
Abstract
Sarcoidosis is a systemic inflammatory disease characterized by the formation of immune granulomas in multiple organs. The cause of this disease is not yet clear. Papillary thyroid cancer (PTC) is the most common malignant endocrine tumor and is often associated with cervical lymph node metastasis. Assessment of risk factors associated with a poor prognosis is crucial in PTC. The coexistence of sarcoidosis and thyroid cancer is rarely reported in the literature. We describe a case of a 54-year-old female diagnosed with PTC and asymptomatic cervical and thoracic hilar lymphadenopathy due to concurrent sarcoidosis. This case will remind clinicians to be aware of the multiple potential causes of lymphadenopathy and realize the importance of the differences in the features of neck lymphadenopathy in patients with suspected head and neck cancer. Overall, careful workup and pretreatment screening enabled us to provide the patient with the most suitable treatment modality and avoid total thyroidectomy.
Keywords
Introduction
Sarcoidosis is a condition characterized by the development of immune granulomas in various organs, such as the lungs (in 90% of cases), lymph nodes, eyes, and skin. The disease affects the entire body and its cause is still unknown.1 -5 Sarcoidosis can occur in individuals of any race, sex, and age, although it is most commonly diagnosed in patients aged between 25 and 45 years; this age group accounts for almost 70% of cases. 1 The diagnosis of sarcoidosis is based on consistent clinical and radiological findings, and is further supported by the presence of no-caseating epithelial cell granulomas in 1 or more organs without evidence of microorganisms or foreign particles. 6 Respiratory symptoms, fatigue, night sweats, weight loss, and erythema nodosum are among the most frequently observed clinical manifestations. 6 However, 50% of patients with sarcoidosis have no symptoms. 6 Bilateral hilar lymphadenopathy or diffuse micronodular pulmonary infiltrates on chest radiography are the most common radiologic findings. Biopsy is required in all patients with suspected sarcoidosis, except those with Lofgren syndrome. 6 Furthermore, sarcoidosis has been reported to be associated with malignancy. Sarcoidosis and cancer can occur together. Cervical lymphadenopathy in patients with cervical nodule granuloma and papillary thyroid cancer (PTC) presents a diagnostic challenge. We present a case of PTC coexisting with asymptomatic cervical and hilar lymphadenopathy and sarcoidosis.
Case Presentation
A 54-year-old female patient with a family history of thyroid cancer visited our ENT outpatient department to follow-up on her thyroid ultrasound. She denied any symptoms, such as cough, fever, weight loss, fatigue, or dyspnea. A physical examination revealed a palpable mass in the right lower central neck area without splenomegaly or hepatomegaly. An ultrasound of the neck reveled a solid nodule of approximately 1.28 cm × 1.05 cm × 1.41 cm with an irregular margin and marked hypoechogenicity (CR TI-RADS 4C, American College of Radiology Thyroid imaging reporting and data system 4C; for the TI-RADS classification, each ultrasound feature received point(s) according to the 2017 ACR TI-RADS publication. 4C (6 points, means high suspicious for malignancy)) in the right lobe of the thyroid. Fine needle aspiration was performed and cytology was suspicious for papillary carcinoma. Laboratory analyses indicated normal thyroid function without related autoantibodies [T3 = 94.3 ng/dL, normal range 72-172 ng/dL; free T4 = 0.83 ng/dL, normal range 0.59-1.43 ng/dL; thyroid‑stimulating hormone (TSH) = 1.019 μIU/mL, normal range 0.38-5.33 μIU/mL]. A chest radiograph detected enlarged bilateral hilar masses (Figure 1). Head and neck computed tomography (CT) scan revealed a mass of about 1.4 cm in diameter on the right side of the thyroid and an enlarged neck lymph nodes over level VI and VII of a suspected metastatic neck lymph node (Figure 2). Chest CT scan showed multiple enlarged lymph nodes in the mediastinum and bilateral hilum, suggesting a diagnosis of metastatic lymphadenopathy. However, according to the thyroid sonography findings of a small primary lesion without obvious lateral neck nodal metastases, as well as the growth pattern of the bilateral hilar lymphadenopathy, abundant central neck lymph node metastases with lung metastases were unlikely. Therefore, after thorough discussion with the patient, she underwent right thyroidectomy and isthmusectomy, central neck dissection (right level VI), and excisional biopsy of the neck level VII lymph nodes to prepare frozen sections. Pathology confirmed PTC without lymph node metastasis and also revealed a noncaseating granuloma in the right level VII lymph nodes (Figure 3). The level VII lymph node excision was negative for acid-fast bacilli stain. A whole-body gallium-67 (67Ga) scan performed after surgery revealed symmetric uptake of 67Ga by the bilateral lacrimal glands and the parotid glands, consistent with the “panda sign” (Figure 4A). In addition, the “lambda sign” was demonstrated by increased 67Ga uptake in the mediastinal, paratracheal, and hilar lymph nodes (Figure 4B). Sarcoidosis was strongly suspected based on the clinical and imaging findings. Therefore, we prescribed oral prednisolone at a dose of 10 mg/day. Subsequent chest radiographs at 1 and 3 months showed a partial response in the bilateral hilar lymph nodes. At 6 month follow-up, the patient was asymptomatic and had no palpable lymph nodes.
