
Abstract
Trigeminal neurofibromas are rarely reported, and even rarer when involving the infratemporal fossa. We describe the case of a 58-year-old man incidentally found through magnetic resonance imaging to have a tumor situated mainly in the infratemporal fossa. The tumor derived from the third branch of the trigeminal nerve and was totally removed by endoscopic endonasal surgery. Final pathology confirmed a diagnosis of neurofibroma. The patient had no intraoperative or postoperative complications except for numbness of the face. During the 6 years of follow-up, there has been no tumor progress or recurrence. We consider that endoscopic endonasal surgery is feasible in treating trigeminal neurofibromas involving the infratemporal fossa.
Introduction
Neurofibromas usually manifest as multiple benign tumors arising from peripheral nerves of neurofibromatosis type 1 (NF1), with nodules, café-au-lait spots, or speckles on the skin. Solitary neurofibromas are quite rare. 1 To our knowledge, there have been fewer than 50 reports of solitary trigeminal neurofibromas, which have mostly arisen from the distal nerve branches and located in the oral cavity.2-5 By contrast, trigeminal neurofibromas involving the infratemporal fossa (ITF) are rarer. Only 6 cases have been reported, and are more difficult to treat by surgery due to the deep location.6-11 Here, we report a case of trigeminal neurofibroma that arose from the trunk of the mandibular nerve, involving mainly the ITF. The tumor was successfully removed via endoscopic endonasal surgery, with acceptable complications.
Case Presentation
