
Abstract
Objective:
To compare graft outcomes and postoperative complications between the extended perichondrium-cartilage butterfly inlay (PCBI) technique and the perichondrium-cartilage over-underlay (PCOU) technique for repairing subtotal perforations over a 2-year follow-up period.
Methods and Materials:
Patients with subtotal perforations were prospectively randomized to either the extended PCBI (n = 52) or PCOU (n = 51) group. Evaluation metrics included operation time, graft success rate, hearing gain, and complications at 24 months postoperatively.
Results:
The study included 103 patients with 103 ears. Follow-up loss occurred in 11 of 52 patients (21.2%) in the PCBI group and 13 of 51 patients (25.5%) in the PCOU group (P = .773). The final analysis included 41 of 52 patients (78.9%) in the PCBI group and 38 of 51 patients (74.5%) in the PCOU group. The average operation time was significantly shorter in the PCBI group (31.2 ± 1.9 min) compared to the PCOU group (52.8 ± 6.3 min, P < .001). At 24 months postoperatively, the graft success rate was 82.9% (34 patients) in the PCBI group and 92.1% (35 patients) in the PCOU group (P = .374). No significant group difference was noted in mean air–bone gap (ABG) gain (P = .759). High-resolution computed tomography (HRCT) demonstrated well-pneumatized mastoids and middle ears in both groups. Altered taste was reported in no PCBI group patients and 23.7% (9 patients) of the PCOU group patients (P < .05). Graft cholesteatoma was found in 4.9% (two patients) in the PCBI group and 7.9% (three patients) in the PCOU group (P = .930).
Conclusion:
The endoscopic extended PCBI technique is safe and effective for repairing subtotal perforation. It avoids raising a tympanomeatal flap and demonstrates high long-term graft success with minimal complications.
Introduction
Myringoplasty, used in the treatment of chronic perforations, typically results in satisfactory healing and hearing outcomes. However, when applied to subtotal perforations, the procedure often involves the raising a tympanomeatal flap. This can lead to several complications, such as damage to the chorda tympani nerve (CTN), stenosis of the external auditory canal (EAC), iatrogenic cholesteatoma, slow healing, and extended operation times.1,2 Since Eavey introduced the cartilage butterfly inlay technique in 1998, 3 it has been recommended for repairing tympanic membrane (TM) perforations.4-9 “Butterfly” refers to the shape of the cartilage graft, which resembles butterfly wings and is inserted into the TM to close the perforations, akin to an ear tube. 3 This technique, known for its practicality and effectiveness, does not require the raising of a tympanomeatal flap. However, it requires accurate assessment of the perforation size and meticulous preparation of the cartilage graft. Otherwise, there is a high risk of graft failure. Moreover, the technique is challenging for beginners, with studies indicating wide variation in graft success rates, ranging from 43% to 100%. 10
Recently, an extended perichondrium-cartilage butterfly inlay (PCBI) technique was developed to repair subtotal perforations. In this method, the perichondrium, resembling a “lateral” butterfly wing, is elevated circumferentially, remaining attached to the cartilage. This perichondrium overlay directly covers the epithelial layer, whereas the cartilage, acting as the medial wing, is placed under the TM remnant. The circular gap between the perichondrium and the cartilage resembles the circular groove of the butterfly technique, grasping the perforation margins. This study aims to compare graft outcomes and postoperative complications between the extended PCBI technique and the perichondrium-cartilage over-underlay (PCOU) technique, when applied to repair subtotal perforations, over a 2-year follow-up period.
Materials and Methods
Ethical Considerations
The study protocol received approval from the Institutional Ethical Review Board of Wenzhou Medical University Affiliated Yiwu Hospital. Informed consent was obtained from all participants.
Methods
Study subjects were selected from among consecutive adult patients diagnosed with chronic large perforations at the Department of Otorhinolaryngology, Head and Neck Surgery. The inclusion criteria were aged >18 years, chronic subtotal perforation covering >75% of the TM area, a dry ear for ≥3 months, and good pneumatization of the middle ear and mastoid region on high-resolution computed tomography (HRCT). The exclusion criteria were suspected ossicular chain disruption, cholesteatoma, middle ear inflammation, revision cases, and fungal otitis externa. Dry ear status was determined based on patient history rather than monitoring the ear for 3 months post-enrollment. HRCT and audiograms were performed for all patients prior to enrollment. The assessment of ossicular chain damage involved evaluating audiometric data for conductive hearing loss >40 dB at any frequency, reviewing HRCT for ossicular chain abnormalities, and intraoperative endoscopic exploration.