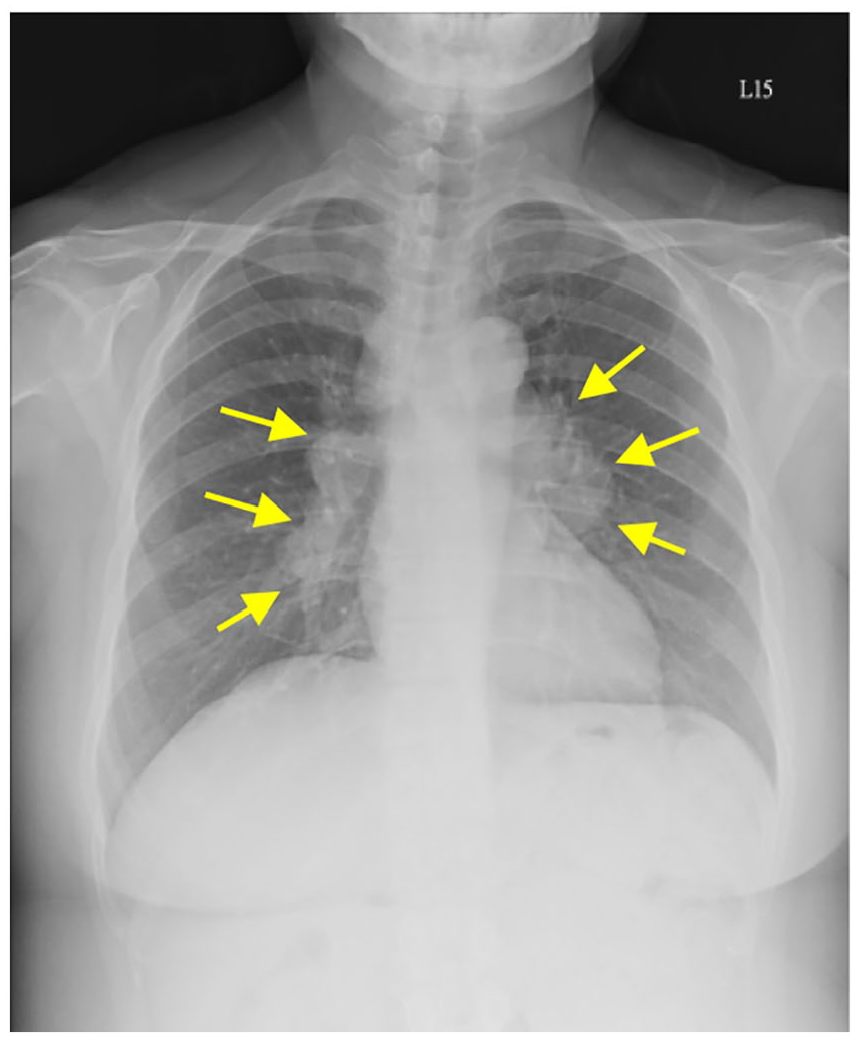
Chest radiograph showed bilateral hilar lymphadenopathy (arrows).