A 58-year-old man was admitted to the Otorhinolaryngology Department in Tianjin Medical University Second Hospital in December 2015. Ten days previously, during an examination for hypertension, a tumor was found incidentally. A cranial magnetic resonance imaging (MRI) scan located the tumor mainly in the ITF. The patient showed no neurological symptoms of hypoesthesia, paresthesia, or muscle weakness, nor did he have a family history of NF1. In addition, he was normally healthy without any systemic diseases except for hypertension.
The blood tests and otorhinolaryngologic examinations, including nasal endoscopy, otoscope, and pure tone audiometry, were normal. The MRI clearly showed the site of the tumor and its relationships with adjacent structures. In the T1-weighted MRI, the tumor was a slightly hypodense, heterogenous mass; in the T2-weighted MRI, it appeared slightly hyperdense and heterogenous. The gadolinium-enhanced image highlighted the tumor with a heterogeneously and markedly intensified shadow. The tumor was seen situated mainly in the ITF, while the oval foramen was obviously enlarged, indicating that the tumor origin was the third branch of the trigeminal nerve (Figure 1(A) and (B)). The internal carotid artery could be seen deviated, but without invasion (Figure 1(C)). MRI images before and after the surgery. (A, B) The tumor was situated mainly in the ITF and the oval foramen was seen enlarged (*tumor, → the enlarged oval foramen). (A) T1-weighted, coronal. The tumor was slightly hypointense, and heterogenous.(B) T2-weighted, axial. The tumor was heterogenously markedly enhanced with contrast medium. (C) The close anatomical relationship of the tumor and internal carotid (→). (D) There was no tumor residue or recurrence (*) twenty days after the operation.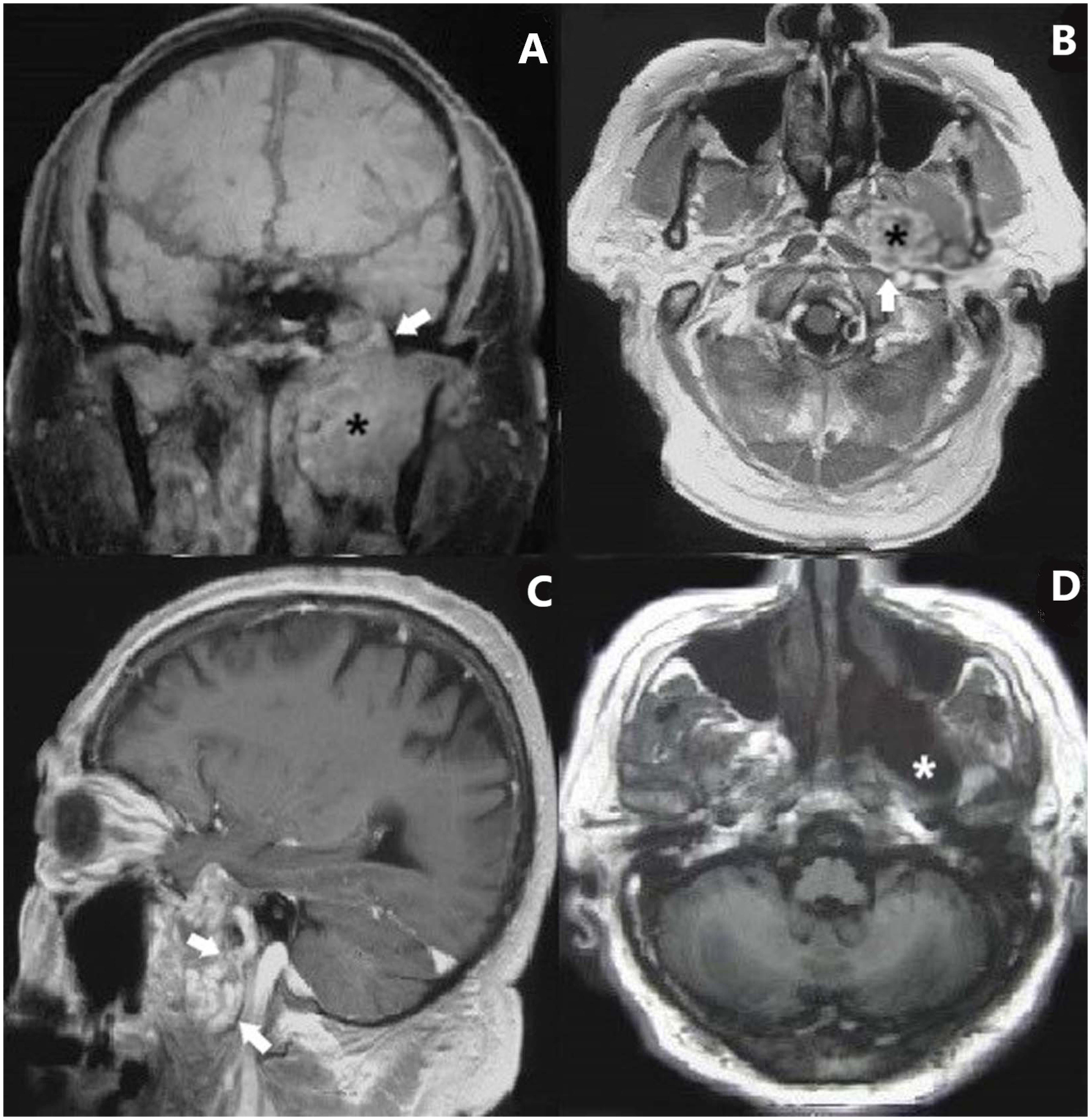
