
Abstract
Hyoid bone fracture unrelated to strangulation is a rare occurrence characterized by a subtle presentation. However, it may manifest as a fatal respiratory distress due to airway obstruction. We present 2 cases of hyoid bone fractures that occurred following a traffic accident in 2 male patients. Both patients presented with either a neck pain or a dysphagia. Physical examination findings were limited to neck sensibility at palpation, saliva stasis, and laryngeal congestion at the laryngeal endoscopy. In both patients, the diagnosis was confirmed through computed tomography. In the first patient, the fracture was simple and located at the body of the hyoid bone, while in the second patient, it involved the greater horn with a medial displacement of the fractured fragment. Due to the clinical presentation, we successfully treated both our patients conservatively through a 48 hour observation, analgesics, steroids, antibiotics, neck rest, and semiliquid diet. This study highlights a rare occurrence of 2 cases of hyoid bone fracture unrelated to strangulation, which emphasizes on the importance of a high clinical suspicion to make the diagnosis of this entity.
Introduction
Hyoid bone fractures are a very rare entity that accounts for 0.002% of all fractures. 1 They are predominantly secondary to strangulation. However, isolated occurrences of hyoid bone fractures following other circumstances were seldom reported. 2 The clinical presentation of hyoid bone fractures varies from a subtle neck pain to an acute life-threatening respiratory distress. Other possible clinical manifestations include odynophagia, dysphonia, and neck swelling.1,3 The diagnosis of hyoid bone fractures is difficult due to their subtle and unspecific presentation. It is based on computed tomography (CT) scan.2,4 Given the rarity of this entity, there is no specific consensus regarding its management modalities. Treatment is mainly conservative and depends on the clinical presentation and associated complications.5,6
In this study, we report 2 cases of an isolated hyoid bone fracture resulting from a traffic accident. Our aim is to determine the clinical presentation of hyoid bone fractures, the possible complications of this rare entity, and its management modalities.
Case Report
First Case
A 42-year-old patient having a medical history of diabetes was a victim of an anterior cervical trauma due to a traffic accident. He was referred to our department due to a dysphagia to solids without any associated dysphonia, odynophagia, or signs of airway compromise. Neck examination was normal without any sensibility or subcutaneous emphysema. Laryngeal endoscopy showed a saliva stasis associated to a laryngeal edema and congestion without any hematoma or laceration. Due to the trauma mechanism and endoscopic findings, we suspected a laryngeal injury. A cervical CT scan was performed revealing a simple hyoid bone fracture without any associated laryngeal, mandibular, or facial fractures (Figure 1). It also showed an acromioclavicular luxation. We opted for a conservative management through a 48 hour close observation, steroids, analgesics, antibiotics, and a semiliquid diet. Symptoms totally resolved after 3 days. Control laryngeal endoscopy was normal. We did not record any complaints after a follow-up period of 2 weeks.