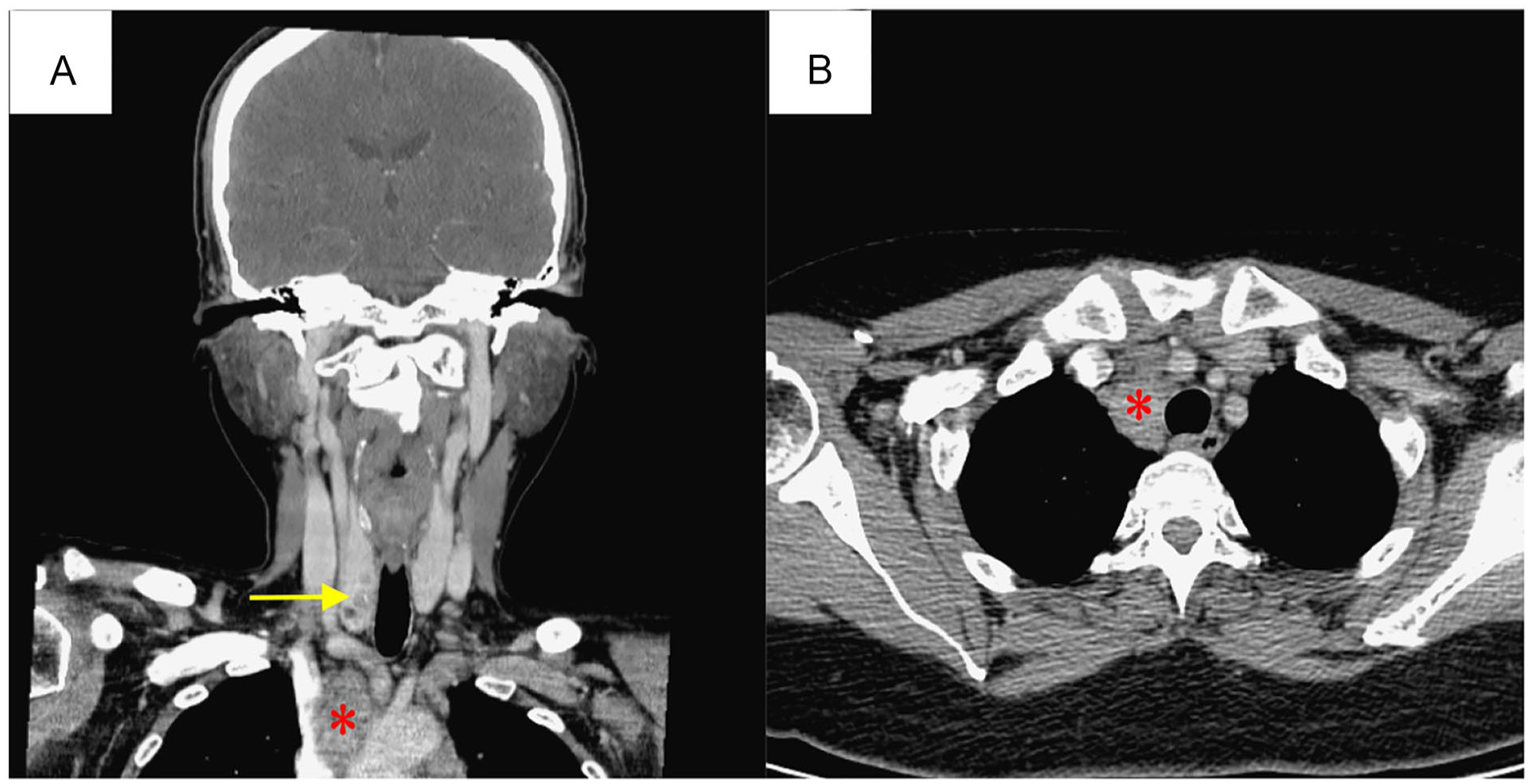
(A) Coronal enhanced neck CT images showed a right thyroid mass/lesion (arrow) and enlarged lymph nodes at level VII (asterisk). (B) Axial enhanced neck CT images showed enlarged lymph nodes at level VII (asterisk) and the mediastinum. CT, computed tomography.
