a prisoner with motive of probation. Similar to previous cases, the prisoner tided a thread on the FB wrapped in tape, and he told the prison guard immediately at ingestion. All of the above was trying to improve the successful rate of removal and to mitigate the risk of complications. Those patients should transfer to special care centers to prevent intentionally injury for a second time. However, the percentage of prisoners significantly decreased during the past years in our hospital. A suspected reason is that China had revised related laws to prevent such incidents.
Although some studies reported no correlation of impaction time with risk of complication, more researchers suggest that EFBI should be removed within 24 hours. 2,21,22 Gastrointestinal Endoscopy and ASGE strongly recommend emergent therapeutic endoscopy within 6 hours (preferably within 2 hours) for sharp-pointed EFBI because prolonged time undermines the possibility of removal and leads to higher risk. 2,3 But this is hard to execute in China, where both RE and FE procedures require fasting for at least 4 hours before endoscopy. In addition, the median time interval from initial ingestion to presentation was about 16 hours in this cohort, which is much longer than 6 hours. Moreover, only 6.9% of patients fast spontaneously after ingestion, and they have a lower proportion of significant complications compared with those without spontaneously fasting (22.2% vs 44.6%). These data must be interpreted in the context of Chinese patients. Due to the traditional mind-set in China, a large proportion of patients drink vinegar or swallow food forcibly instead of seeing doctors after FB ingestion. Besides, elders are unwilling to increase the burden on family members and worry about the cost, most of them hesitate whether to go to hospital, thus result in great delays in hospital visit. 16 This may increase the risk of complication and aggravate the mucosal injury. In line with the analysis, data in this cohort conclude that time interval longer than 15 hours is the only independent risk factor for significant complications in this study.
The culture that people are willing to gather together with/without drinking on holidays may explain the higher proportion of mis-swallow during holidays (56.9%) compared with workdays (43.1%) in this study. 15,23 Spicy and hot food always result in quick swallow, especially under the influence of alcohol, making people at high risk of FB ingestion.
Previous data indicate that types of impacted/ingested FB vary in different regions. Most studies in Asia and coastal countries reported that bone fragments, especially fish bones, are most commonly encountered. 3,12,13,16,18,24 While studies in the United States showed that meat comprised the majority type. 13,25 A systematic review including 13 092 patients all over the world revealed sharp-pointed FB (38.1%) as the most common FB. 7 The conflicting results may be owing to various social, cultural, economic, and religious factors in different regions. Take China, for example, the most common type of FB is fish bones in south China and coastal provinces, in contrast with jujube pits in north China. 9,26 This may be explained by the following reasons. First of all, north China is the main place of origin of jujubes, while fish are daily diet in south China and coastal provinces with an abundant supply. Secondly, Chinese eat rice dumplings during the Dragon Boat Festival. Northerners make rice dumplings with jujube, while southerners with meat. Moreover, northerners prefer congee cooked with jujube, and southerners prefer soup simmered with fish, meat, or bone. In present cohort, the most frequent FBs encountered were jujube pits (66.9%), followed by bones of other animals (14.6%) and fish bones (9.2%). In addition, ingestion of jujube pits occurs more commonly in female (65.5%). Female are relatively vulnerable mainly because the following reason: Traditional Chinese medicine advocates that jujube could adjust the vitality and nourish the blood, extremely suitable for female. As to fish bones, the incidence among Chinese patients was a lot higher as compared with other Asian patients. 27 This may be associated with following reasons: deboning fish in mouth, eating fish with chopsticks, and wearing dentures while eating fish. 27,28 To avoid such incidence and accidental denture ingestion, dental implants is advised instead of removable dentures for the seniors, especially for patients with seizure and Alzheimer. 7
In this study, about half of patients had odynophagia and sore throat. And only 4 (3.1%) patients were asymptomatic, significantly less than previous studies. 14,24,29 This may due to the mix of food bolus impaction with FB ingestion in previous studies. Foreign-body ingested patients were more frequently symptomatic, while a considerable number of patients with food bolus impaction were asymptomatic. 2,3,14 However, the symptom does not correlate with the severity of complication. In the present cohort, there are 4 asymptomatic patients. Of these 4 patients, 2 had mild complications and 2 had significant complications.
In clinical practice, radiopacity and radiographic visibility are usually confused. 30 In fact, they are 2 different concepts. Radiographic visibility depends on the radiopacity, size, and location of the impacted patients. Most radiopaque, even some radiolucent-ingested sharp-pointed FB, could not be identified on radiographs, but on CT. 2,3,31 Moreover, CT could evaluate relevant regional complications, and the sensitivity and specificity of CT may be increased with the 3-dimensional reconstruction. 2,32 The ESGE guideline does not recommend radiological evaluation for nonbony food impaction without complications, and CT is recommended in patients suspected of perforation or other complications requiring surgery. However, CT should be a prioritized imaging method for all patients suspected with EFBI, even in asymptomatic patients.
