
Abstract
Introduction
Thyroid cancer is one of the most common malignant tumors of the endocrine system, ranking 9th in the global cancer spectrum. It ranks seventh in the total population of China and third among women, with an increasing incidence around the world.1,2 The prevalence of coronary heart disease also increases year by year. Approximately 1 million patients undergo coronary stent implantation surgery in the United States and Europe each year, and there are more than 11 million patients with coronary heart disease in China.3,4 In clinical practice, we see more and more patients with coronary heart disease who need thyroid surgery, most of whom take antiplatelet drugs such as aspirin and clopidogrel. At this time, both patients and doctors must decide whether to stop antiplatelet therapy before surgery and risk potentially life-threatening thromboembolic events or continue treatment and risk intraoperative bleeding and related complications. 5 Currently, there is no general consensus in domestic and foreign guidelines on this issue, and there is a lack of literature on the impact of stopping or continuing antiplatelet therapy on thyroid surgery. This study investigates the safety of continuing aspirin use in patients with coronary heart disease undergoing thyroid surgery during the perioperative period to provide a reference for the perioperative management of such patients.
Materials and Methods
Subjects and Methods
Subjects
All eligible coronary heart disease patients who underwent thyroid surgery at Beijing Anzhen Hospital affiliated to Capital Medical University from July 2019 to June 2023 were selected as the observation group, with a total of 44 cases. Forty-four patients who underwent the same surgery at the same hospital during the same period without coronary heart disease and without anticoagulant or antiplatelet therapy were selected as control group 1. Another 44 patients with coronary heart disease who underwent the same surgery in the same hospital from August 2015 to June 2019 and used a low molecular weight heparin bridge during the perioperative period were selected as control group 2. The clinical data of the patients was collected for retrospective analysis. The selection criteria for the control group were patients who underwent the same surgical procedure as the observation group and had the closest surgical date. Inclusion criteria for surgery: (1) highly suspected thyroid cancer or benign thyroid nodules with a diameter > 4 cm diagnosed by preoperative ultrasound; (2) voluntarily signed informed consent for surgical risk; (3) observation group all had a history of coronary heart disease and received aspirin-drug antiplatelet therapy. Exclusion criteria for surgery: (1) patients with poor general condition who could not tolerate surgery; (2) patients who were reluctant about surgery and could accept tumor-bearing survival; (3) patients with other diseases that required simultaneous anticoagulation or dual antiplatelet therapy; (4) patients who had a recent myocardial infarction or underwent cardiac stent placement within 6 months. Coronary heart disease patients had New York Heart Association functional classification I to II. This study was approved by the Ethics Committee of Beijing Anzhen Hospital, affiliated to Capital Medical University (2019081X). The authors assert that all procedures contributing to this work comply with the Declaration of Helsinki of 1975, as revised in 2008.
Treatment methods
Perioperative preparation
All 3 groups of patients underwent preoperative thyroid ultrasound examination, blood tests including thyroid function, parathyroid hormone, routine blood tests, coagulation function, routine biochemistry, electrocardiogram, chest radiograph, lung function, and so on. The cardiac function of the observation group was also evaluated by measuring cardiac biomarkers, brain natriuretic peptide (BNP), echocardiography, coronary computed tomography angiography (CTA), and so on, and myocardial perfusion imaging was performed in patients with coronary artery stenosis >70% to confirm the presence or absence of myocardial ischemia. The observation group continued to use 100 mg Qd aspirin (Bayaspirin, 0.1 g, Bayer HealthCare Manufacturing S.r.l., Milan, Italy) during the perioperative period; control group 1 did not use anticoagulant or antiplatelet therapy before surgery; control group 2, which was the previous research data of the project group, stopped using aspirin 5 to 7 days before surgery and administered low molecular weight heparin (Aspen, 5070) 1 mg/kg, 12 hour/once subcutaneously. Low molecular weight heparin was discontinued the night before surgery until 72 hours after surgery, and low molecular weight heparin was resumed at the preoperative dose and frequency 3 to 5 days after surgery, switching back to aspirin on postoperative Day 5. 6 All patients were prohibited from using hemostatic drugs during the perioperative period.