Audiometric data were collected both before and 24 months after surgery. Pure-tone averages (PTAs) were calculated using the findings at 500, 1000, 2000, and 3000 Hz for both air conduction and bone conduction (BC). For many patients, a threshold of 4000 Hz was utilized to interpolate the threshold at 3,000 Hz, as recommended by the Hearing Committee of the American Academy of Otolaryngology–Head and Neck Surgery. Pre- and postoperative air–bone gaps (ABGs) were determined by subtracting air-conduction PTAs from bone-conduction PTAs. The extent of closure of the ABG corresponded to the difference between the preoperative and postoperative ABG.
Randomization and Blinding
All patients underwent endoscopic cartilage underlay myringoplasty, performed by the same surgeon using total intravenous anesthesia. Patients were randomly divided into two groups using the block randomization method. For group allocation, a sealed envelope system was used, with patients assigned to either the extended PCBI or PCOU group. Both the patients and the assessor were blinded to the treatment arm.
Surgical Technique
All patients underwent endoscopic perichondrium-cartilage myringoplasty under total intravenous anesthesia. Cartilage with a single-layer perichondrium composite graft was harvested from the ipsilateral tragus. Lateral support of the graft was provided by biodegradable synthetic polyurethane foam packing. The cartilage was then packed with antibiotic-soaked gauze, extending up to the tragus incision.
Extended PCBI Technique
The PCBI technique does not require the raising of a tympanomeatal flap. Under a 0° rigid endoscope, the perforation edges were freshed, removing the epithelium around the malleus handle while preserving the epithelial layer of the TM remnant and myringosclerosis.
The perichondrium was elevated circumferentially, maintaining its attachment to the cartilage. The cartilage graft was shaped according to the size of the perforation, and we ensured that it was approximately 1 mm larger than the perforation margins. Similarly, the raising perichondrium flap was shaped to be at least 2–3 mm larger than the cartilage graft (Figure 1). A notch was then created in the cartilage graft to accommodate the malleus handle if any.
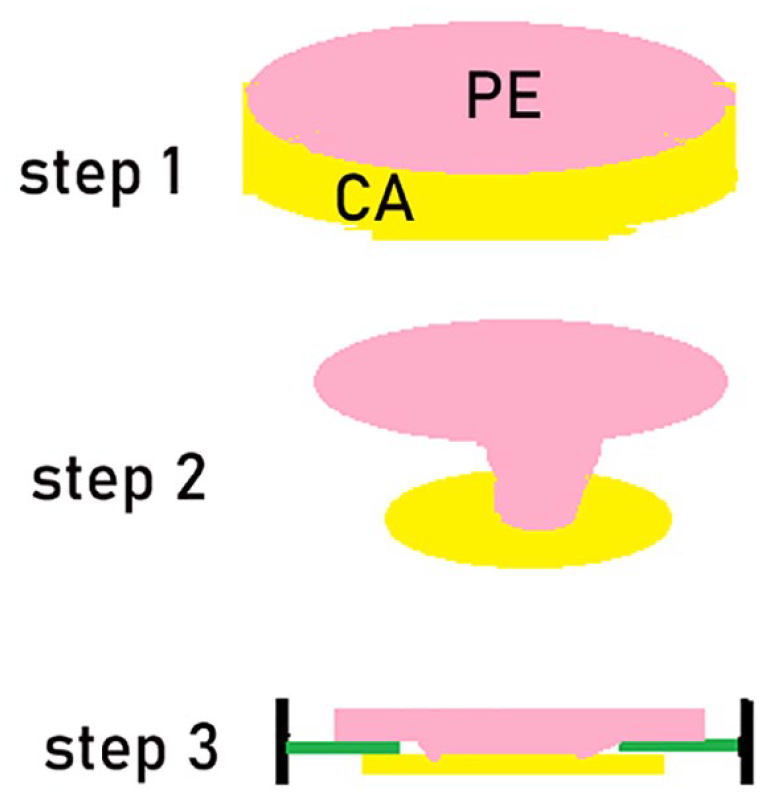
Schematic diagram of the PCBI technique. Step 1: harvesting of the cartilage with a single-layer perichondrium composite graft; step 2: circumferential elevation of the perichondrium with the pedicle attached to the cartilage; step 3: placement of the cartilage graft medial to the TM remnant with the perichondrium overlaying the epithelial layer of the TM remnant. CA, cartilage; PCBI, perichondrium-cartilage butterfly inlay; PE, perichondrium.