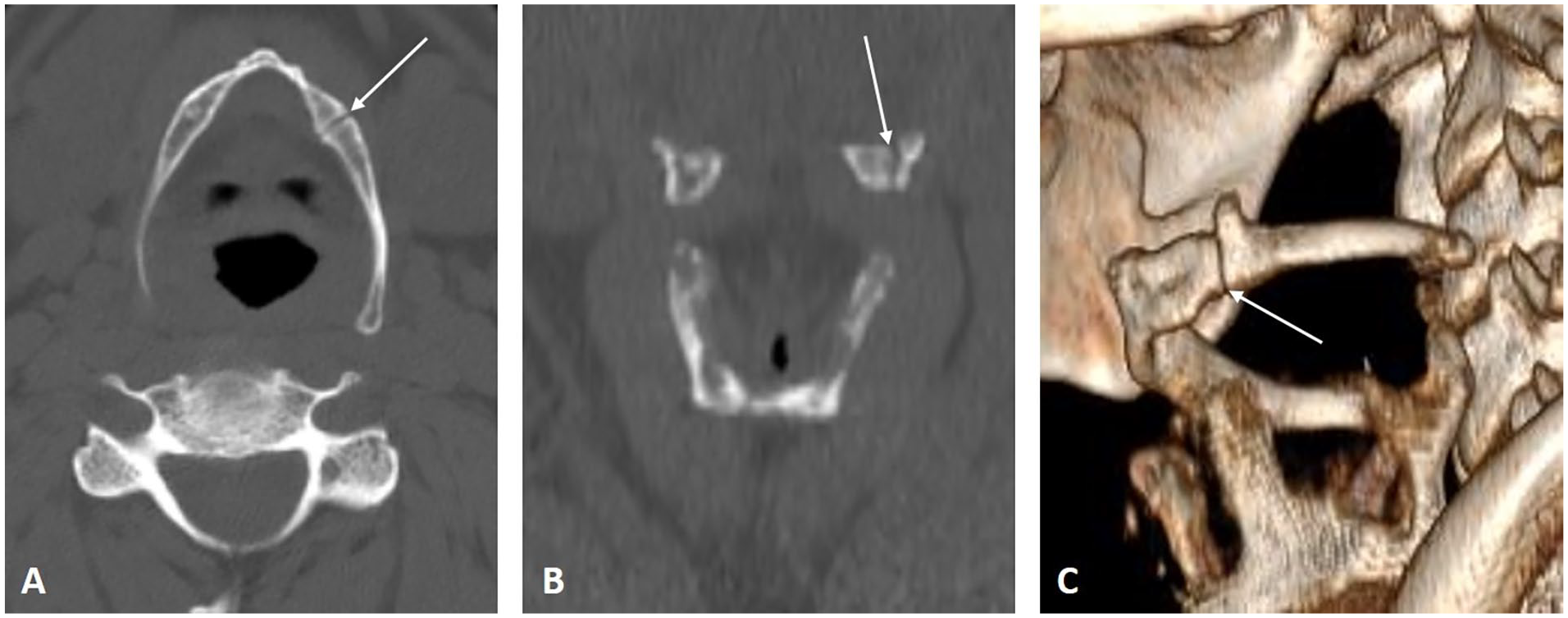
Cervical CT scan axial (A) and coronal (B) bony window slides with a 3D reconstruction (C) showing a fracture at the left side of the hyoid bone body (white arrows). CT, computed tomography.
Second Case
A 70-year-old male with a medical history of diabetes was a victim of a head and neck trauma following a traffic accident. He reported a neck pain without any associated symptoms. Physical examination revealed a sensibility at the lateral right cervical region without any cutaneous traumatic lesions. We did not observe any respiratory distress. Laryngeal endoscopy did not show any hematoma, laceration, or airway obstruction. CT scan revealed a displaced fracture of the greater right horn of the hyoid bone. It also showed a fracture of the right zygomatic process, the transverse process of C1 and C4 as well the process spinosus of C5 (Figure 2). The patient was monitored for 48 hours and was placed under antibiotics, steroids, and analgesics. He remained stable without any further clinical deterioration. Associated injuries did not require a surgical treatment either. Follow-up after 1 month was normal.