Surgical methods
According to the condition, the observation group underwent unilateral subtotal thyroidectomy (benign nodules with tumor diameter >4 cm) in 9 cases, unilateral lobectomy + isthmus resection + ipsilateral central lymph node dissection (malignant, unilateral lesion) and unilateral lobectomy + isthmus + contralateral partial lobectomy + ipsilateral central lymph node dissection (malignant, contralateral single nodule benign lesion) in 22 cases, total thyroidectomy + bilateral central lymph node dissection (malignant, multiple nodules, or capsular invasion) in 11 cases, and total thyroidectomy + lateral neck and central lymph node dissection (malignant, lateral neck lymph node metastasis) in 2 cases. As the control groups were matched according to the same surgical procedure, the surgical methods for the 3 groups were exactly the same. Intraoperative bipolar electrocoagulation was used for meticulous dissection, complete hemostasis, and protection of the recurrent laryngeal nerve, superior laryngeal nerve, and parathyroid glands. At the end of the surgery, a drainage tube was placed, and the layers were sutured and pressure bandaged. The drainage tube was removed when the 24 hour drainage volume was less than 10 mL. All operations were performed by the same team of doctors.
Observation indicators
Age, sex, surgical time, intraoperative blood loss, total postoperative drainage volume, duration of drainage tube retention, total hospital stay, postoperative hospital stay, preoperative, and postoperative Day 1 hemoglobin (Hb), platelet (PLT), international normalized ratio (INR), and incidence of cardiovascular events were compared between the 3 groups.
Statistical methods
SPSS 25.0 software was used for statistical analysis of the data. Measurement data was tested for normality using the Kolmogorov–Smirnov test. Normally distributed data was expressed as mean ± standard deviation (±s), and one-way analysis of variance was used for comparisons between multiple groups. The least significant difference (LSD) test was used for pairwise comparisons with equal variances, and the Tanhane test was used for unequal variances. The independent sample t-test was used for comparisons between groups, and the paired sample t-test was used for comparisons within the group. Nonnormally distributed data were expressed as median and interquartile range M(P25, P75), and the Kruskal–Wallis H test was used for multiple group comparisons. The entire pairwise method was used for pairwise comparisons, the Mann–Whitney U test was used for comparisons between groups, and the Wilcoxon Z test was used for comparisons within groups. The count data were expressed as percentages (%), and the chi-square test was used for comparisons between groups, with the Bonferroni method for post hoc analysis. All statistical tests were 2-sided, with P < .05 considered statistically significant.
Results
Basic patient information: the age and the proportion of male patients in patients with coronary heart disease (observation group, control group 2) were higher than in control group 1, with statistically significant differences (P < .05, Table 1).
