
Abstract
Neuroendocrine tumors are rare and highly heterogeneous neoplasms with a wide spectrum of histological differentiation, functional, and biological features. Small cell neuroendocrine carcinomas (SNECs) of the sinonasal tract are particularly rare. Pathological features of SNECs of the nasal cavity and paranasal sinuses, which are aggressive tumors, are similar to those of anaplastic small cell carcinomas of the lung. We present a case of high-grade sinonasal SNECs in a patient with Xeroderma pigmentosum complementation group C (XPC) gene-positive xeroderma, which, to our knowledge, is the first case reported worldwide.
Introduction
Small cell neuroendocrine carcinoma (SCNEC) is characterized by poor differentiation, high-grade features, a mitotic rate of >20 mitosis per 2 mm2, and Ki-67 index exceeding 20%, which involves counting ≥500 cells in the areas with the highest labeling (hot-spots). 1 Neuroendocrine carcinomas are uncommon, exhibiting a wide spectrum of histological differentiation. 2 Neuroendocrine tumors (NET) are a spectrum of heterogeneous neoplasms with functional and biological features that vary based on location, tumor size, and histological differentiation. NET arises from the neuroendocrine cells. 3 Extrapulmonary sites of small cell cancer are rare. Extrapulmonary small cell carcinoma of the head and neck represent approximately 10% of all cases of extrapulmonary small cell cancer, and there are only a few reports of this disease. Small cell carcinomas in extrapulmonary locations typically have an aggressive natural course characterized by extensive metastases. 4 The gastroenteropancreatic system (approximately 70%) and the lungs (>25%) are the most common primary sites for NET due to the high density of neuroendocrine cells in these organs. 5 It is characterized by areas of high mitotic activity and necrosis. 6 Sporadic cases have been reported in the larynx and salivary glands in the head and neck. SNECs of the nasopharynx is extremely rare, with only 14 cases reported in the literature. 7 To our knowledge, this is the first reported case worldwide of high-grade sinonasal SCNEC in a patient with xeroderma pigmentosum complementation group C (XPC) gene-positive.
Case Report
A 15-year-old male has a known case of XPC-positive xeroderma pigmentosum, migraines, basal cell carcinoma, and osteochondroma. The patient’s complaints started 3 weeks before the surgery when he experiencing a progressive bifrontal pressure-like headache associated with blurry vision, particularly in the right eye. This condition deteriorated over time, and he also had recurrent episodes of nausea and vomiting. Over time, the patient developed redness in the right eye, proptosis, and recurrent mild epistaxis associated with nasal congestion, primarily on the left side. The patient denied experiencing any facial pressure, change of smell or taste, or any of the B symptoms. There was no known family history of malignancy. On examination, there was right eye proptosis, with redness and restricted eye movement. Nasal examination using a 0-degree scope showed inflamed mucosa on the right side with a fleshy mass occupying the right nasal cavity extending from the lateral wall up to the skull base and reaching down to the floor. Other ENT examinations, cranial nerves, and pulmonology examinations were unremarkable. A coronal view of computerized tomography (CT) scan of the brain and paranasal sinuses showed a large sinonasal tumor pushing the nasal septal to the other side with right intraorbital and intracranial extensions (Figure 1).
