
Abstract
Introduction
The standard treatment of chronic tympanic membrane (TM) perforation is myringoplasty, but the gold standard remains an inpatient tympanoplasty under general anesthesia. 1,2 This result in high medical costs and potentially associated risk. 1 -3 Some scholars suggested office-based myringoplasty to reduce the medical costs and shorten the surgical wait times. 3 Office-based myringoplasty is defined as a transcanal procedure performed without sedation or general anesthesia and without creating a tympanomeatal flap. 2,4 Some authors performed hyaluronic acid application and 2 platelet-rich plasma myringoplasty 5 to use office-based surgery and obtain good results; however, these biological materials are expensive, not readily available, and only restricted to small perforations in an office setting. 2,5
Inlay butterfly cartilage myringoplasty was described by Eavey, 6 which is to insert the cartilage graft into the perforation edges of the TM by creating circumferential grooves on the graft and achieve graft stabilization, thereby making it incorporate into the TM remant. It does not require tympanomeatal flap elevation and packing of external auditory canal (EAC). 6 Theoretically, it is consistent with office-based surgery. However, butterfly cartilage myringoplasty is relatively difficult to accurately creat circumferential grooves on the cartilage graft of 0.5 to 1 mm depth to fit the size and shape of perforation. 7 In addition, relatively speaking, the cartilage is heavy on the TM, especially for the atrophic TM around the edges, which inlays into the thin TM margins and easily causes a laceration or slides out of TM, thereby losing one’s balance and resulting in residual perforation. Özdemir et al 8 presented a new technique of extended perichondrium butterfly; its advantage is that it only requires the reservation of perichondrium but still requires creating the grooves of the cartilage. Recently, we developed a new office-based perichondrium-cartilage butterfly technique without creating the grooves of the cartilage but only elevating the lateral perichondrium. In this article, we describe our study of the effectiveness of a new perichondrium-cartilage butterfly technique in repairing chronic TM perforations as an office-based procedure.
Material and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Yiwu Central Hospital (Grant #2021KY1186). Informed consent was obtained from all participants.
Methods
This was a prospective case series study performed between June 2016 and June 2020. The inclusion criteria were as follows: aged more than 18 years; chronic perforation associated with mucosal chronic otitis media; at least 2 mm of remnant TM around the margin but does not involve the malleus; dry ear for at least 3 months prior to surgery, and good middle-ear pressure-regulation functions. Suspected ossicular chain disruption, cholesteatoma, middle-ear inflammation, myringitis, and revision cases were excluded from the study. All patients who underwent this procedure (as per the inclusion criteria) over this time period were included in the study. However, some patients who fitted the inclusion criteria did not undergo surgery with this technique but another technique was used in hospital. Nevertheless, a control or comparison group was not included in this study.
The middle-ear pressure-regulation functions including active eustachian tube (ET) functions and transmucosal gas exchange function were preliminarily evaluated to exclude the mechanically obstructed ETs. 9 The mastoid condition was examined on the computed tomography (CT) before surgery and revealed the good air space. Each participant was asked to perform a Valsalva maneuver, and they noted that they were able to “pop” or “clear” their ears, indicating a positive maneuver. 10 The perforation size was classified as small (1/8-1/4 of the pars tensa area) and medium (1/4-1/2 of the pars tensa area). The location of the TM perforations were classified as anterosuperior quadrant (ASQ), anteroinferior quadrant (AIQ), posterosuperior quadrant (PSQ), and posteroinferior quadrant (PIQ).
