
Abstract
Anaplastic thyroid cancer (ATC), a rare thyroid malignancy, accounts for only 5% of all thyroid cancers. However, it is the most aggressive form and has a very poor prognosis. Increasing evidence suggests that ATC arises from papillary thyroid carcinoma (PTC). However, the exact mechanism underlying this transformation remains unclear. In almost all cases, ATC originates within, but rarely outside, the thyroid gland. Transformation of metastatic PTC into ATC within the cervical lymph nodes is extremely rare. In this report, we present a rare case in a 63-year-old male patient who was initially diagnosed with PTC at his first hospital visit, which underwent anaplastic transformation in lymph node metastasis, and was subsequently diagnosed during the follow-up visit.
Main Points
This is a report of a 63-year-old male patient who was diagnosed during follow-up with a rare case involving anaplastic transformation of lymph node metastases after an initial diagnosis of papillary thyroid carcinoma (PTC).
To our knowledge, this is the first reported case of anaplastic transformation of a metastatic lymph node in the neck.
This anaplastic transformation is rare, and there is currently no consensus on treatment approaches; therefore, we recommend treatment approaches that include surgical excision, with the goal of achieving clear margins whenever possible, coupled with radiation therapy and possible application of chemotherapy as a neoadjuvant or adjuvant treatment.
Introduction
Papillary thyroid cancer (PTC), the most common thyroid malignancy, is associated with a relatively favorable prognosis. However, the transformation of PTC into anaplastic thyroid cancer (ATC) is rare and has an extremely poor prognosis. A recent analysis of a surveillance epidemiologic database on ATC conducted from 1986 to 2015 reported a median overall survival (OS) of 4 months, with a 6-month OS rate of 35%. 1 Disease-specific mortality rates ranged from 98% to 99%.2,3 Unlike PTC, which generally has a favorable prognosis and is primarily managed through surgery, patients with ATC typically present with a rapidly growing and invasive mass in the neck, involvement of regional cervical lymph nodes, and distant metastatic disease at the time of diagnosis in approximately half of patients. 4 Consequently, patients with ATC are often considered ineligible for surgery at presentation, which has historically led to palliative treatments or hospice referrals. The pathologic characteristics of ATC are determined by the combination of three primary histological patterns: spindle cell, giant cell, and squamoid. These patterns often coexist or present with a unihistologic feature. However, they have been employed to categorize ATC into significant histological groups and establish the primary differential diagnoses. Generally, cells of ATC do not exhibit immunohistochemical features for thyroglobulin, calcitonin, or the TTF-1 oncoprotein, suggesting a marker of thyroid carcinoma origin. The coexistence of PTC and ATC in the same patient is extremely rare. Furthermore, to our knowledge, cases in which anaplastic transformation of PTC occurs at lymph node metastases sites during follow-up despite an initial diagnosis of PTC have not yet been reported. Therefore, we report a case in which a patient was initially diagnosed with PTC and finally manifested anaplastic transformation.
Case Presentation
A 63-year-old man visited our outpatient clinic with a palpable, painless neck mass. The neck mass had been palpable for the past year, and the patient reported that it had rapidly increased in size over several weeks. He had a history of atrial fibrillation diagnosed 10 years earlier and had been taking medications, including warfarin and digoxin. The patient denied using alcohol and tobacco. On neck magnetic resonance imaging (MRI), a mass measuring 5 cm in size with strong heterogeneous enhancement was observed near the right parotid gland (Figure 1A). Following a core-needle biopsy, the pathological report indicated a malignant mass suggestive of PTC, including positive findings for the marker of thyroglobulin and thyroid transcription factor-1 (TTF-1). Positron emission tomography-computed tomography (PET-CT) was performed to evaluate the metastasis, which revealed focal small hypermetabolic activity with calcification in the right thyroid and evidence of right lateral lymph node metastasis (Figure 1B and C). Fine needle aspiration of the right thyroid gland and neck nodes confirmed the diagnosis of PTC and lymph node metastasis. The patient underwent definitive resection surgery, including total thyroidectomy and dissection of the central and right lateral neck. The final histopathological examination confirmed a well-differentiated PTC with microscopic extrathyroid extension (Figure 2A), together with the presence of multiple lateral neck lymph node metastases (Figure 2B). Multiple lateral neck lymph node metastases of thyroid origin were identified through positive immunohistochemistry results of TTF-1 and Thyroglobulin.