The middle ear was packed using biodegradable synthetic polyurethane foam packing (Stryker Canada, Hamilton, ON, Canada). The cartilage graft was placed transperforation, medial to the annulus and the TM remnant with the perichondrium directly overlaying the epithelial layer of the TM remnant, the malleus, and the annulus (Figure 2). Care was taken to avoid excessive perichondrium, which could form folds. Additionally, the perichondrium did not completely cover the TM remnant or the annulus, allowing the TM epithelium to continue shedding. Lateral support for the graft was provided by biodegradable synthetic polyurethane foam packing. Finally, the cartilage was packed with antibiotic-soaked gauze, extending up to the tragus incision.
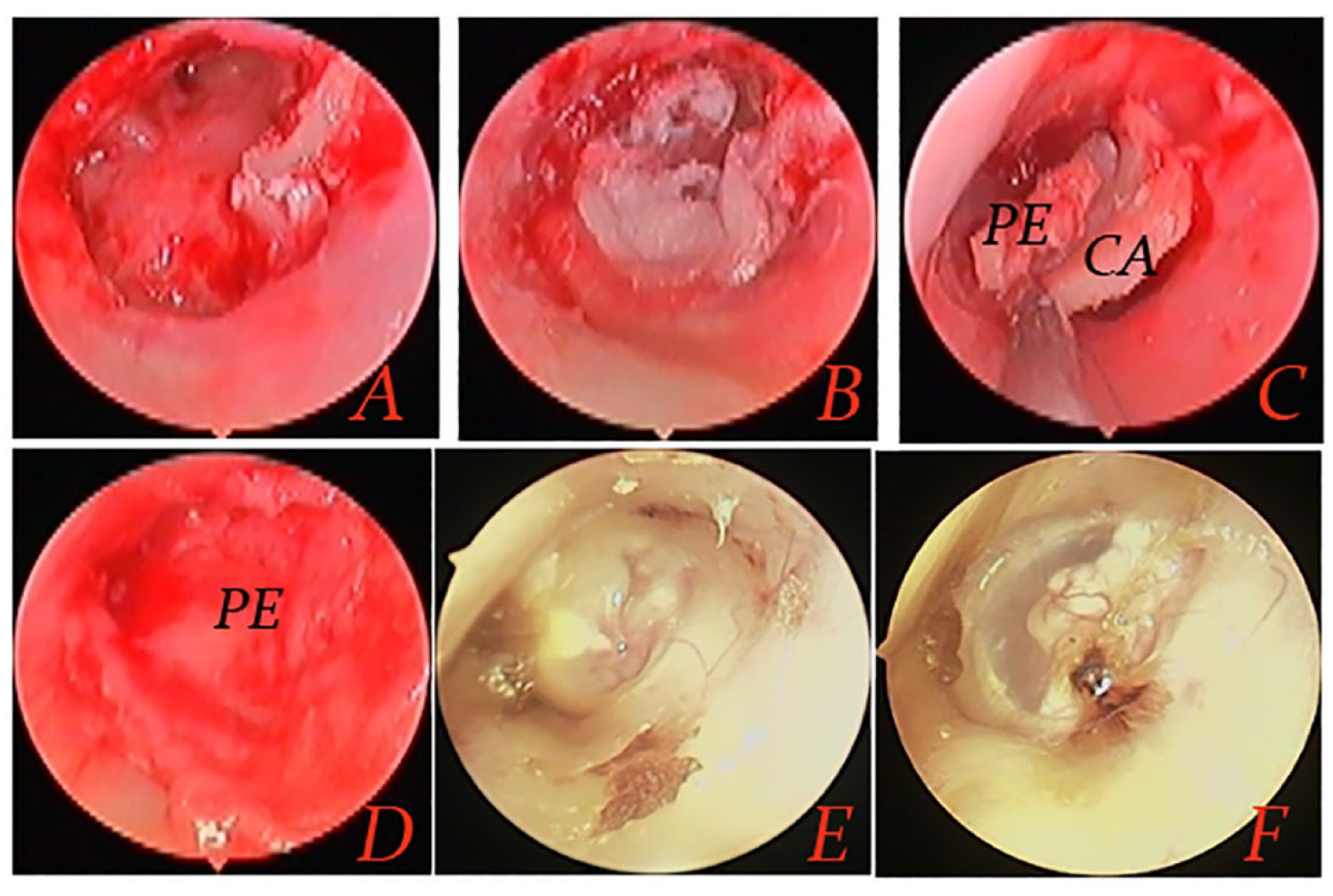
PCBI technique. (A) De-epithelialization of the perforation margin, (B) middle ear packing, (C) placement of the cartilage-perichondrium graft, (D) the perichondrium overlaying the epithelial layer of the TM, (E) 5 weeks after surgery, and (F) 6 months after surgery. CA, cartilage; PCBI, perichondrium-cartilage butterfly inlay; PE, perichondrium.