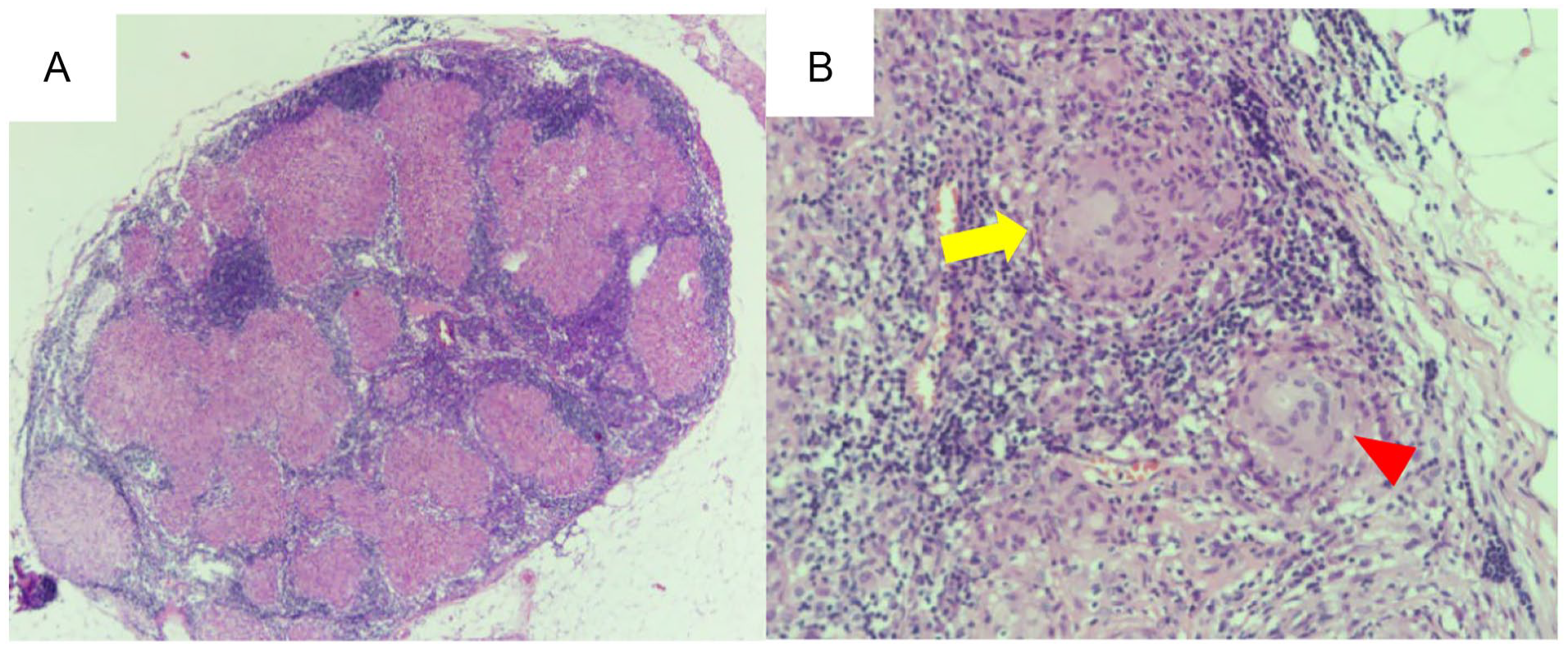
(A) Numerous noncaseating granulomatous lesions were detected in the lymph nodes (H&E stain, ×40). (B) High magnification of (A) showing the granuloma mainly consisted of epithelioid cells with Langhan’s cells (arrows) and foreign body-type giant cells (arrowhead); (H&E stain, ×200). H&E, hematoxylin and eosin.
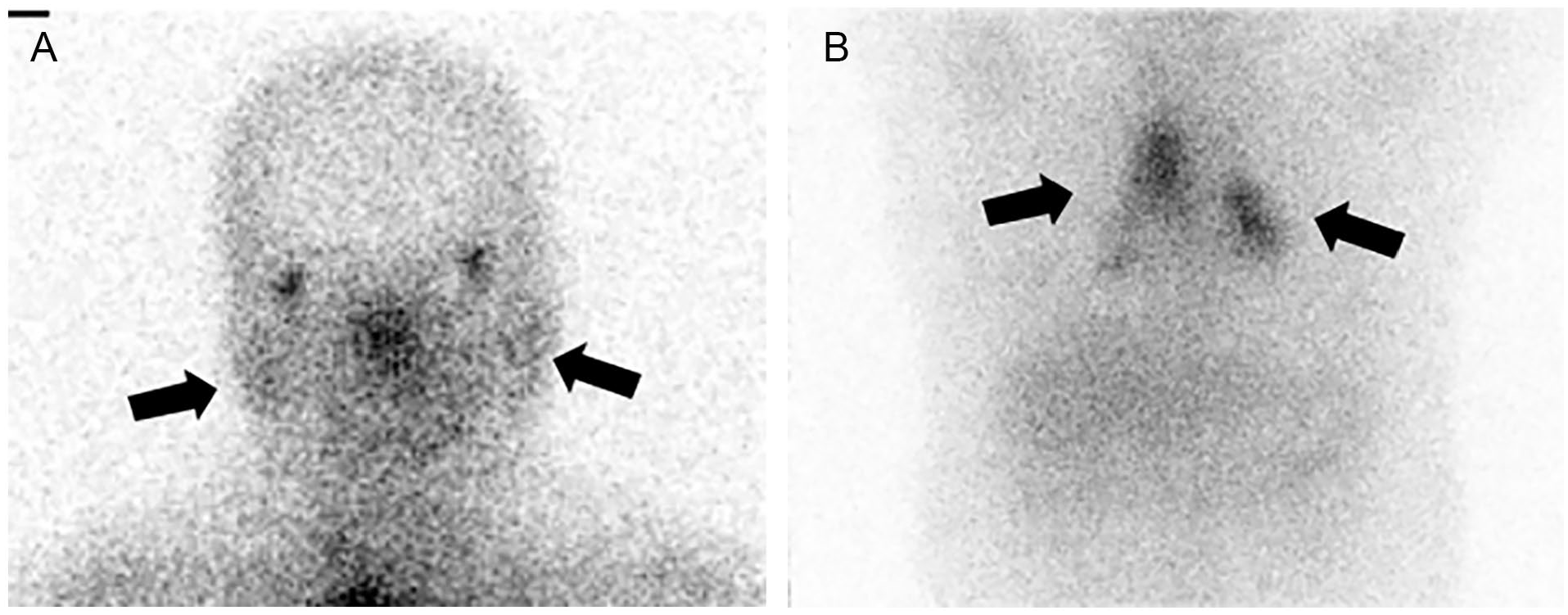
(A) A 67Ga scan showed symmetrical uptake of 67Ga in the nasopharynx, lacrimal glands, and parotid glands, revealing the “panda sign” (A, arrows). (B) Increased 67Ga uptake in the paratracheal and hilar lymph nodes revealed the “lambda sign” (B, arrows). 67Ga, gallium-67.
Discussion
Sarcoidosis is a systemic inflammatory disease distinguished by the presence of noncaseating granulomas, which are composed of macrophages, lymphocytes, and epithelioid giant cells.2,6,7
Most studies suggest that patients with pulmonary sarcoidosis tend to develop malignancy, but other reports suggest that malignancy causes sarcoidosis. 8 Treatment of coexisting PTC and sarcoidosis can be difficult because these diseases affect the same organs and have very similar morbidity rates.
Thyroid cancer is the most common malignant endocrine tumor and 80% to 85% of thyroid cancers are PTC. 9 Cervical lymph node metastasis is a major risk factor for recurrence in patients with PTC. Several studies have reported several other significant risk factors for lymph node metastasis in PTC, including age ≤45 years, male sex, tumor size >1.0 cm, tumor located in the upper third of the lobe, capsular invasion, extra thyroidal extension, and sonographic features as microcalcification.9,10 The sole determinant of risk in this scenario is the size of the tumor, with a measurement of 1 cm or greater associated with a higher risk of cervical lymph node metastasis.