Comparison of Basic Data of the 3 Groups of Patients [Cases (%)], (
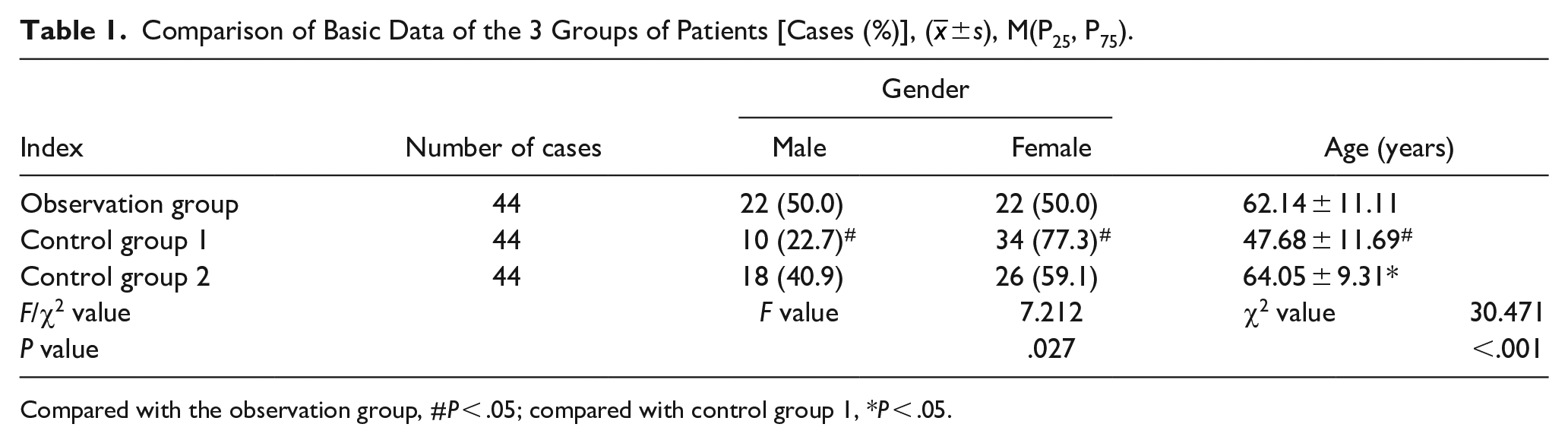
Compared with the observation group, #P < .05; compared with control group 1, *P < .05.
All patients successfully completed the surgery, recovered, and were discharged without perioperative death, acute myocardial infarction, stroke, pulmonary embolism, or other serious complications. There were also no permanent recurrent laryngeal nerve injury, parathyroid function decline, postoperative hematoma, or major bleeding related to thyroid surgery. One patient in the observation group and 2 patients in control group 2 experienced chest pain after returning to the ward on the day of surgery. Pain disappeared after infusion with isosorbide dinitrate, and monitoring of electrocardiogram and cardiac enzymes showed no significant changes.