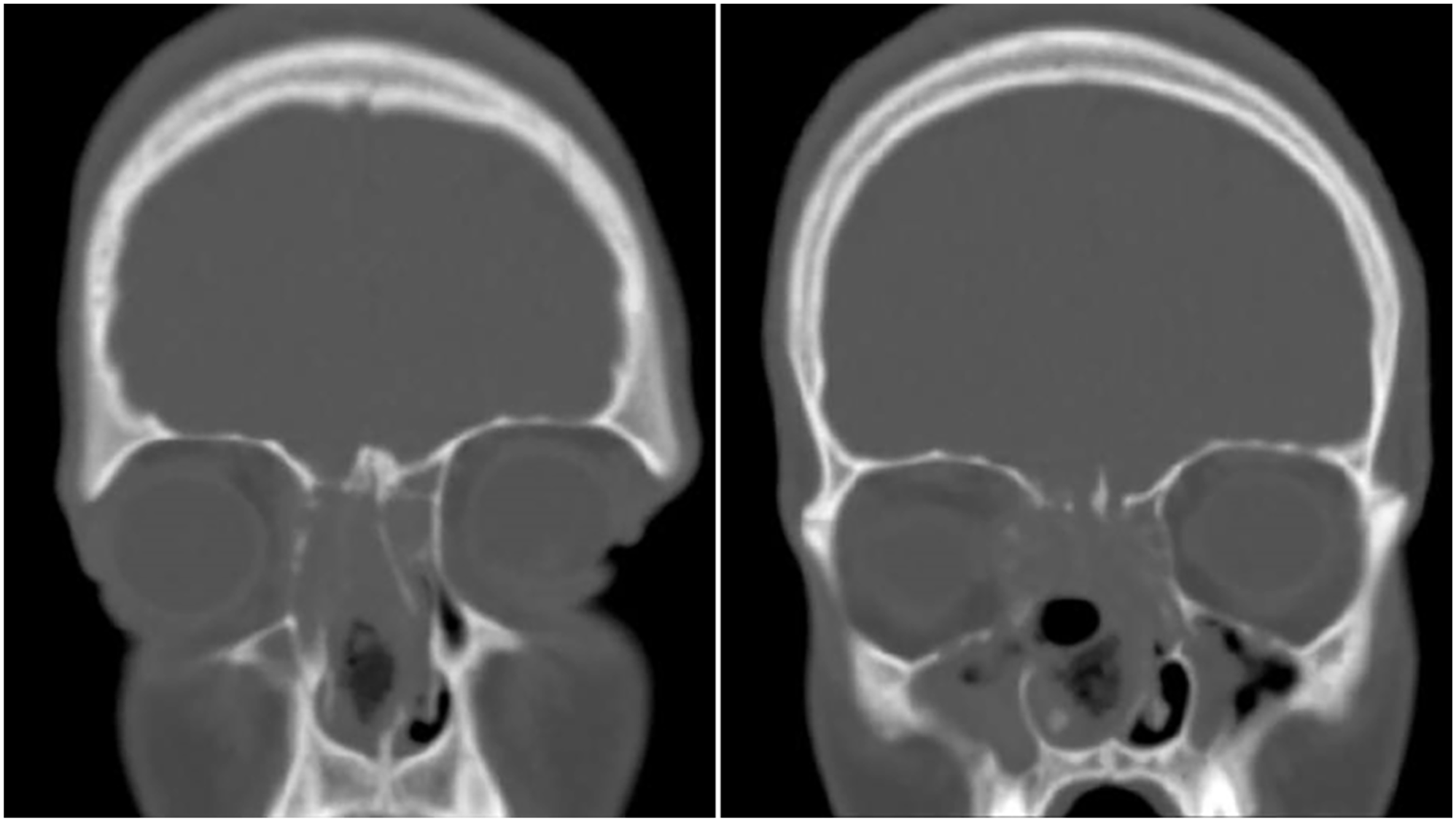
Coronal view of computerized tomography scan of the brain and paranasal sinuses with large sinonasal tumor.
Magnetic resonance (MR) imaging with a contrast of the sinus showed a large infiltrative soft tissue mass lesion occupying the anterior and posterior nasal cavity, ethmoidal air cells, and sphenoidal air sinuses extending to the right maxillary sinus. There was an associa-ted expansion of the aforementioned sinuses. In T1 with contrast, the imaging showed heterogeneous enhancement in post-contrast sequence, with the mass measuring approximately 7 cm × 4.7 cm × 4.6 cm in anteroposterior, crania-caudal, and transverse dimensions, respectively (Figure 2).