PCOU Technique
In PCOU group patients, the technique has been described by previous authors. 11 Raising tympanomeatal flap was applied and the perforation margin was freshly prepared. The middle ear was accessed by identifying and elevating the annulus, with the TM remnant being lifted until the long process of the malleus was visible. However, the anterior annulus was not elevated.
The lateral perichondrium was circumferentially peeled and rolled up, maintaining its attachment to the cartilage. The cartilage graft was tailored to be 1 mm more than the perforation margins. The free perichondrium was then trimmed to be ≥2 mm wider than the cartilage graft. A notch in the cartilage was made to accommodate the malleus handle if any. The middle ear was packed using biodegradable synthetic polyurethane foam packing (Stryker Canada).
The cartilage-perichondrium graft was inserted into the middle ear. The cartilage was positioned medial to the TM remnant and annulus, and the cartilage graft’s notch was aligned with the malleus handle. The free perichondrium was placed lateral to the long process of the malleus and medial to the TM remnant and tympanomeatal flap. Subsequently, the tympanomeatal flap was repositioned.
Postoperative Follow-up
Patients were discharged the day after surgery. Follow-up appointments were scheduled at 4 weeks, and at 3, 6, 12, and 24 months postoperatively. During each visit, graft status was endoscopically examined, and patients were questioned about any changes in taste, vertigo, or tinnitus. Follow-ups were conducted by a surgeon not involved in the initial operation. Audiometric evaluations were carried out at the end of the 24th postoperative month to measure ABGs. All postoperative complications were documented, including graft infection, atelectasis, graft lateralization, significant blunting, and medialization. Graft success was defined as an intact graft without residual or reperforation. HRCT was reassessed at 2 years postoperatively, and magnetic resonance imaging was ordered if HRCT indicated “lump shadows” in the mastoids and middle ear. The operative time was defined as the period from the harvesting of the graft to the packing of the EAC.
Statistical Analysis
Statistical analyses were conducted using SPSS software (version 21.0; SPSS Inc., Chicago, IL, USA). Data are presented as means with standard deviations (SDs) or percentages (%). Categorical data were compared using the chi-squared test. The Wilcoxon and Mann–Whitney U tests were utilized for comparing non-parametric variables, while independent- and paired-samples t-tests were used for parametric variables. P < .05 was considered statistically significant.
Results
Demographic Data
This study included 103 patients (103 ears). In total, 11 of 52 patients (21.2%) in the PCBI group and 13 of 51 (25.5%) in the PCOU group were lost to follow-up; the difference was not significant (P = .773). The final analysis included 41 of the 52 patients (78.9%) in the PCBI group and 38 of the 51 patients (74.5%) in the PCOU group (Figure 3). Age, sex, duration of condition, ear side, presence of myringosclerosis, and smoking status were matched between the two groups (Table 1). The mean operation time was significantly shorter in the PCBI group (31.2 ± 1.9 min) compared to the PCOU group (52.8 ± 6.3 min, P < .001).