There were no statistically significant differences in surgical time, intraoperative blood loss, postoperative drainage volume, duration of drainage tube retention, postoperative hospital stay, and perioperative Hb, PLT, INR, and so on among the 3 groups of patients (all P > .05, Tables 2 and 3). However, the total hospital stay was significantly longer in control group 2 than in the observation group and control group 1 (P < .01, Table 2).
Comparison of Hospital Data of the Three Groups of Patients M(P25,P75).
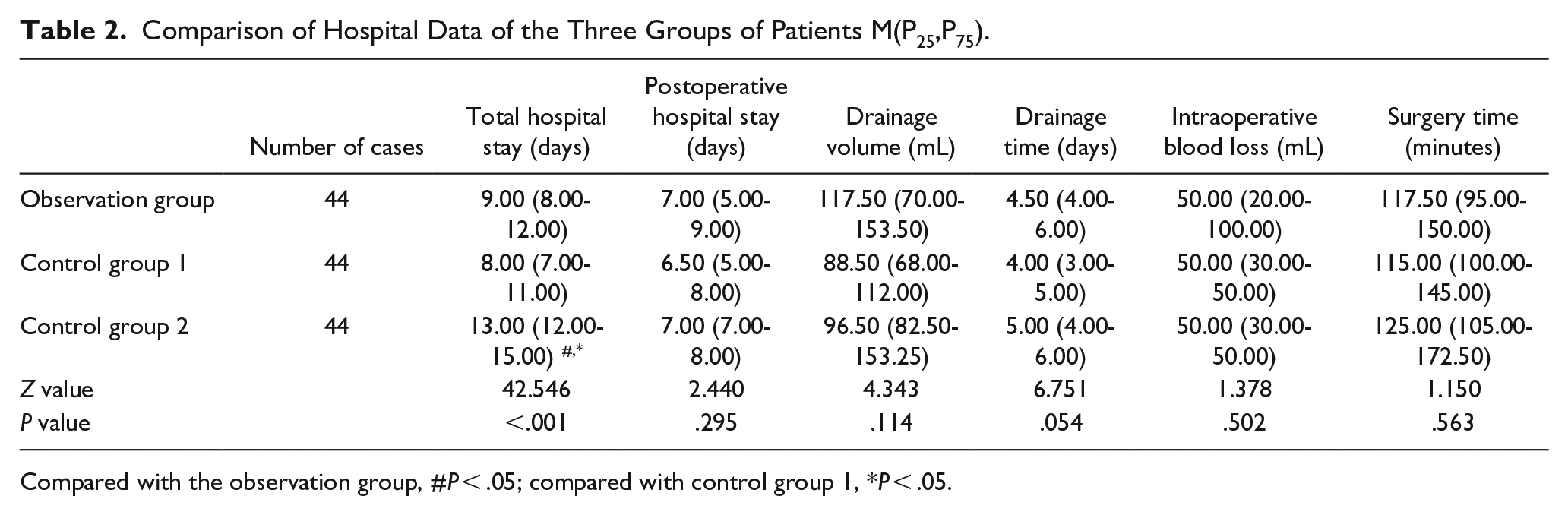
Compared with the observation group, #P < .05; compared with control group 1, *P < .05.
Comparison of Preoperative and Postoperative HB (g/L), PLT (109/L), INR in the three groups of patients M(P25, P75).
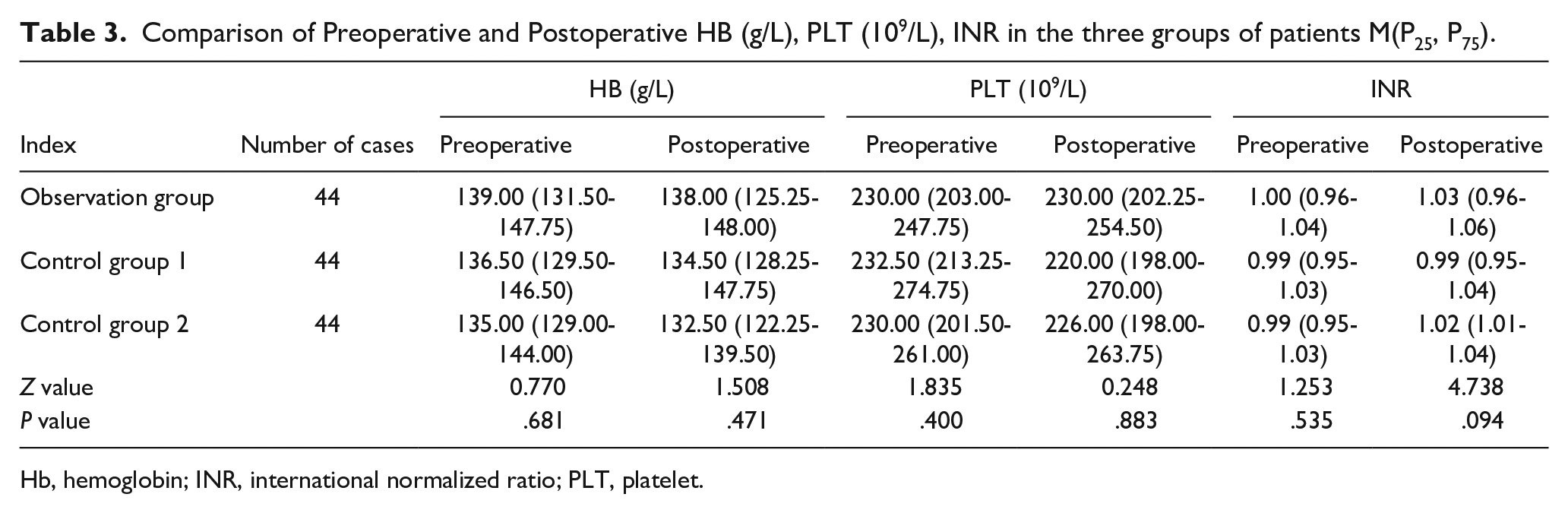
Hb, hemoglobin; INR, international normalized ratio; PLT, platelet.