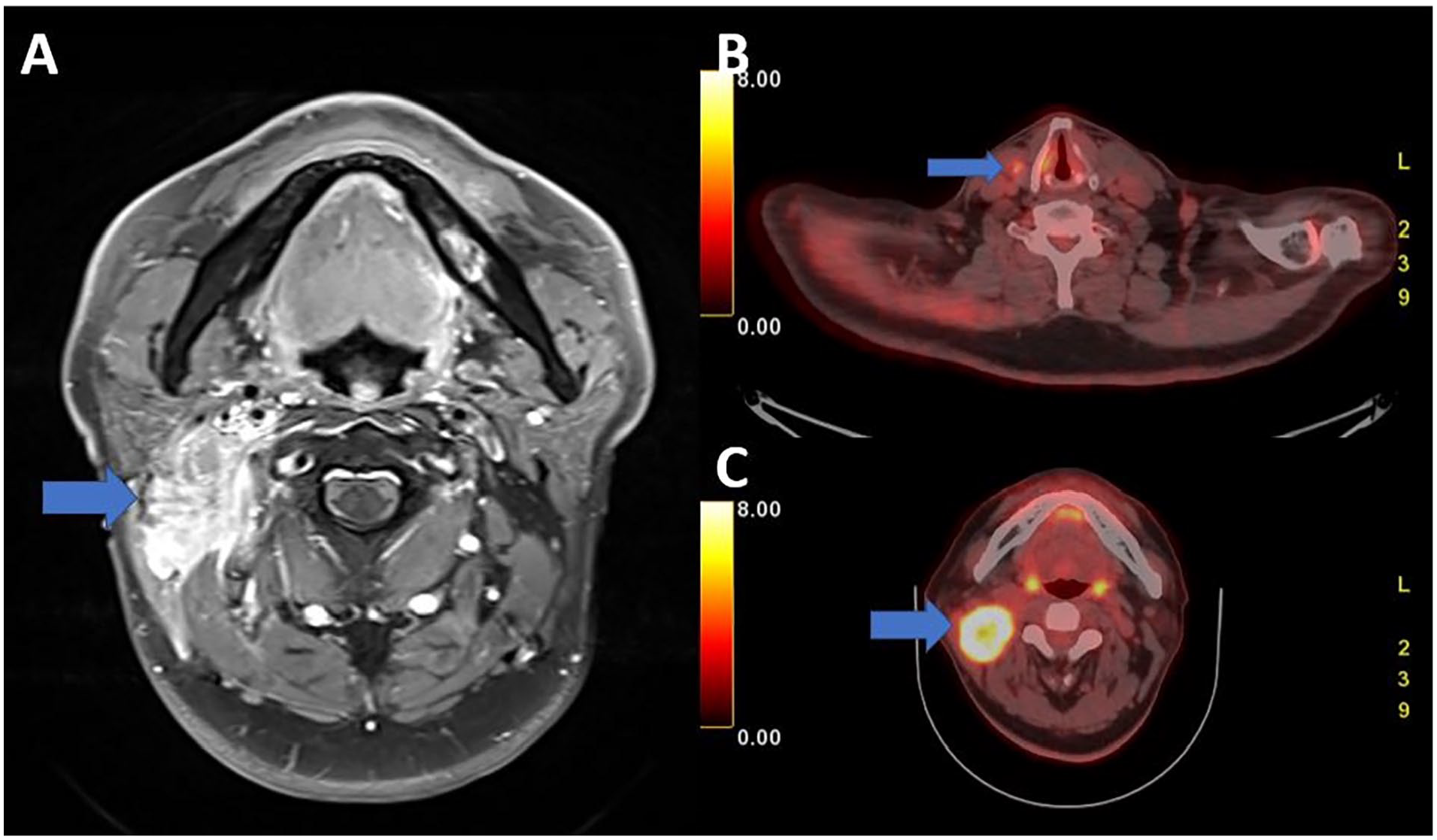
(A) MRI T1 axial enhanced image shows a strong, heterogeneous enhancing mass lesion at the parotid site. (B) Positron emission tomography computed tomography (PET-CT) shows focal small hypermetabolic activity with calcification in right thyroid gland. (C) PET-CT shows hypermetabolic enlarged mass on right neck level II.