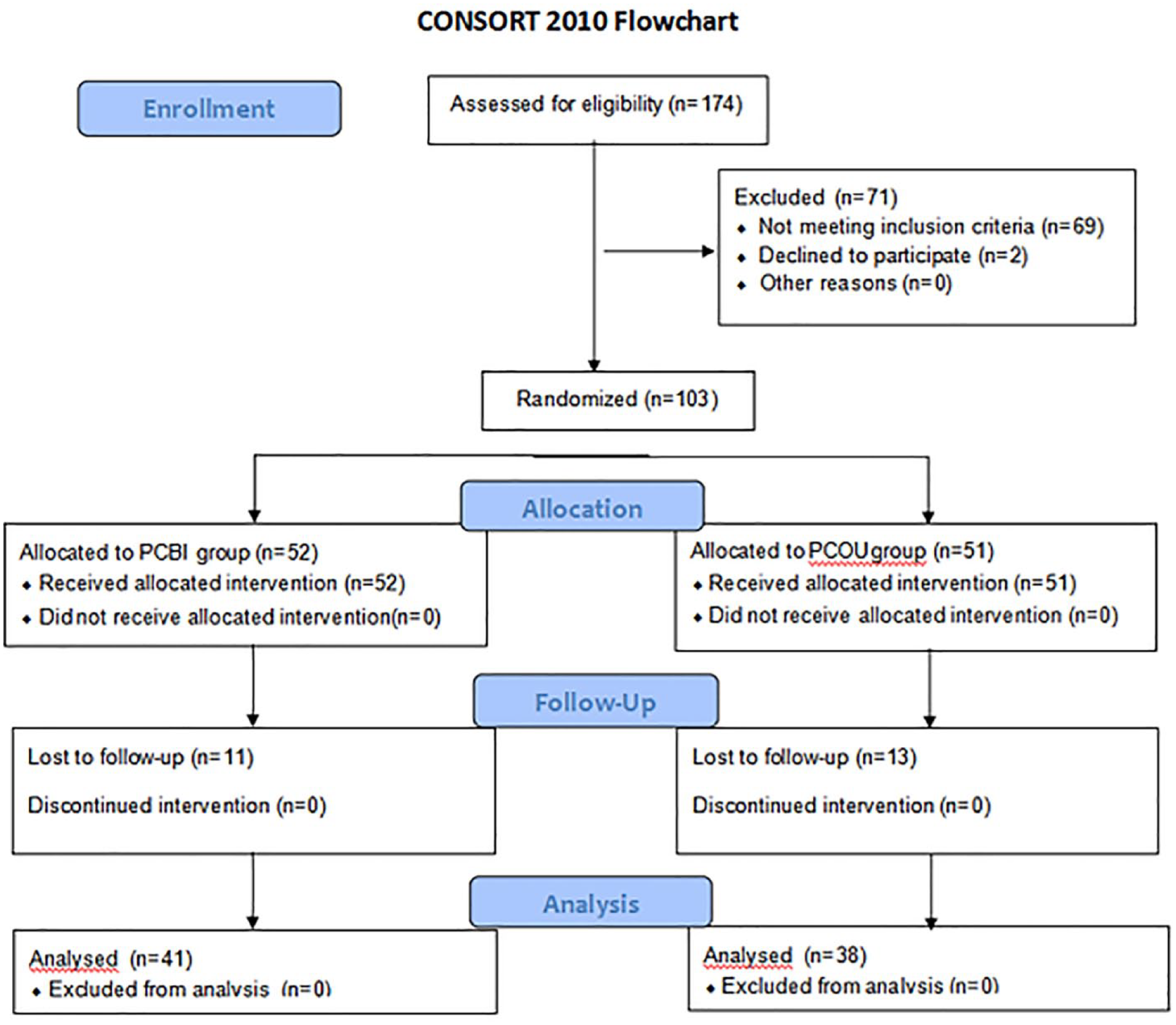
Enrollment, randomization, and follow-up of study participants.
Demographic Characteristic of Patients.
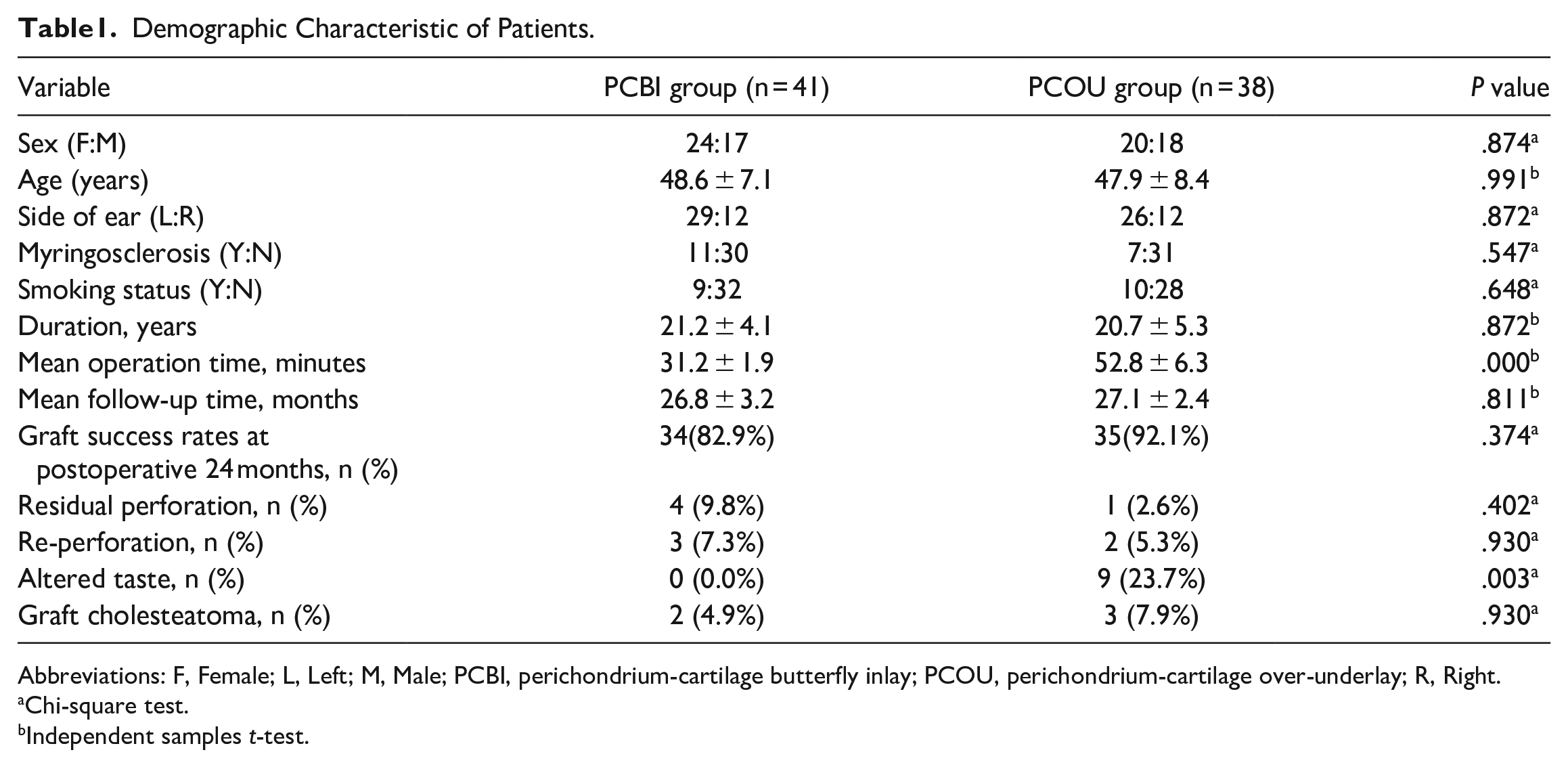
Abbreviations: F, Female; L, Left; M, Male; PCBI, perichondrium-cartilage butterfly inlay; PCOU, perichondrium-cartilage over-underlay; R, Right.
Chi-square test.
Independent samples t-test.
Graft Success Rate
At 24 months postoperatively, residual perforation was observed in four patients (9.8%) in the PCBI group and one patient (2.6%) in the PCOU group; the difference was not significant (P = .402). Similarly, there was no significant difference in reperforation rate between the PCBI and PCOU groups (7.3% vs. 5.3%, P = .930). The graft success rate was 82.9% (34 patients) in the PCBI group and 92.1% (35 patients) in the PCOU group, and the difference was not significant (P = .374).
Hearing Outcome
Postoperative ABG showed significant improvement compared to preoperative ABG in both groups(Table 2). However, no significant difference was observed between the groups in either the preoperative (P = .941) or postoperative (P = .893) ABG, or in the mean ABG gain (P = .759). Additionally, there was no significant difference between the groups in the preoperative (P = .672) or postoperative (P = .664) mean BC PTA.
Comparison of Hearing Gains, the Air-bone Gap, and Bone Conduction.