The audiometry was performed by an independent audiologist. Audiometric data were obtained preoperatively and 6 months postoperatively. Pure-tone averages (PTAs) were calculated for both air conduction (AC) and bone conduction (BC) by averaging the thresholds at 500, 1000, 2000, and 3000 Hz; in most cases, a threshold of 4000 Hz was used to interpolate the threshold of 3000 Hz as per the standards of the Hearing Committee of the American Academy of Otolaryngology—Head and Neck Surgery. 11 Pre- and postoperative ABG was calculated by subtracting the AC PTA from the BC PTA. ABG closure was calculated as preoperative ABG minus postoperative ABG. The operative time was defined as the duration from the perichondrium-cartilage graft harvest to the successful graft placement. Intraoperative pain intensity was measured via a visual analog scale. Intraoperative pain was rated on a subjective scale with scores ranging from 1 (no pain) to 10 (severe pain). 12
Surgical Technique
All patients underwent perichondrium-cartilage butterfly inlay myringoplasty by a single surgeon in an outpatient-based surgery. Patients were placed in a supine position with their head turned so that the ear with the perforation was up. A 0° endoscope with 4-mm diameter and 18 cm was used during the operation and a high-definition monitor. The patient’s ear was prepped with Betadine, the periaural area and the ear canal is injected with 2 mL of 2% lidocaine with 1:100,000 epinephrine. Transcanal injections (1 cc) were administered in all 4 quadrants by using a 20-gauge needle under direct endoscopic vision. Meanwhile, blanching of the canal skin was observed, and hemorrhagic bulbs were prevented by slowly and carefully injecting local anesthesia. The EAC and surface of TM were packed using a small piece of gauze soaked with 2% lidocaine with 1:100,000 epinephrine for 10 minutes to ensure the blanching of TM.
A tragal cartilage with single-side perichondrium is harvested from the ipsilateral tragus. The lateral perichondrium was circumferentially elevated but the pedicle attached the cartilage graft to created a circumferential “clip” between the perichondrium and cartilage. The cartilage is fashioned to make it 0.5 to 1 mm larger than the freshed margins, while the lateral perichondrium graft is also trimmed to make it 1 to 2 mm wider than the cartilage.
The perforation margins and the mucosa underneath will be gently curetted to form minor bleeding. The myringosclerosis of TM remnant was reserved.
The tympanic cavity was slightly filled using a few biodegradable synthetic polyurethane foam through the perforation. The cartilage graft is placed trans-perforationally medial to the TM remnant, the lateral perichondrium is placed on the superficial layer of the TM around the perforation edges. The packing of EAC was not performed. The cartilaginous of EAC was packed with erythromycin ointment gauze, up to the tragus incision (Figure 1).
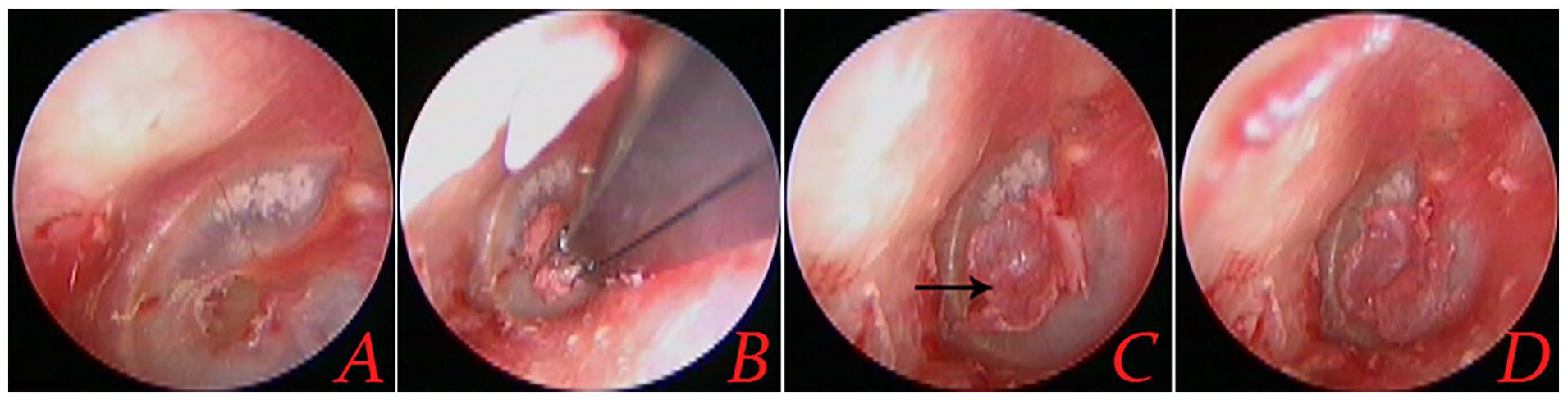
Surgical procedure of the same patient. The scoraping of perforation edges and mucosal underneath (A), the transcanal placement of perichondrium-cartilage graft (B), the free perichondrium lateral to the superficial layer (C and D).