Discussion
Perioperative bleeding is one of the most important concerns in thyroid surgery. Intraoperative bleeding can increase the difficulty of identifying and protecting recurrent laryngeal nerves, superior laryngeal nerves, and parathyroid glands, increasing the risk of injury and causing postoperative complications such as hoarseness and parathyroid dysfunction. Postoperative bleeding can lead to life-threatening airway compression due to hematoma formation. Therefore, head and neck surgeons are very sensitive to factors that may cause bleeding.
Antiplatelet therapy plays an important role in the primary and secondary prevention of cardiovascular and cerebrovascular diseases. 7 In recent years, the use of antiplatelet drugs has increased significantly, and aspirin is the most widely used antiplatelet drug. 8 The number of patients who undergo surgery who have been taking aspirin for a long time is also increasing. Each year in the United States and Europe, approximately 1 million patients undergo coronary stent implantation, and up to 15 and 25% of patients, respectively, undergo some invasive diagnostic or surgical procedure within 1 and 5 years after stent implantation. 3 At this time, both patients and doctors face the choice of stopping treatment before surgery, risking life-threatening thromboembolic events, or continuing treatment, risking intraoperative bleeding and related complications. A survey showed that most otolaryngologists routinely advise patients to stop taking aspirin before surgery. Ninety-one percent of the respondents reported that they asked patients to discontinue antiplatelet therapy before elective surgery, and 65% of the respondents reported that they would consider heparin bridging therapy. The main reason for this is the concern that aspirin can increase the risk of perioperative bleeding. 9 Their concerns are supported by some literature; for example, a review of 50 studies on cardiopulmonary bypass cardiac surgery showed an average increase of 300 mL of bleeding per patient. 10 During transurethral prostatectomy, patients taking aspirin had a 2.7-fold increase in transfusion rate compared to the control group, with 23 deaths. 11 In the first 24 hours after tonsillectomy, there was no difference in bleeding between patients using aspirin and acetaminophen. However, the incidence of secondary bleeding with aspirin increased about 6 times. 12
However, the risk of thromboembolic events caused by discontinuation of medication may need more consideration. Studies have shown that discontinuing aspirin 7 to 10 days before surgery may be dangerous for certain populations of patients, with a 3-fold increase in the risk of cardiovascular events, and the average time from discontinuation of the medication to the onset of acute coronary syndrome is 8 to 11 days. 13 Sudden discontinuation of antiplatelet drugs can produce a rebound effect, significantly increasing the incidence of acute coronary syndrome, death, and myocardial infarction. 14 The latest guidelines from the European Society of Cardiology and the European Society of Anaesthesiology for noncardiac surgery recommend that antiplatelet therapy is generally continued during the perioperative period, at least maintaining single-drug aspirin therapy, for patients at risk of thromboembolic events. However, the guidelines also indicate that individual decisions should be made after weighing the risks of bleeding and thrombosis. 15 Increasing research supports the continuation of aspirin use during the perioperative period. Francis David O et al. 16 suggest that maintaining antiplatelet therapy during minimally invasive laryngeal surgery does not increase the risk of bleeding. Researchers have also reached the same conclusion in vitrectomy, laparoscopic colorectal cancer surgery, endoscopic airway surgery for laryngotracheal stenosis, and lung resection.17,18,19,20 There is still a lack of general consensus on how to manage antiplatelet therapy during the perioperative period of noncardiac surgery, and the situation is constantly changing. We previously used preoperative discontinuation of aspirin with a low molecular weight heparin bridging regimen, and research results suggested that the use of low molecular weight heparin bridging did not increase perioperative bleeding, and the surgery was relatively safe. However, most patients were unable to complete the switch from aspirin to the low molecular weight heparin bridge on their own prior to surgery, requiring early hospitalization, which significantly extended the patient’s hospital stay, reduced medical efficiency, increased patient costs, and increased the patient’s psychological burden. 