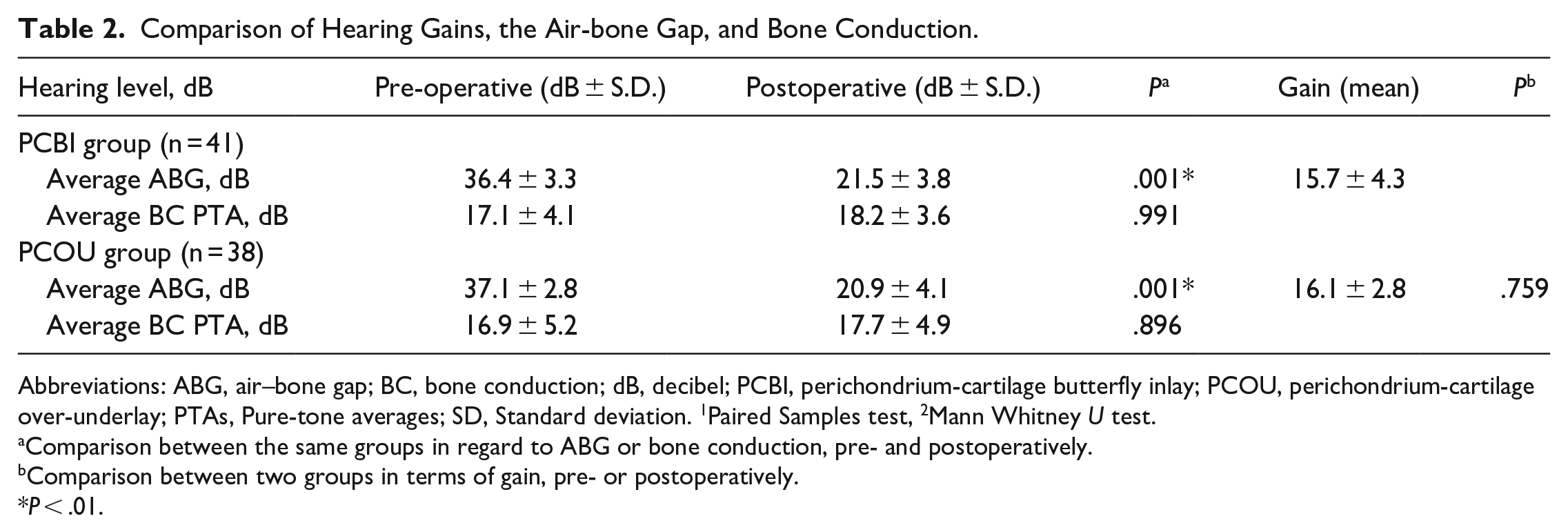
Abbreviations: ABG, air–bone gap; BC, bone conduction; dB, decibel; PCBI, perichondrium-cartilage butterfly inlay; PCOU, perichondrium-cartilage over-underlay; PTAs, Pure-tone averages; SD, Standard deviation. 1Paired Samples test, 2Mann Whitney U test.
Comparison between the same groups in regard to ABG or bone conduction, pre- and postoperatively.
Comparison between two groups in terms of gain, pre- or postoperatively.
P < .01.
Complications
The mean follow-up time was 26.8 ± 3.2 months (range: 26–31 months) in the PCBI group and 27.1 ± 2.4 months (range: 25–32 months) in the PCOU group (P = .811). HRCT showed good pneumatization of the mastoid and middle ear in both groups.
Altered taste occurred in no patients in the PCBI group and in nine (23.7%) patients in the PCOU group; the difference was significant (P < .05). Graft cholesteatoma was found in two (4.9%) patients in the PCBI group and three (7.9%) in the PCOU group; the difference was not significant (P = .930). In the PCBI group, the graft cholesteatoma locations were the anterosuperior and anteroinferior TM in one patient each; in the PCOU group, graft cholesteatoma was near the malleus handle in two patients and in the EAC flap in one patient. All graft cholesteatomas were removed endoscopically in the office.
No graft-related complications, such as graft lateralization, significant blunting, or graft medialization, were reported during the follow-up period. None of the patients experienced sensorineural hearing loss or intractable tinnitus.
Discussion
The cartilage butterfly technique has been successfully utilized to repair chronic perforations, yielding satisfactory outcomes. Its main advantages include avoiding the need to elevate the tympanomeatal flap, use packing, or remove myringosclerotic plaques.3,5 However, the technique faces two primary challenges: accurate evaluation of the perforation size and meticulous preparation of a precisely fitting cartilage graft.6,8 The tragal cartilage, which is quite thin (average thickness of 1.18 ± 0.11 mm in males and 1.12 ± 0.14 mm in females), 12 makes the procedure particularly difficult for beginners and requires the assistance of a microscope. Additionally, the butterfly technique is not suitable for thin, atrophic, or scarred TMs.
Building on the principles of the butterfly technique and ventilation tube insertion, we introduced the extended PCBI technique. In this technique, the perichondrium is circumferentially elevated while maintaining its attachment to the cartilage, forming a circular gap between the perichondrium and the cartilage. This gap is similar to the circular groove in the butterfly technique and grasps the perforation margins. Raising the perichondral flap is easier than creating a circular groove in the cartilage, especially for thin cartilage, and does not require microscopic assistance. Furthermore, in the traditional butterfly technique, the atrophic TM remnant is often torn by the cartilage graft, potentially enlarging the perforation in atrophic or scarred TMs and causing the graft to fall into the tympanic cavity. In contrast, our extended perichondrium-cartilage technique mainly relies on support from the handle of the malleus and sclerotic plaque. The PCOU technique, requiring elevation of a tympanomeatal flap and the creation of a tunnel, not only increases the operation time but can also lead to increased intraoperative bleeding, indirectly prolonging the operation. The extended perichondrium-cartilage butterfly technique, however, does not involve these steps. Our study indicates that the extended perichondrium-cartilage butterfly technique significantly reduces the mean operation time compared to the over-underlay technique, which involves the raising of a tympanomeatal flap (31.2 ± 1.9 vs 52.8 ± 6.3 min, P < .001).