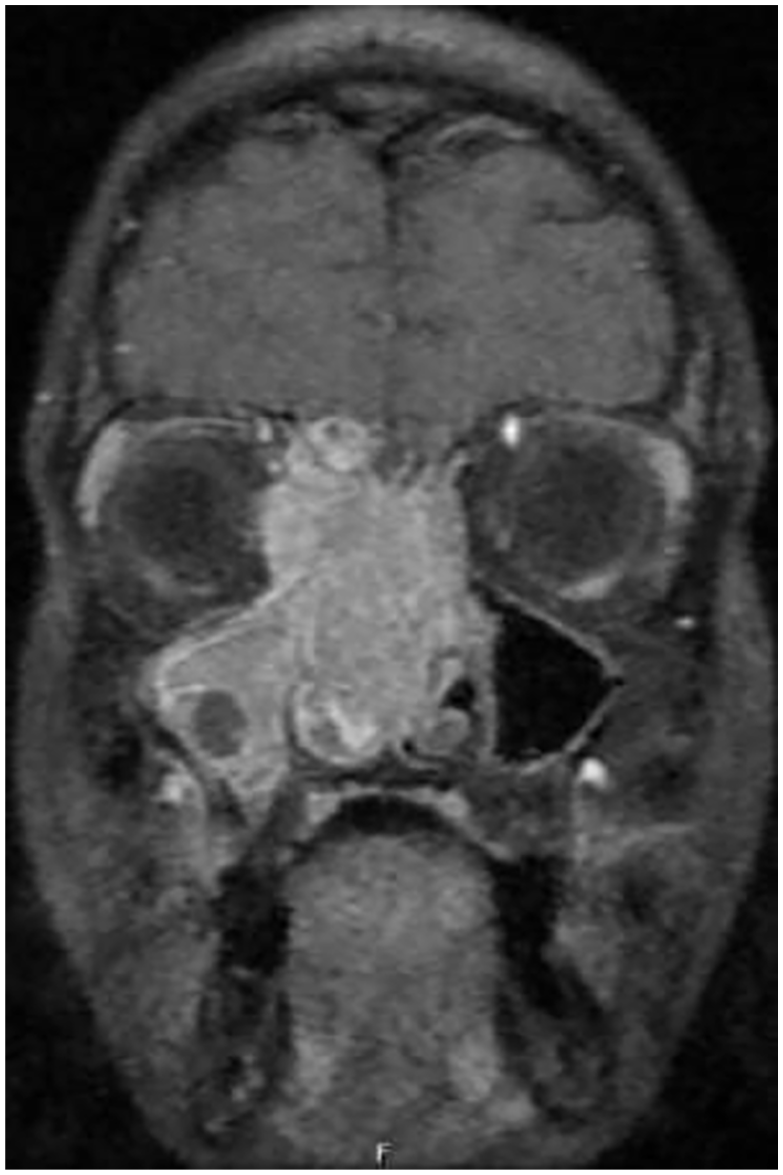
Magnetic resonance imaging with contrast of the sinus with large infiltrative soft tissue mass lesion occupying the anterior and posterior nasal cavity.
The patient underwent functional endoscopic sinus surgery. The surgical procedure included nasal mass debulking, right orbital decompression, biopsy, and surgical endoscopic sinus surgery. The intra-operative details were as follows. There was a right mucosal nasal mass filling the entire right nasal cavity all the way to the nasopharynx. The pathology report confirmed high-grade sinonasal SNECs in the right anterior ethmoid. Positron emission tomography scans revealed localized fluorodeoxyglucose (FDG) uptake suggestive of infectious/neoplastic processes within the ethmoid and sphenoid sinuses. No evidence of distant metastases was found (Figure 3). CT scan of the chest, abdomen, and pelvis revealed multiple nonspecific patchy ground glass opacities in the left lower lobe, which could potentially be associated with vaping/infectious processes. Furthermore, there was a nonspecific pulmonary nodule located in the lingular subpleural region, which was likely benign. No abdominopelvic metastases were found. The case was discussed in a tumor board meeting, which is a multidisciplinary gathering involving ear, nose, and throat surgeons, medical oncologist, radiation oncologist, and oral and maxillofacial doctors. Based on the discussion, the tumor was staged as T4N2M0. The multidisciplinary team agreed to treat the tumor with chemotherapy, with the possibility of adding radiation.