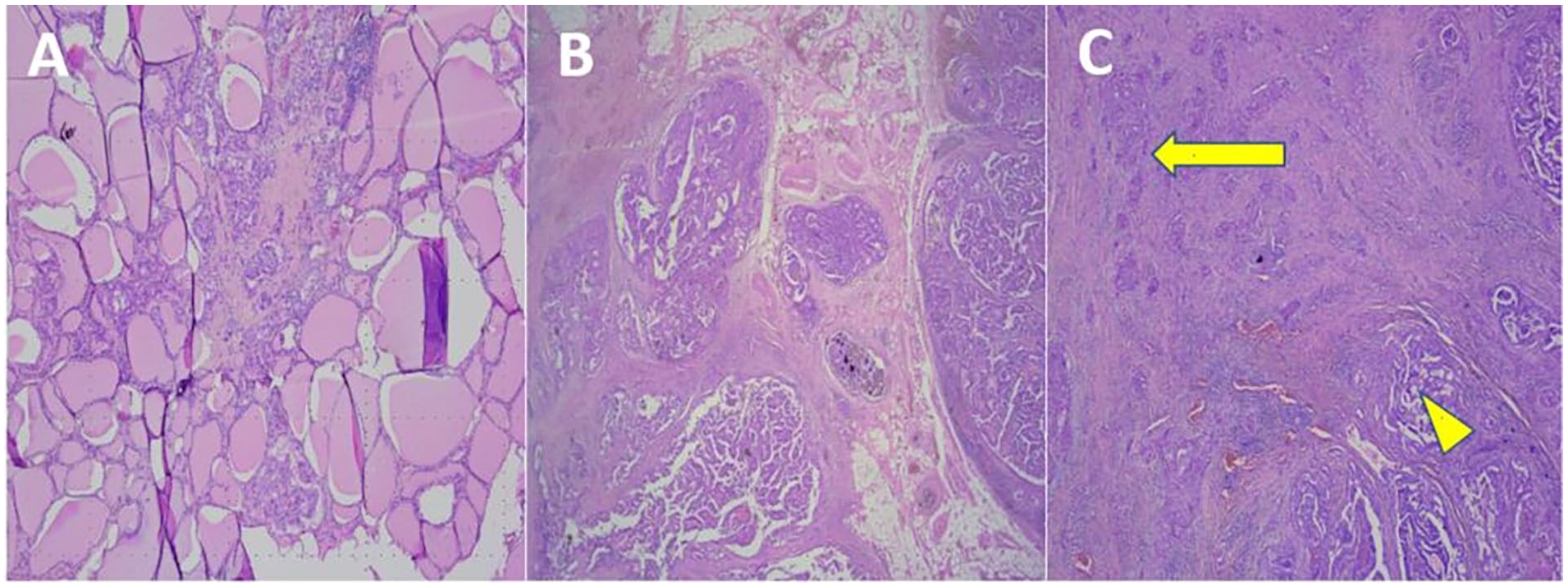
(A) Surrounding the cystic-shaped normal thyroid tissue is the evidence of papillary thyroid carcinoma (PTC). (B) Metastasis of papillary-like form of PTC to the lymph node was confirmed based on evidence of invasion into the surrounding tissues. (C) A progression that naturally transitions from papillary thyroid cancer is observed. Squamous differentiation (yellow arrow). Typical papillary thyroid cancer (yellow arrowhead).
During follow-up observation, 2 months after initial surgery, the patient visited our clinic due to a recurrent neck mass. Therefore, we performed a computed tomography (CT) scan, which revealed the recurrence of a 3 cm-sized neck mass near the previous neck operation site. Subsequently, a secondary surgery was performed as a radical neck dissection. Pathological examination during the second surgery revealed differentiated PTC tissue along with coexisting squamous differentiation (Figure 2C). Histoimmunochemical results of neck mass showed TTF-1 negative and P63 positive, also suggesting squamous differentiation. We conducted comprehensive cervical physical examinations, including examination of the skin, tonsils, oropharynx, and esophagus, along with neck MRI and PET-CT scans to differentiate it from metastatic lymph nodes originating from primary squamous cell carcinoma in the neck area. However, no primary focus was identified in other areas, which implies the diagnosis of anaplastic transformation of PTC.
Taking into account ATC, concurrent chemoradiotherapy (CCRT) was planned as a palliative treatment. However, during preparation for CCRT, a pus-like discharge oozed from the surgical site on the right side of the neck, prompting the administration of antibiotics. Despite antibiotic use, the neck discharge persisted, and the wound area gradually enlarged. On the neck CT scan, a 7 cm heterogeneous enhancing mass was observed at the right neck operation site (Figure 3). Following local anesthesia, histopathological examination, including examination of cervical tissue with purulent discharge, revealed poorly differentiated squamous cell carcinoma with necrotic features. Furthermore, thoracic CT, performed to assess thyroid cancer metastasis, revealed the existence of several small solitary lung nodules (<0.5 cm). Unfortunately, the patient’s condition deteriorated during the course of radiotherapy, eventually leading to death, due to sepsis resulting from pneumonia.