In this study, the graft success rate at 24 months postoperatively was not significantly different between the PCBI and PCOU groups (82.9% vs 92.1%, P = .374). There was also no significant group difference in the rate of residual perforations (9.8% vs 2.6%, P = .402) or re-perforations (7.3% vs 5.3%, P = .930). These graft success rates are comparable to those reported in the literature for cartilage butterfly and over-underlay techniques, which are in the range of 43–100%.10,13,14 Alain et al 5 reported a 92% success rate at 6 months postoperatively using butterfly myringoplasty for subtotal perforations, while Demir et al 7 and Jumaily et al 14 reported success rates of 96% and 65.6%, respectively, for large- and medium-sized perforations. Zhang et al 13 and Bao et al 15 reported success rates of 89.80% and 95.0%, respectively, using the over-underlay technique for large perforations. The external perichondrium in our study likely aided migration of the epithelium of the TM remnant, in turn accelerating epithelization of the cartilage graft and facilitating its survival, similar to the patch technique used for traumatic perforations.
The audiologic gains observed were similar to those documented in the literature,4-15 with no significant differences noted in pre- or post-operative ABG values or mean ABG gain. Theoretically, the superficial layer of the TM might migrate below the edges of the cartilage graft in the butterfly technique, posing a risk of cholesteatoma formation. However, no cases of middle ear cholesteatoma have been reported in the English-language literature.3-9 In our study, 79 patients were followed up for 24 months and underwent HRCT at the final follow-up, with well-pneumatized mastoids and middle ears being observed in both groups. Cholesteatoma may develop under the perichondrium in the TM epithelium with our technique. The cartilage overlaps the TM remnant epithelium by at least 1–2 mm when using the butterfly technique; similarly, the perichondrium graft overlaps by at least 2–3 mm. We believe that positioning the cartilage graft medial to the TM remnant can prevent epithelial migration into the middle ear, thus avoiding cholesteatoma when using both the traditional butterfly technique and our extended technique. Since the epithelial layer of the TM remnant is preserved in both techniques, the likelihood of cholesteatoma developing is not substantially different. Kim et al 16 also reported no cases of cholesteatoma when using a butterfly dermal allograft technique. Moreover, graft cholesteatomas occurred in 4.9% of patients in our PCBI group and in 7.9% in the PCOU group (P = .930), suggesting that it may be unrelated to the graft material or technique. Nejadkazem et al 17 and Ayache et al 18 reported graft cholesteatoma rates for the underlay technique, whereas Babu et al 19 and Bao et al 15 reported rates for the over-underlay technique. In our technique, the perichondrium does not completely cover the TM remnant or the annulus, which may allow the epithelium to shed without entrapment, thereby avoiding the risk of entrapment. Thus, this technique could be an alternative to the endoscopic butterfly technique, especially in cases with thin cartilage, atrophic TMs, or scarred TMs.
No patients in this study reported altered taste following PCBI, whereas 23.7% reported altered taste following PCOU. This finding aligns with previous studies suggesting that raising the tympanomeatal flap increases the risk of damage to the CTN, leading to temporary taste alteration.1,2,13 Iynen et al 20 reported CTN damage-related symptoms in 16.6% of patients during tympanoplasty, whereas Sham et al 21 noted a prevalence rate of ~50% for CTN injury following myringoplasty. Limitations of this study included its single-institution design and small sample size. Additionally, the 2-year follow-up period means that the development of middle ear cholesteatoma, which may occur ≥3 years after surgery, cannot be ruled out.
Conclusion
The endoscopic extended PCBI technique is a safe and effective method for repairing subtotal perforation. It does not require the raising of a tympanomeatal flap and is associated with high long-term graft success rates and minimal complications.
Footnotes
Author’s Note
Author Contributions
Data Availability Statement
All data generated or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study protocol, approved by the Human Research Ethics Committee of Wenzhou Medical University Affiliated Yiwu Hospital, adhered to local and national laws, and the World Medical Association Declaration of Helsinki. Written informed consent was obtained from all patients, including consent from parents or guardians for minors. All procedures were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Not applicable.