The patient provided written informed consent for surgical treatment. Endoscopic endonasal surgery was performed under general anesthesia to remove the tumor, as follows. First, the uncinate process was removed using low temperature plasma and ethmoid forceps. The opening of the maxillary sinus was enlarged and the sphenopalatine artery was coagulated to reduce bleeding. The bone of the medial part of the posterior wall of the maxillary sinus was removed by diamond drill and elevator. The fascia in front of the pterygopalatine fossa (PPF) was cut, and adipose tissue inside it was removed. Inside the PPF, the maxillary artery and its branches, as well as the nerves behind them, could be identified. The maxillary artery was cut off with sufficient coagulation, and the lateral pterygoid plate near it was drilled with a diamond drill until the tumor could be seen: it was a light gray, mixed mass with both cystic and fibrous contents (Figure 2(A) to (C)). Images show the main operative procedures and the postoperative pathology. (A) Cutting off the maxillary artery (→) in PPF to expose the lateral pterygoid plate (▲), ☆ shows the maxillary nerve. (B) Removing the lateral pterygoid plate (▲) with diamond drill.(C) The tumor appears as a light gray, cystic mass (*). (D) Attempting to remove the tumor (*) with endoscopic equipment. (E) Histologic section shows typical plexiform neurofibroma comprised of copious nerve fibers, fibroblasts, and collagen cells in mucinous matrix (Hematoxylin and eosin stain, 100×).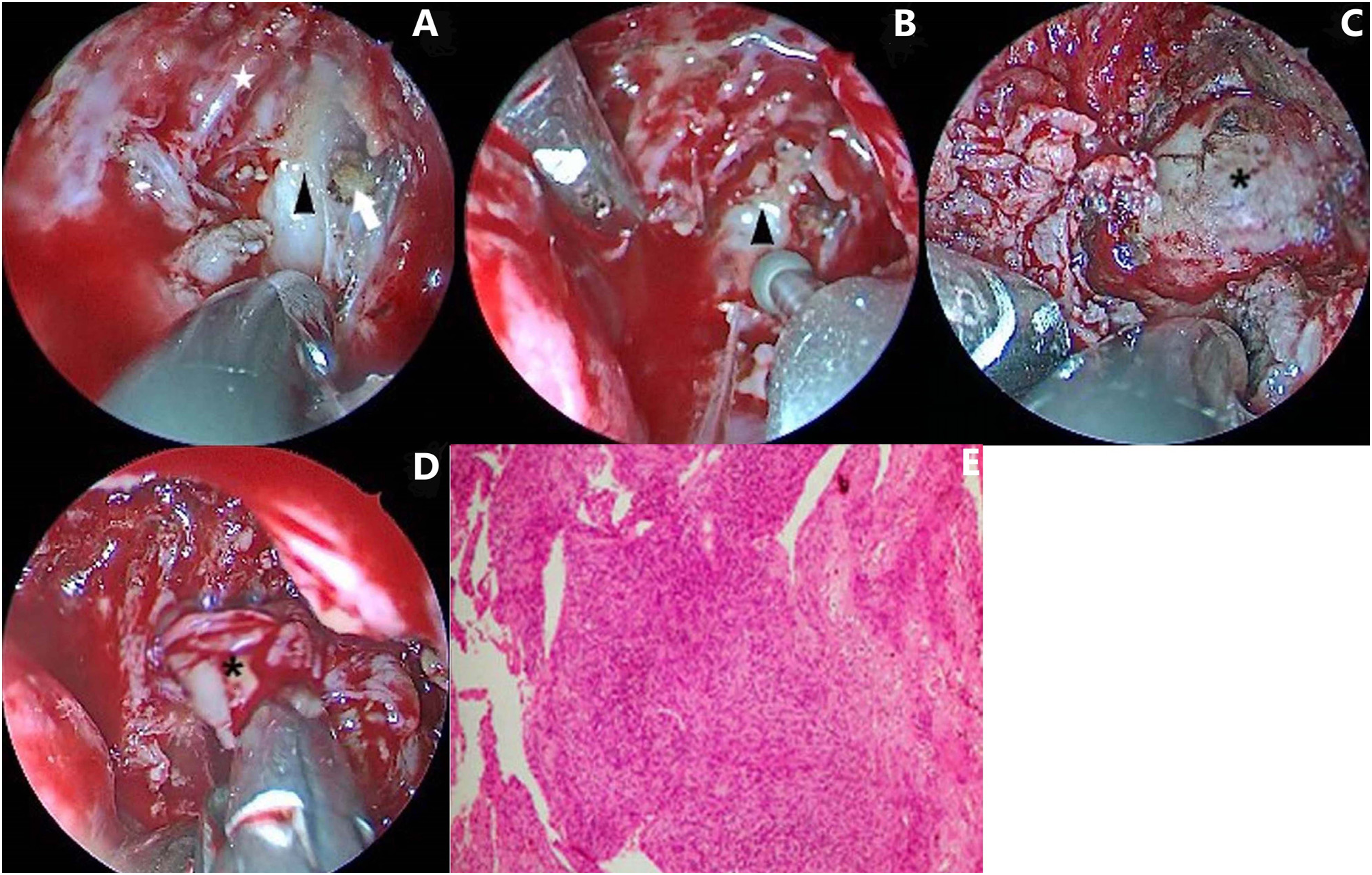
When trying to remove the tumor, we could see that it originated from the third branch of the trigeminal nerve. As much as possible, the tumor was removed while reserving nerve fibers that were not involved. Identification and preservation of the dura near the oval foramen and the internal carotid artery was particularly important, for fear of cerebrospinal fluid leakage or severe bleeding (Figure 2(D)). Finally, the ITF, PPF, and maxillary sinus were packed with gelatin sponge particles and iodoform sponges, and the tumor tissues were sent for pathological investigation.