Postoperative Follow-up
All patients received a course of antibiotics (amoxicillin) after the surgery. All patients were discharged on the day after the surgery. All patients were scheduled by endoscope for regular follow-up visits at 2 and 4 weeks postoperatively, as well as at 3 and 6 months postoperatively. Audiological testing was performed 6 months after surgery. At each follow-up time point, the patients were asked about altered taste, vertigo, and tinnitus, and some complications were observed, including facial nerve function, otitis media effusion, inclusions, and so on. Graft success was defined as the presence of an intact graft; graft failure was defined as the presence of a residual or re-perforation after surgery. Functional success was defined as an ABG ≤ 20 dB.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics, version 20 (IBM Corp, Armonk, NY, USA). Data are expressed as means (standard deviations) and numbers (percentages). Differences between preoperative and postoperative ABGs were analyzed using the Paired-Samples T Test. Differences with P < .05 were considered statistically significant.
Results
Demographic Data
A total of 39 patients (39 ears) were included in this study. Of the 39 patients, 28 (%) were female and 11 (%) were male (mean age at surgery, 42.6 ± 6.1 years; range, 38-57 years), the duration of perforations was 19.7 ± 3.9 years. Left perforation was in 22 (56.4%) patients and right in 17 (43.6%), 25(64.1%) ears were small perforation and medium perforation in 14 (35.9%) ears. The perforation location was in 6 (15.4%) patients in ASQ, 16 (41.0%) in AIQ, 13 (33.3%) in PSQ, and 4 (10.3%) in PIQ.
The mean operation time was 26.5 ± 3.2 (ranged from 21 to 32) minutes. The intraoperative mean pain score was 0.61 ± 0.28.
Graft Successs Rate and Hearing Outcome
All patients completed 6 months of follow-up. Residual perforation was seen in the posterosuperior margin in 1 patient, the graft success rate was 97.4% (38/39) at 6 months postoperatively. Audiological testing was achieved in 38 patients at 6 months postoperatively, which showed that there is no sensorineural threshold shift. The mean preoperative ABG was 19.18 ± 4.01 dB, while the mean postoperative ABG at 6 months was 10.56 ± 2.27 dB; the difference between these values was significant (P < .05; Paired-Samples T Test), a plot of the pre- versus postoperative audiometric (ABG) results are shown in the Figure 2. The functional success rate was 100.0% (38/38).
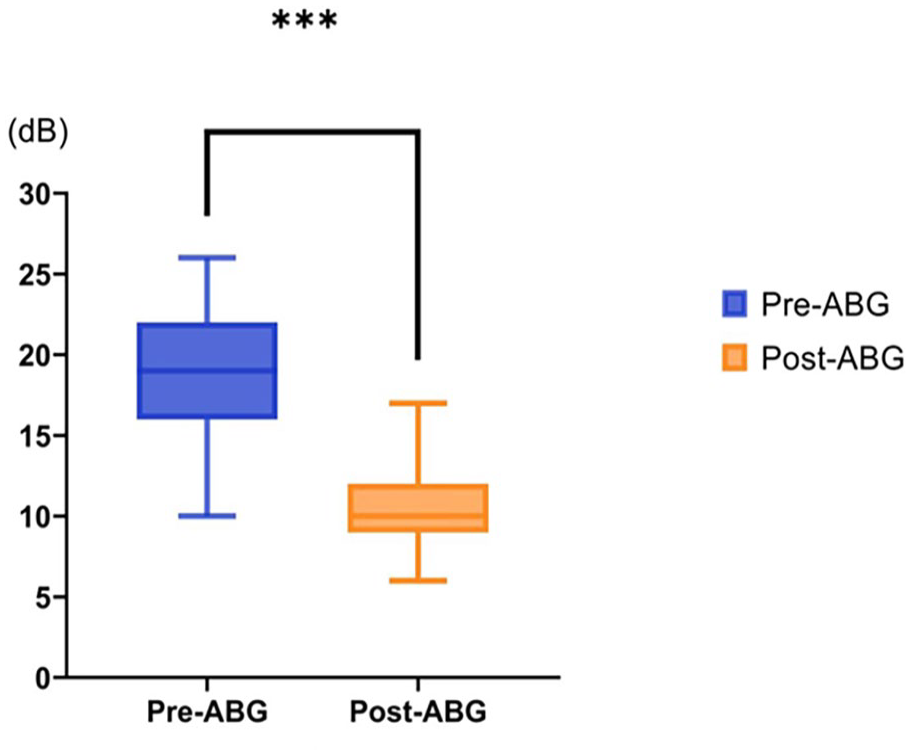
A plot of the pre- versus postoperative audiometric (ABG) results. ABG, air-bone gap.