The most common site of distant metastasis site for PTC is the lungs. 11 Pulmonary metastases from thyroid cancer usually appear as micronodular or miliary patterns in both lungs; nodular lung metastases of 10 mm in diameter are very rare. 12 However, pulmonary sarcoidosis can exhibit different radiographic patterns. The most common features of pulmonary sarcoidosis are bilateral intrathoracic hilar lymphadenopathy or diffuse micronodular pulmonary infiltrates. Therefore, PTC with pulmonary metastases was less likely in our case, and concomitant pulmonary sarcoidosis was strongly suspected based on chest CT scan.
Sarcoidosis can affect any organ. Many studies have reported that the lungs, mediastinal, and hilar lymph nodes are most commonly involved in sarcoidosis.1 -5 The prevalence of peripheral lymphadenopathy in sarcoidosis is 10% to 20%, mostly affecting the cervical or supraclavicular lymph nodes. Furthermore, a few cases have been reported in which sarcoidosis presented with cervical lymph node enlargement without mediastinal or lung abnormalities.6,13
Conclusion
Patients with PTC commonly develop cervical nodal metastases and the most common site of distant metastases is the lung. However, the metastatic pattern in the lungs is typically of the micronodular or military type in thyroid cancer. Therefore, it is important for clinicians to carefully consider whether the pattern of the lymph nodes at presentation is unusual in patients with suspected PTC to detect or exclude another coexisting disease. In this case, the coexistence of sarcoidosis was confirmed by the final pathology and the patient could avoid total thyroidectomy due to their low-risk thyroid cancer status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.