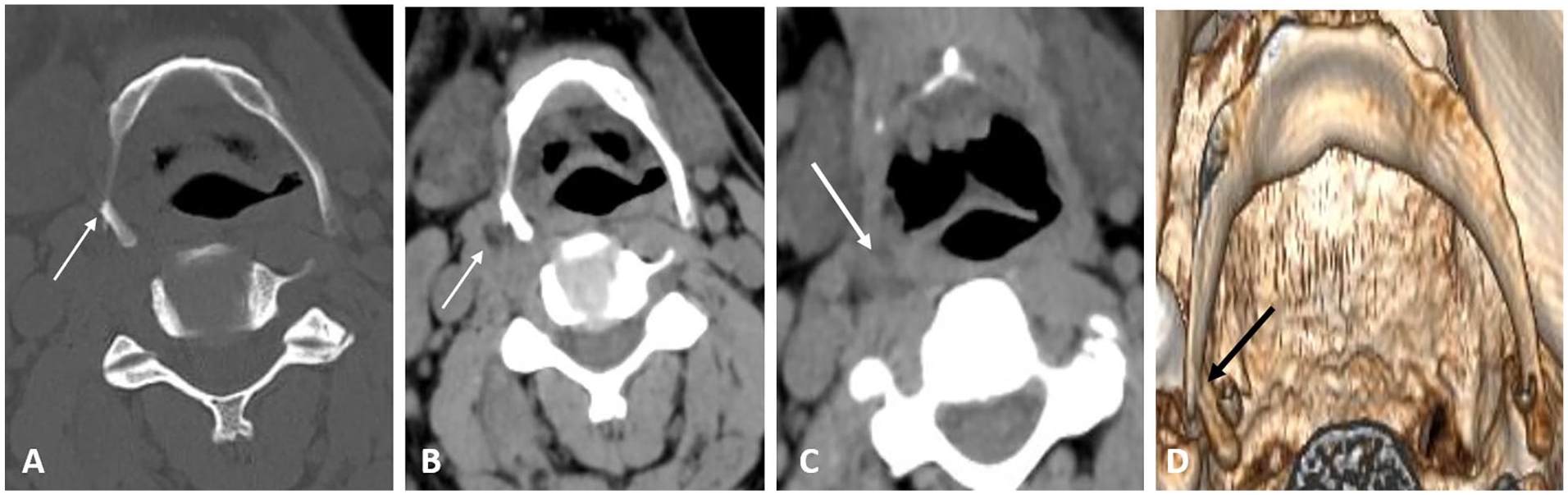
Cervical CT scan axial bony window slide (A) and soft tissue slides (B and C) with a 3D reconstruction (D) showing a fracture of the right greater horn of the hyoid bone with a median displacement of the fractured fragment (A: white arrow, D: black arrow). Densification of the adjacent soft tissues (B and C: white arrow). CT, computed tomography.
Discussion
Hyoid bone fractures unrelated to strangulation seldom occur.2,3 Etiologies other than strangulation are dominated by traffic accidents that cause neck hyperextension or an impact of the hyoid bone with the steering wheel or the dashboard.1,7 Other reported causes of hyoid bone fractures include assaults to the neck, hyperextension, explosions, gunshots, athletic activities, neck wounds, and falls. Fractures induced by vomiting efforts were also observed.6,8-11
The rarity of this entity is explained by various anatomical factors. The hyoid bone is anatomically protected by the protruded portion of the mandible anteriorolaterally and the cervical spine posteriorly.1,3 The mobility of the hyoid bone also minimizes the risk of fracture occurrence. The protection level is reinforced at a relaxed position of the neck.5,12 However, cervical hyperextension unbalances protection mechanisms by decreasing the protective role of the mandibular protrusion and increasing the tension of attached muscles, leading to a decreased hyoid bone mobility and making the bone more vulnerable to isolated fractures.1,3-5
The clinical presentation of hyoid bone fractures is heterogeneous. Complaints vary from subtle to severe. 4 Symptoms mainly appear immediately following the trauma, while a delayed onset is rather rare. 9 Our patients presented with either dysphagia or neck pain that appeared immediately following the trauma. The most commonly reported clinical manifestations include neck pain exasperated by coughing, swallowing, or head rotation, neck swelling, odynophagia, dysphonia, wheezing, coughing, and lump throat sensation.4-6,13 However, the most feared manifestation is respiratory distress; its severity varies from slight to fatal and life-threatening.6,9
Physical examination findings include anterior neck tenderness at palpation, neck swelling, subcutaneous emphysema, throat swelling, limited neck rotation, and bruises at the mouth mucosa or the neck especially in a trauma context.1,4,13 Laryngeal endoscopy reveals various lesions, such as hematoma, edema, laryngeal or pharyngeal lacerations, exposed laryngeal cartilages, airway obstruction, as well as the protrusion of the fractured hyoid bone at the pharyngeal wall.4,5 Moreover, using the Valsalva maneuver during laryngeal endoscopy ensures a better visualization of hyoid bone fractures since this maneuver causes a positive pressure which pushes the mobile hyoid bone segment into the pharyngeal wall, and makes its visualization easier.4,13 Laryngeal endoscopy revealed a laryngeal edema in one of our patients.