Physiologically, there are 4 anatomical stenoses in the esophagus at the level of the cricopharyngeal sphincter, the aortic arch, the crossing of left main bronchus, and the diaphragmatic hiatus. And about two-thirds or more EFBI lodge at the upper esophagus, especially at the level of the cricopharyngeal sphincter, which is the most narrowing area. 7,33,34 In this cohort, 96.8% of FBs lodged at upper esophagus, among which two-thirds located around the cricopharyngeal sphincter. The higher proportion is mainly because of the multidisciplinary collaboration following the procedure in Figure 1. The majority of FB located at the middle/lower esophagus and those parallel to the esophagus were removed by FE after multidisciplinary assessment in this study. Another possible reason is that jujube pits is the most common FB in this cohort. The size and fusiform shape with 2 pointed ends makes jujube pits mainly embedded at the upper esophagus (Figure 2). Pathological stricture may exist, associated with underlying esophageal disease. 7,33,34 The most frequently associated etiology of EFBI in adults is eosinophilic esophagitis (EoE) as proved by biopsy, accounting for 12% to 53% of patients. 11,23,35,36 Moreover, clinical characteristics differ between EFBI patients with and without EoE. 11 While in this cohort, esophageal biopsies were performed in only 2 patients, who had noticeable masses. None of them confirmed EoE. The lower proportion for biopsy was partially due to the fact that underlying etiology in the patients with sharp-pointed FB was significantly less prevalent than those with food impaction. 14 A more important reason is that otolaryngologists rarely perform mucosal biopsies when remove FB.
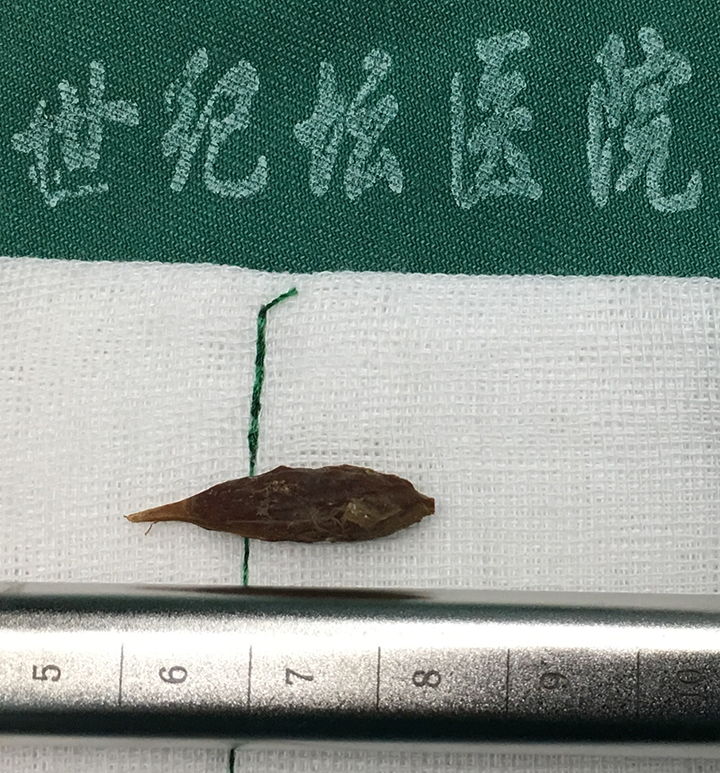
A fusiform shaped jujube pit removed from esophagus with a length of more than 2 cm.
Various medications such as glucagon and proteolytic enzymes have been advocated for esophageal food bolus impaction, while the effectiveness and safety are debated. 3,23,37 Moreover, there’s no evidence to support the effectiveness of medical management in sharp-pointed EFBI. Therefore, as designed in this procedure, medications are not recommended for sharp-pointed EFBI.
Previous studies reported that as high as 35% sharp-pointed FB lead to perforation. 2,3 Thus, once the FB, especially those wider than 2.5 cm, passed the esophagus, daily radiographs should be performed to document passage. 2,31,32 However, daily radiographs are not feasible in this study due to the doctor–patient relationship status in China. In this cohort, FBs were not found in 6 patients during endoscopy and were excreted in stool afterward in 4 days. Of the 6 patients, 4 had history of esophagogram with barium in primary medical units. Furthermore, logistic regression revealed that esophagogram with barium is a protective factor for sharp-pointed EFBI in this study. However, contrast esophagography was largely opposed because of aspiration risk and interference with subsequent endoscopic and radiographic visualization. 2,3 Considering the fact barium aspiration can be life-threatening but rarely occurred, esophagogram with barium is cautiously suggested as an effective and cost-effective option for patients without perforation when FE/RE are unavailable.
As a retrospective and single-center research, this study does have several inevitable limitations: (1) This cohort is subject to selection biases, (2) the sample was not large enough and the clinical data were reviewed retrospectively, (3) as most FBs were irregularly shaped, their precise sizes could not be measured radiographically, and (4) considering that most mucosal injuries were found after removal of FB and there was an incubation period between infection and manifestation; therefore it is difficult to distinguish whether complications were from the FB itself or iatrogenic. In view of the limitations above, prospective studies evaluating this procedure are needed in the future.
In conclusion, this study highlights multidisciplinary collaboration. People should visit doctor immediately after FB ingestion without hesitation. Computed tomography should be a prioritized imaging method for all patients suspected with EFBI. In addition, otorhinolaryngologists should recognize the importance of esophageal biopsy. And mass education on eating habits is necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.