6 Furthermore, with the update of the guidelines and the publication of new literature, more and more views support the continuation of aspirin use during the perioperative period. In particular, the multidisciplinary consensus on perioperative antithrombotic therapy for patients with coronary stent classifies thyroid surgery as a moderate risk of bleeding and recommends continuing aspirin during the perioperative period. 21 We hypothesize that if the postoperative hematoma compresses the airway, the life-threatening risk can be mitigated if the hematoma is detected in time and the wound is reopened. On this basis, we have conducted special training for ward physicians and nurses (when the patient has symptoms of neck swelling or breathlessness, the neck dressing should be removed immediately for examination. If swelling and subcutaneous bruising in the operative area or blood clot in the drainage tube are found, the wound should be opened in time for exploration and hemostasis), discontinued the study of low molecular weight heparin bridging, and began to use aspirin during the perioperative period. This is also the reason why this study is not a randomized double-blind design, but rather uses bridge patients from previous research as the control group. The results of this study indicate that continuing aspirin use during the perioperative period is safe for patients undergoing thyroid surgery, does not increase the risk of intraoperative and postoperative bleeding, and does not increase the complications of thyroid surgery itself, which is consistent with the findings of Raggio et al. 22 Furthermore, the hospital stay of the observation group was significantly shorter than that of the low molecular weight heparin bridge group, with a statistically significant difference (<0.01). The absence of aspirin discontinuation during the perioperative period can also effectively avoid the rebound effect of abrupt discontinuation of antiplatelet drugs, although this has not been confirmed due to the small number of cases.
The age and sex differences between patients with coronary heart disease (observation group and control group 2) and noncoronary heart disease patients are worth discussing. In our study, we found that the male-to-female ratio in the coronary heart disease group was close to 1:1, while the ratio in control group 1 was close to 1:3, with a significant statistical difference. This is because the incidence of coronary heart disease is higher in men than in women, while the male-to-female ratio in the noncoronary heart disease group is closer to the incidence of thyroid disease. 2 Furthermore, the average age of the coronary heart disease group was higher than that of the noncoronary heart disease group, with a statistical difference, which is due to the increasing incidence of coronary heart disease with age; this is consistent with the literature reporting that patients receiving antiplatelet therapy may be older compared to those not receiving antiplatelet therapy. 18
Conclusions
In our study, thyroid patients on long-term oral aspirin antiplatelet therapy, continuing aspirin use during the perioperative period does not increase the incidence of perioperative bleeding, hematoma, and cardiovascular and cerebrovascular events, and surgery is relatively safe.
Methodological Considerations/Limitations
This study is a retrospective analysis with a small sample size, and the 3 groups of patients were not randomly assigned to undergo surgery at the same time, which are the limitations of this study. However, with the update of thyroid guidelines and the publication of new literature, more and more views support the continuation of aspirin use during the perioperative period. Given the study design and number of patients available for study, patients could only be matched on several key variables, and potential selection bias is difficult to avoid with this trial design. Future studies should consider a randomized, double-blind design to help avoid these limitations.
Supplemental Material
sj-xls-1-ear-10.1177_01455613241230844 – Supplemental material for Safety of Continuing Aspirin Use in Patients With Coronary Heart Disease Who Undergo Thyroid Surgery During the Perioperative Period
Supplemental material, sj-xls-1-ear-10.1177_01455613241230844 for Safety of Continuing Aspirin Use in Patients With Coronary Heart Disease Who Undergo Thyroid Surgery During the Perioperative Period by Yuansheng Rao, Jianhong Wang, Fan Yang and Xin Ni in Ear, Nose & Throat Journal
Footnotes
Data Availability Statement
The data that support the findings of this study are available in the supplementary material of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.