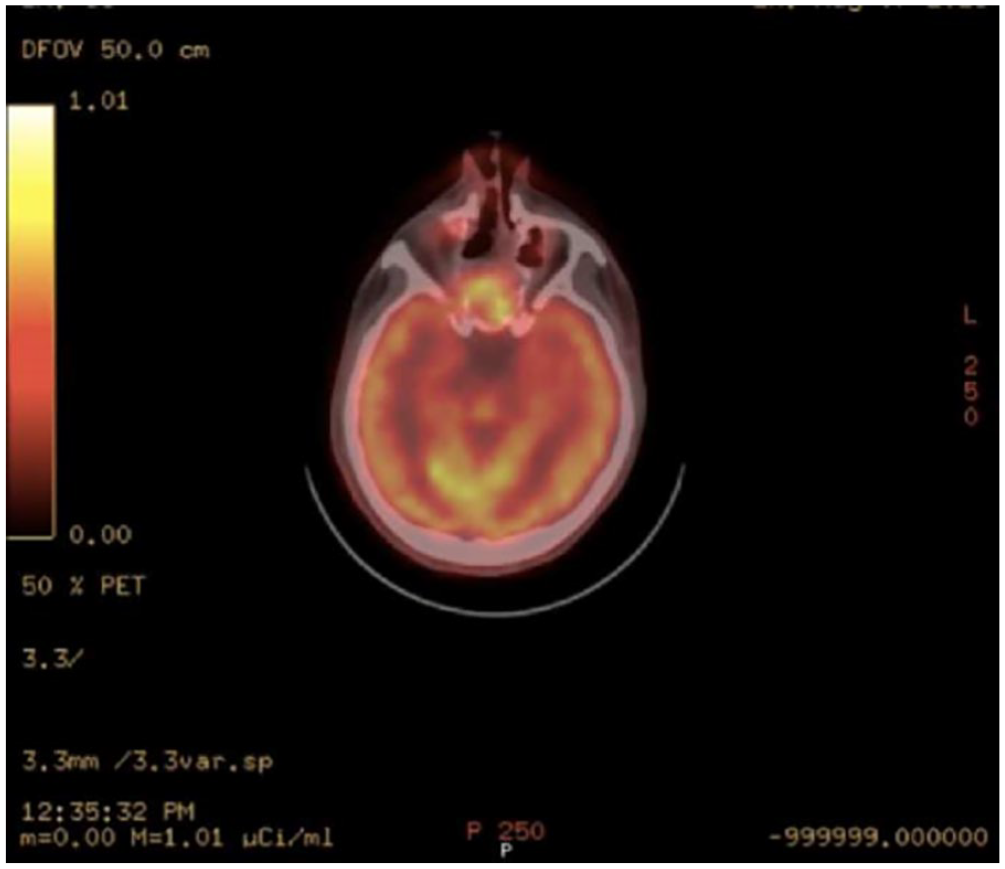
Positron emission tomography scan suggestive of infectious/neoplastic processes within the ethmoid and sphenoid sinuses.
Histopathology examination using different stains and markers showed benign surface-ciliated epithelium, with subepithelial neoplastic infiltration of small round cell tumor cells with high NC ratio, salt-and-pepper nuclear chromatin, and only a few small nucleoli. CAM5.2 cytokeratin stain displayed dot-like pattern in the tumor cells. There is a nonneoplastic gland serving as an internal control. CK 8/18 positive cytoplasmic staining.
Positive synaptophysin, Epithelial membrane antigen (EMA) and Thyroid transcription factor-1 (TTF1) immunostain. The Ki-67 proliferation index in tumor cells is almost 100% (Figure 4).