Complications
Endoscopic examination showed that the transplanted perichondrium graft gradually atrophied, flattened, and became indistinguishable from the surrounding TM, 2 to 3 months following surgery, the superficial layer of perichondrium graft formed the crust and migrated into the EACat 3 to 6 months postoperatively (Figure 3). No graft-related complications (eg, graft lateralization, significant blunting, graft medialization) were encountered during the follow-up period. None of the patients reported sensorineural hearing loss, facial nerve palsy, vertigo, or intractable tinnitus. All the patients did not develop postoperative otitis media effusion. However, granular myringitis with minimal moistness but without infection has been noted in 10.3% (4/38) of patients.
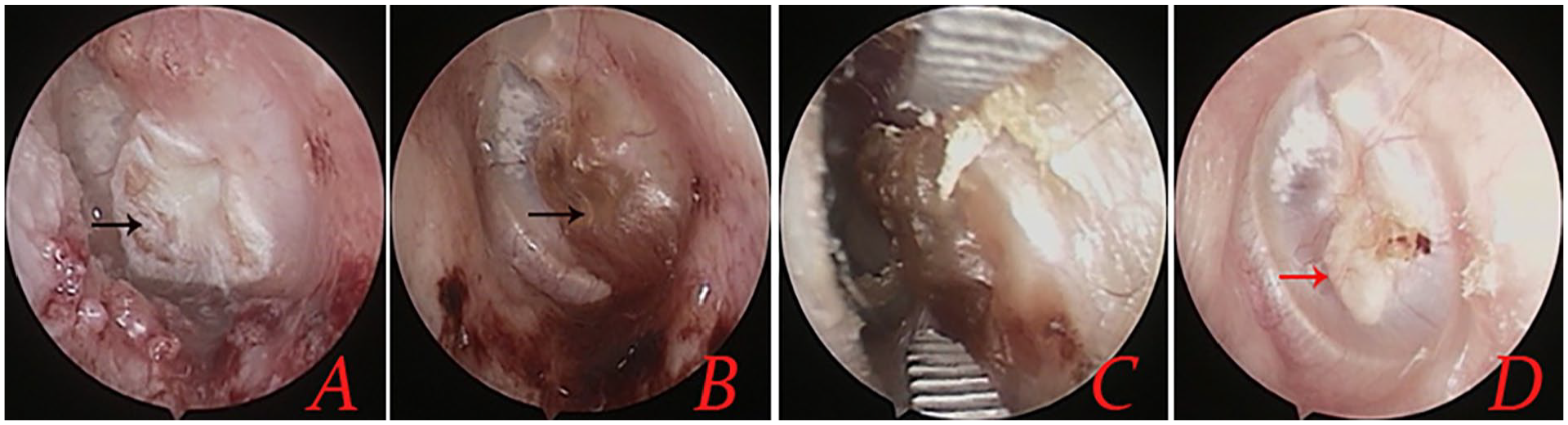
Follow-up of the same patient. Postoperative 2 weeks (A), 4 weeks (B), 3 months (C), and 6 months (D). Red indicated cartilage and Black indicated perichondrium.
Discussion
The office-based myringoplasty was defined as a transcanal procedure performed without sedation or general anesthesia and without creating a tympanomeatal flap. 2,4 Traditionally, indications for in-office myringoplasty have been limited to small and dry perforations, the margins of which are fully visible under microscopic examination. 4 Endoscopy improves visualization of the rim of the TM, thus expanding the indications for some medium-sized perforations, the margins of which are not fully visible under microscopic technique. In addition, a relative contraindication to in-office repair is the presence of extensive myringosclerosis. 3,4
Our technique is consistent with office-based surgery based on the definition. In this study, however, office-based surgery was also used to repair chronic medium perforation as long as it did not involve the malleus and elevation of the tympanomeatal flap.
In this study, the graft success rate reached 97.4% at 6 months after surgery, postoperative ABG had significant improvement compared with preoperative. This technique was similar to but not identical to inlay butterfly cartilage myringoplasty. Butterfly cartilage myringoplasty is to creat the grooves in the cartilage graft, which is diffcult for the beginner, 13 while only to elevate the perichondrium in the perichondrium-cartilage composite graft in this technique, which is relatively easy.