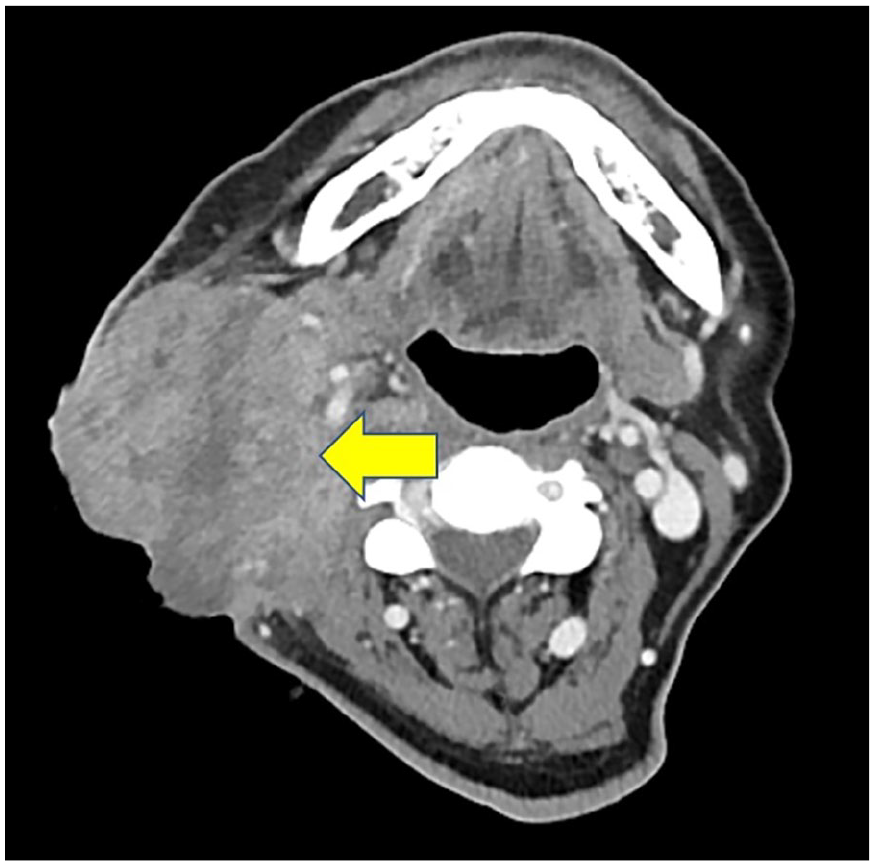
Computed tomography axial enhanced image shows a heterogeneous enhancing mass lesion at the previous operation site.
Discussion
According to the fifth edition of the World Health Organization on the classification of thyroid neoplasms, squamous cell differentiation of differentiated thyroid cancer is classified as a subtype of anaplastic thyroid carcinoma. 5 The hypothesis that ATC transforms from PTC has been proposed because of the coexistence of poorly and well-differentiated tumors in thyroid neoplasms. Currently, there is no standardized technique for predicting which thyroid neoplasm will undergo anaplastic transformation. Several hypotheses have been proposed regarding the mechanism of anaplastic transformation in PTC. 6 The first involves genetic mutation, where the presence of genetic mutations such as genes in the BRAF, TERT, RAS, TP53, and Wnt pathway can lead to the development of ATC. Other research has indicated that being over 65 years old and having a history of radiation exposure to the neck and prolonged goiter, as possible risk factors for ATC, suggesting that the combination of these factors can contribute to the appearance of the transformation to ATC.
Our case involving a 63-year-old male patient with a poorly differentiated thyroid tumor is particularly interesting and provides valuable information. Although initially diagnosed with well-differentiated thyroid cancer, this patient experienced a rapidly growing neck mass as an unexpected transformation into ATC for reasons that remain unclear. Examination of the patient’s tissue sample revealed the coexistence of anaplastic tumor and PTC marked by a transition zone. The pathological connection between PTC components and anaplastic tumors suggests the existence of a linkage, implying a type of progression as a sequel of malignant transformation. In actual clinical practice, a comprehensive reassessment is necessary when the clinical course differs from the expected progression. In cases in which indolent cancers such as PTC exhibit aggressive behavior, the possibility of transformation into ATC should also be considered.
Squamous transformation is rare and has only been documented in a few case reports.7-9 However, these cases occur mainly within the thyroid itself. To our knowledge, this is the first reported case of anaplastic transformation of a metastatic lymph node in the neck. Due to the rarity of such anaplastic transformations, there is currently no consensus on treatment approaches. Therapeutic options include surgical excision, with the goal of achieving clear margins whenever possible, coupled with radiation therapy and the potential application of chemotherapy as a neoadjuvant or adjuvant treatment.
Conclusions
Here, we report a case of anaplastic transformation in a patient with PTC. Unlike previously reported cases, this case demonstrates the possibility of anaplastic transformation, even in metastatic lymph nodes. In this case, it is evident that when rapid deterioration of metastatic lesions is observed in patients with PTC, differential diagnoses such as anaplastic transformation should be considered.
Footnotes
A Data Availability Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research funds from Chosun University Hospital (2023).
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki of the World Medical Association. This study was approved by the Institutional Review Board of the Chosun University Hospital (IRB No. 2023-08-017).
Informed Consent
Informed consent was not required because the photographs did not allow identification of the patient.