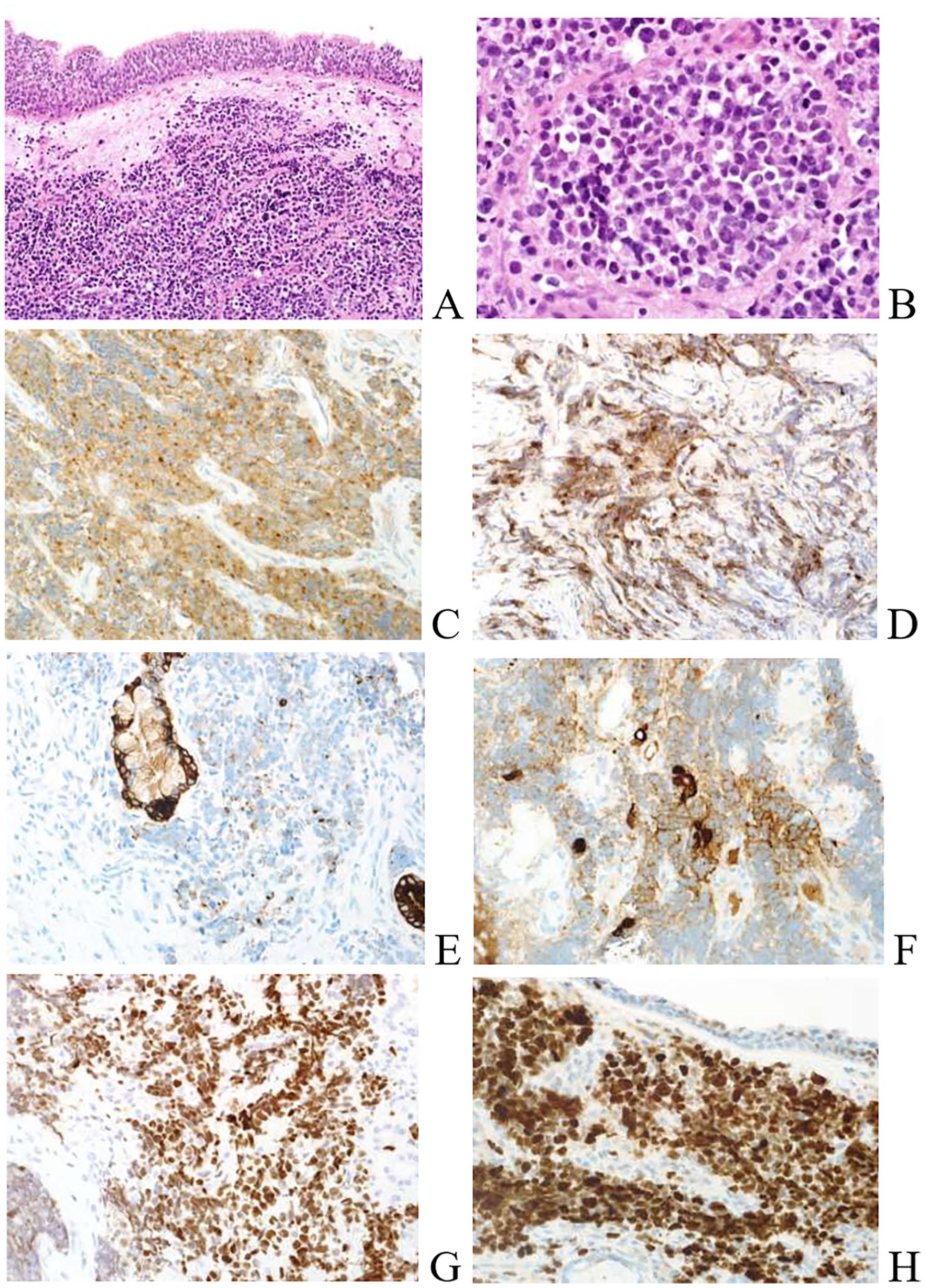
Stained section (A, ×20 and B, ×60) showed benign surface-ciliated epithelium, with subepithelial neoplastic infiltration of small round cell tumor and tumor cells with high NC ratio, salt-and-pepper nuclear chromatin, and only a few small nucleoli. Synaptophysin is strongly positive (C, ×40). EMA is strongly positive in tumor cells (D, ×40). CAM5.2 cytokeratin stain showed dot-like pattern in tumor cells, with nonneoplastic gland serving as an internal control (E, ×40). CK 8/18 positive cytoplasmic stainings (F, ×40). TTF1 immunostaining is strongly positive in tumor nuclei (G, ×40). Ki-67 proliferation index in tumor cells is almost 100% (H, ×40).
The tumor beneath the benign surface epithelium is a hypercellular small round cell tumor with no relation to the surface epithelium. It shows strong positivity for synaptophysin and CD56, weak positivity for chromogranin, and is positive for EMA. Additionally, it shows multifocal positivity for cytokeratin, including dot-like pattern, as shown above. TTF1 is strongly positive in tumor nuclei, and the Ki-67 proliferation index is almost 100%. P16 and calretinin were also positive, which raises consideration for the differential diagnosis of olfactory neuroblastoma. However, the presence of strong diffuse positivity for TTF1 and EMA, along with the dot-like pattern for low molecular weight cytokeratin and the absence of S100 positivity for sustentacular cell pattern, does not support the diagnosis of olfactory neuroblastoma. Other immunostainings for small round cell tumors such as desmin, myogenin, CD45, TDT, and CD99 are all negative.