The pathological result revealed plexiform neurofibroma (Figure 2(E)), and immunohistochemical staining was positive for S100. An MRI scan performed 20 days after surgery showed no tumor residue, indicating total excision of the tumor (Figure 1(D)). The patient suffered no complications except for numbness in his right face after surgery, which did not relieve with time. The most recent MRI scan was taken 4 years after surgery and no recurrence was detected. There has been no sign of tumor progression or recurrence as of this writing.
Discussion
We report here a case of solitary trigeminal neurofibroma that mainly involved the ITF. The tumor was totally resected via endoscopic endonasal surgery.
Solitary trigeminal neurofibromas are rarely encountered. To our best knowledge, there have only been 6 reports of trigeminal neurofibromas that involve the ITF, and only 3 of these were reported after the year 1990. Unlike schwannomas arising from nerve sheath cells, neurofibromas that arise from nerve fibers include involved nerve fibers and collagen fibers, as well as nerve sheath cells. 12 Therefore, neurofibromas can present with neurologic symptoms such as pain or paresthesia in the nerve distribution areas.
Yet, the present case showed no obvious neurologic symptoms. We believe this is because the tumor originated from the trunk of the mandibular nerve rather than its peripheral branches and was detected early enough on MRI that symptoms had not developed. He et al. 6 reported a pediatric case of trigeminal neurofibroma with a cheek mass and facial asymmetry, with no neurologic symptoms. As in the present case, the tumor originated from the trunk of the mandibular nerve. What is more, the present case did not show features of NF1 such as nodules, café-au-lait spot, or speckles on the skin, nor was there a family history of NF1, and thus a diagnosis of NF1 could be excluded.
The present case also suggests the importance of imaging for diagnosing trigeminal neurofibromas. Majoie et al. 13 reported that in T1 (T2) weighted MRI scans, trigeminal neurofibromas usually appeared isodense or hypodense (isodense or hyperdense). These features have been confirmed in trigeminal neurofibromas arising from the maxillary nerve, mandibular nerve, or their distal branches.7,8,14-16 In the present case, the tumor in the T1-weighted MRI was slightly hypodense, and in the T2-weighted, it was slightly hyperdense, which accords with the previous reports. In addition, in the present case obvious heterogeneity could be observed in the MRIs, both before and after intensified with contrast medium. This may be due to the variety of cells originating in the tumor. Boedeker et al. 15 also described this feature of heterogenous enhancement in MRI for trigeminal neurofibromas. We deduce that characteristics that might contribute to the diagnosis of trigeminal neurofibroma are: isodense or hypodense in T1-weighted MRI; isodense or hyperdense in T2-weighted MRI; and heterogeneity.
Given the potential for recurrence and malignant transformation in trigeminal neurofibroma, complete surgical resection is advisable and should be strongly considered.6,8 The present is the first reported case of trigeminal neurofibroma involving the ITF removed by endoscopic endonasal surgery. The ITF is deep within the head, surrounded by the maxillary bone, sphenoid bone, and mandible, and beneath the floor of the middle cranial fossa. Furthermore, the ITF contains important neurovascular structures including the mandibular nerve, chorda tympani, middle meningeal artery, internal maxillary artery and vein, pterygoid venous plexus, and pterygoid muscles. Thus, surgery for lesions in the ITF is challenging.