Monfared et al 1 reported the graft success rate of 67.6% using an office-based cartilage inlay myringoplasty. Özdemir et al 8 reported the graft success rate of 98.1% using extended perichondrium-cartilage butterfly technique, nevertheless, they did not significantly improved the procedure of cartilage butterfly technique but only preserved the single perichondrium. They believed that reservation of perichondrium facilitated the graft neovascularization and survival of cartilage graft. 8 Takahashi et al 9 previously reported that impairment of all the middle-ear pressure-regulation functions was likely to cause poor outcome of tympanoplasty, and ears with mechanically obstructed ETs were contraindicated for tympanoplasty. In this study, the middle-ear pressure-regulation functions were preliminarily evaluated by preoperative CT and Valsalva maneuver, the patients with poor mastoid air space and mechanically obstructed ETs were excluded.
Yuasa and Yuasa 14 applied autologous tissue using simple underlay myringoplasty with fibrin glue as office-based myringoplasty to repair small perforations and obtained the graft success rate of 97.3%, 14 the high success rate was due to the stable adhesion between the remnant TM and the graft by the fibrin glue. 14 In this study, middle-ear packing supports the cartilage graft, and the overlay perichondrium itself plays a role in glue sealing to ensure the stable adhesion between the remnant TM and perichondrium. In addition, some authors suggested the excision of myringosclerosis, 3,4 while any thick sclerotic plaques were reserved in this study. Lou et al 15,16 found that sclerotic plaques did not affect the graft neovascularization. Sclerotic plaques, remnant TM, and the malleus play a role of support for the perichondrium, thereby further ensuring the intimate contact between the remnant TM and the perichondrium. 17
In this study, the perforation edges and sclerotic plaques were not excised but only the mucosas underneath were curetted to form the vascular bed and prevent the expansion of perforation; these procedures may reduce the intraoperative pain. In this study, most of patients well tolerated the intraoperative pain, the intraoperative mean pain score was 0.61 ± 0.28. In addition, the vascular bed facilitated the graft healing. Supiyaphun and Kerekhanjanarong 18 reported only a partial removal of skin on the TM remnant followed by lateral placing of fascia and free skin graft and obtained the graft success rate of 97%. Lou et al 19,20 found similar graft neovascularization, epithelization, and graft success rate between excising and preserving perforation margins with myringoplasty.
Postoperatively, the ABG significantly improved because the perforations did not involve an ossicular chain abnormality; the function success rate reached 100%. Similar to previous study, 21 in this study, the transplanted perichondrium graft gradually atrophied, flattened, and became indistinguishable from the surrounding TM 2 to 3 months following surgery, the superficial layer of perichondrium graft formed the crust. 13,17,20 Gülşen and Erden 22 observed that the excess perichondrium became necrotic in a short period of time postoperatively. Thus, although this study did not perform the long-term follow-up, we speculated that iatrogenic cholesteatoma was almost minimum. This had been provened by previous studies, Lou et al 15,16 applied the double layer graft technique without removal of the superficial layer and did not find the iatrogenic cholesteatoma. In addition, all the patients did not develop postoperative otitis media effusion during the period of follow-up because the mechanically obstructed ETs were excluded in this study.
This method possesses some advantages: (1) the procedure does not require the removal of perforation edges and sclerotic plaques, most of patients well tolerated the procedure, only a few reported mild pain. In addition, only mucosas underneath of the perforation margins are curetted, thus a reoperation can be done easily even when a perforation recurs; (2) the technique is simple and shortens the operation time; (3) the procedure does not require hospitalization, thus the cost of surgery is inexpensive; (4) since no packing is necessary in the EAC, the results of graft are easily observed, and, if necessary a graft mismatch can be corrected in the early stage; (5) it does not require worrying about iatrogenic cholesteatoma, even if the epithelial pearl occured, they can be removed by endoscope in an office setting. 23 However, further large sample and long-term follow-up are needed in future.
Conclusion
Inlay butterfly perichondrium-cartilage myringoplasty is a highly successful and minimally invasive procedure well tolerated by adults for closure of small- and medium-sized perforations in an office setting.
Footnotes
Author Contributions
CZ: Interpretation of data for the work, design of the work, analysis of data for the work, drafting the work, and agreement to be accountable for all aspects of the work; final approval of the version to be published.
Data Availability Statements
All data generated or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Technology Agency of Jinhua city, China (Grant #2022-3-042).