Hyoid bone fractures are rarely associated with a damage to the surrounding structures, such as mandibular, cervical, and facial fractures, as well as laryngeal and pharyngeal injuries.1,4 In the systematic review by Ramchand et al, 1 only 20 of the total 47 reported cases were associated with other injuries. In our patients, associated injuries included cervical spine and facial fractures, as well as acromioclavicular luxation. Other possible complications include vascular injuries by bony fragments, or more rarely, a neck abscess and carotid artery pseudoaneurysm.4,14,15
The diagnosis of hyoid bone fractures remains challenging and requires a high clinical suspicion because of its subtle and unspecific clinical presentation. 4 In earlier studies, hyoid bone fractures were diagnosed through lateral cervical X-rays, although their detection using this modality is difficult.1,2 More recently, CT scan of the neck has been the gold standard to confirm hyoid bone fractures.6,13 In addition, it helps rule out other possible associated injuries, such as mandibular, cervical spine, laryngeal, and pharyngeal injuries.5,10 However, a normal CT scan does not exclude the possibility of a hyoid bone fracture since it can, although rarely, miss the diagnosis. 13 Direct laryngoscopy is not routinely performed; its indications include dyspnea, hemoptysis, and laryngeal or pharyngeal lacerations. 6
The management of hyoid bone fractures remains not consensual due to their rarity. Treatment is either conservative or surgical. The choice of the adequate approach depends on symptoms severity and associated injuries and complications.1,3,6,13
Conservative treatment is the keystone of hyoid bone fractures, especially asymptomatic and closed fractures, unless the airways were not compromised.1,3,5,7 It is based on a 48 to 72 hour observation period to detect any clinical deterioration such as a compressive hematoma, edema, or acute respiratory distress, which can be fatal requiring an orotracheal intubation or tracheostomy.1,6,7 Conservative treatment involves liquid or semiliquid alimentation, neck rest, nasogastric tube placement in case of dysphagia, voice rest, as well as analgesics and antibiotics.1,2,5,10 The role of steroids in the treatment of edema caused by hyoid bone fractures was not well established, although its use was reported in some studies.5,7 However, while medical treatment ensures the resolution of symptoms, its effect on their long-term evolution remains unclear. 1 In agreement with the previous studies, both our patients were successfully managed through a 48 hour surveillance period along with steroids, antibiotics, and analgesics.
Surgical treatment is rarely required. Its indications were limited to patients presenting with airway compromise, laryngeal or pharyngeal lacerations, open hyoid bone fractures, and clinical deterioration under conservative treatment.1,6,13 Karna et al 7 reported a 5.2% rate of surgical treatment in their patients. Surgical management of acute airway obstruction is based on tracheostomy but may also require the drainage of pharyngeal and other neck spaces.1,2 Surgical treatment modalities also involve a thorough neck exploration, the repair and suture of pharyngeal lacerations caused by protruding fractured hyoid bone, and the resection of hyoid bone fragments.1-3,6 However, surgery does not systematically include the reduction or stabilization of the hyoid bone fracture, which was rather rarely reported.1,3,6
Following both conservative and surgical treatment, hyoid bone fractures have a good prognosis even without the union of the fractured bone. The resolution of symptoms occurs between 2 and 8 weeks. No further imaging is required during the follow-up.2,7 Both our patients presented a total resolution of their symptoms 2 weeks following the incident.
Conclusion
Hyoid bone fractures unrelated to strangulation are a very rare occurrence. Their clinical presentation is mainly subtle but can also be associated with a fatal and life-threatening presentation. Their diagnosis poses a challenge and requires a high clinical suspicion. It is based on CT scan. The therapeutic approach is not consensual but it mainly depends on the severity of symptoms. Management is most frequently conservative involving a close clinical surveillance with analgesics and antibiotics. Surgery is rarely indicated and is limited to severe presentations.
Footnotes
Acknowledgements
None
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from patients for their anonymized information to be published in this article.