Discussion
Neuroendocrine neoplasms (NENs) are tumors that can develop in many locations across the body. Based on their molecular distinctions, NENs are divided into NETs and neuroendocrine carcinomas (NECs). The classification of mixed NENs has evolved due to genomic data, and these tumors are now conceptually classified as “mixed neuroendocrine-non-neuroendocrine neoplasms (MiNENs).”
Mixed adenoneuroendocrine carcinomas, which exhibit genetic changes similar to adenocarcinomas or NECs than NETs, most likely represent clonal evolution within the tumors. 8 Xeroderma pigmentosum (XP) is a rare autosomal recessive disorder characterized by DNA nucleotide excisional repair failure following sun-induced damage from ultraviolet (UV) B light. 9 A high sensitivity to sunlight is among the symptoms of the disease, which leads to changes in skin pigmentation, sunburns, and a noticeably higher incidence of skin cancers. In these patients, non-melanoma skin cancer most commonly affects the nose. Depending on the disease’s stage, the surgical treatment of skin tumors can be quite challenging. 10 This is one of the rarest, and in this particular case, it is associated with a rare disease, XP, and an unusual location. Neuroendocrine carcinomas are classified into 3 categories: well differentiated (typical carcinoid), moderately differentiated (atypical carcinoid), and poorly differentiated (small and non-small cell types). The poorly differentiated neuroendocrine carcinomas are less common and have a bad prognosis due to its aggressive nature, characterized by an excessive capability for recurrence and metastasis (DM) irrespective of multimodal treatment. 2 Patients with xeroderma will first experience photosensitivity between the ages of 1 and 2 years. Compared to the general population, it increases the risk of developing various skin cancers such as basal cell carcinomas, malignant melanomas, and squamous cell carcinomas. In patients with XP, disease-causing mutations have been identified in 8 different genes. Due to its role in global-genomic nucleotide excision repair (GG-NER) and its participation in other DNA repair pathways, the DNA damage response, and transcriptional regulation, XPC is recognized as important for protecting against non-dermatological cancers. The XPC gene’s expression levels and polymorphisms likely impact the development of non-dermatologic cancers and may act as predictive and therapeutic biomarkers. DNA damage recognition protein called XPC is essential for the initiation of GG-NER. People carrying germline mutations in the XPC, are highly susceptibility to skin cancer due to defective removal via GG-NER of genotoxic, solar UV-induced dipyrimidine photoproducts. 11 It has been demonstrated that XP-C patients are more likely to acquire internal and skin malignancies. Patients with XP are 10-20 times more likely to develop internal cancers. Two young XPC patients with thyroid gliomas and one with neuroendocrine carcinoma were reported. 12 NENs involving head and neck structures and the nasopharynx are extremely rare. Diagnosing such neoplasms is difficult due to morphological features and the limited size of the biopsy specimens. These factors can make it difficult to differentiate them from other types of neoplasms. 13 Modern radiological imaging plays a revolutionary role in diagnosing and staging sinonasal tumors. It provides clear information about tumor invasion into important anatomical structures such as the skull base, orbit, and intracranial region. Additionally, functional MR technologies such as diffusion-weighted imaging and dynamic contrast enhancement imaging have demonstrated promise in differentiating between different sinonasal tumors. The diagnosis of small cell neuroendocrine carcinoma (SNEC) is based on the pathologic features of the specimen obtained during surgical resection. However, radiological imaging can provide preoperative diagnosis, which is most beneficial for early staging and treatment planning. 14
Depending on the comparative treatment of SNECs of the larynx and lungs, various approaches are indicated, including surgical resection, radiation therapy, chemotherapy, or a combination thereof. 15
Conclusion
SCNEC of the paranasal sinuses and nasopharynx is a high-grade tumor with a poor prognosis. More case reports are required to understand the clinical behavior of this rare group of tumors. Additional studies must be published to further understand the nature of the disease for better outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.