In recent decades endoscopic technology has developed rapidly. Theodosopoulos et al. 17 conducted a cadaveric study on endoscopic surgery for removing lesions in the ITF. Some researchers and surgeons subsequently proposed endoscopic endonasal surgeries for ITF tumors such as trigeminal schwannomas or meningiomas.18,19 However, until now there have been no reports on curing trigeminal neurofibroma via endoscopic endonasal surgery.
Lye et al. 11 described craniotomy for treating ITF trigeminal neurofibromas, and Loutfy et al. 9 applied surgery in two courses: first a temporal craniotomy and then by the preauricular pathway. In both reports, the tumors were successfully removed, but postoperative functional loss of the trigeminal nerve or mandible nerve occurred and the patients’ qualities of life were severely affected. Yue et al. 6 cured a pediatric case of trigeminal neurofibroma involving the ITF by transmandibular surgery, with no consequential neurologic complications. The transmandibular approach provided adequate exposure to the tumor. However, mandible osteotomy and reconstruction were necessary, causing comparatively large trauma, and the facial nerve was put at risk. Takuro et al. 7 proposed a transoral-retromolar combined with transtemporal approach for totally resecting a trigeminal neurofibroma in the ITF. The transoral-retromolar pathway succeeded in avoiding facial scarring, and reduced the risk of facial nerve injury. However, the transoral route led to a higher risk of infection. Besides, it should combine with the transtemporal route, which involved the middle cranial fossa, and thus injury of the intracranial nerves and blood vessels might occur. In the present case, we used endoscopic endonasal surgery and achieved total tumor resection without complications other than numbness in the mandible nerve distribution. The endoscopic surgery was minimally invasive, free of cosmetic problems due to the endonasal path, and craniotomy or mandible reconstruction was not needed. Compared with previous surgical approaches, the patient had a shorter hospitalization and suffered less during postoperative recovery.
In our surgery, we applied the endonasal-transpterygopalatine fossa approach to the ITF, as the tumor site was medial and anterior to the posterior wall of the maxillary sinus. This approach provided direct surgical access and enabled adequate exposure of the tumor. Also, compared with the lateral approach, dissection of the temporal and pterygoid muscles, and other structures within the ITF, was avoided. In the PPF, the maxillary artery was coagulated to prevent large bleeding, while the pterygopalatine ganglion and nerves connected to it were preserved.
The endoscopic surgery offered a good view, and operative manipulations could be done with a straight vision. The tumor in our case was extradural, but it had invaded the cranial basal bone and obviously pressed against the temporal lobe. Under the sight of the endoscope, the tumor was resected extradurally, largely decreasing the risk of cerebrospinal fluid leakage. Moreover, the tumor was close to the internal carotid, which could be seen clearly in the MRI. Thus, identification and protection of the internal carotid during the surgery was crucial, lest fatal bleeding occur. There was no intraoperative complication. Finally, the tumor in our case was obviously derived from the mandible nerve and was related to it. We took care to differentiate the involved nerve fibers from the non-involved, guaranteeing tumor radical resection to avoid tumor recurrence, while reducing unnecessary damage that can lead to complications. After the surgery, the patient suffered permanent numbness in the right face, which was most likely due to the tumor and was acceptable and inevitable.
Above all, we consider that the endoscopic endonasal approach is feasible for removing trigeminal neurofibromas in the ITF. Mastery of the anatomy of the PPF and ITF, with their inside and adjacent structures, combined with proficient endoscopic manipulation experience, can ensure the safety of the operation. Trigeminal neurofibromas may occur in any part of the trigeminal nerve path. More studies are warranted for indications of endoscopic endonasal surgery.
Conclusion
Solitary trigeminal neurofibromas involving the ITF are quite rare. Endoscopic endonasal surgery may be a good option for treating ITF trigeminal neurofibromas as it is minimally invasive, and total tumor resection can be achieved with acceptable complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Patient Consent
This study was approved by the Ethics Committee of Tianjin Medical University Second Hospital. All procedures involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The patient provided written informed consent for surgical treatment.
Data Availability Statements
The datasets generated and analyzed during the present study are available from the corresponding author on reasonable request.