
Abstract
Neuroendocrine tumors are a spectrum of rare and highly heterogeneous neoplasms with distinct functional and biological behavior in relation to location, tumor size, and histological differentiation. Neuroendocrine tumors arise from the neuroendocrine cells of the diffuse neuroendocrine system located in almost every organ. Neuroendocrine tumors in the head and neck district are usually reported in sinonasal cavities and larynx. We present the case of a nasopharyngeal small-cell neuroendocrine carcinoma, which, as far as we know, is the 16th case reported in literature.
Introduction
Neuroendocrine tumors (NET) are a spectrum of rare and highly heterogeneous neoplasms with distinct functional and biological behavior in relation to location, tumor size, and histological differentiation. Neuroendocrine tumors arise from the neuroendocrine cells of the diffuse neuroendocrine system located in almost every organ. 1
The most common primary sites for NET are the gastroenteropancreatic system (about 70%) and the lungs (more than 25%), reflecting the high density of neuroendocrine cells in these organ systems.1,2
The histological category of neuroendocrine carcinomas includes carcinoid tumors, atypical carcinoid tumors, and small-cell carcinomas. Other synonyms for small-cell carcinoma include small-cell neuroendocrine carcinoma, oat cell carcinoma, anaplastic small-cell carcinoma, and small-cell neuroendocrine carcinoma of intermediate type. 3
Small-cell carcinomas in extrapulmonary sites (ESmCCs) are very rare. 4 They are about 5% of all small-cell neuroendocrine carcinomas. 5 Small-cell carcinomas in extrapulmonary sites originating in the head and neck account for approximately 10% of all ESmCCs, and there are few reports about this disease. Small-cell carcinomas in extrapulmonary sites have an aggressive natural history characterized by widespread metastasis. 4 It is characterized by high mitotic activity and areas of necrosis. 6 It is often associated with smoking, 7 unlike large cell neuroendocrine carcinoma that is related to EBV infection. 8 Small-cell carcinomas in extrapulmonary sites have an unfavorable clinical course and poor response to therapy; however, this is often a challenge due to overlapping pathology features. 5 Less than 15% of patients survive more than 5 years. 4 In the head and neck district, NET’s localization is described in sinonasal cavities and larynx.
According to the 2005 WHO classification of the sinonasal cavities’ tumors, 4 main categories of neuroendocrine neoplasms may be identified: typical and atypical carcinoids, small-cell carcinoma, and Neuroendocrine Carcinoma (NEC) not otherwise specified. Its differential diagnosis is first of all with sinonasal undifferentiated carcinoma and then with all neoplasms expressing neuroendocrine markers (olfactory neuroblastoma, paraganglioma, pituitary adenoma, or metastases). 9 There are few cases reported in literature about nasopharynx small-cell carcinoma 10 (Table 1).
Case Reported Nasopharyngeal Small-Cell Neuroendocrine Carcinoma.
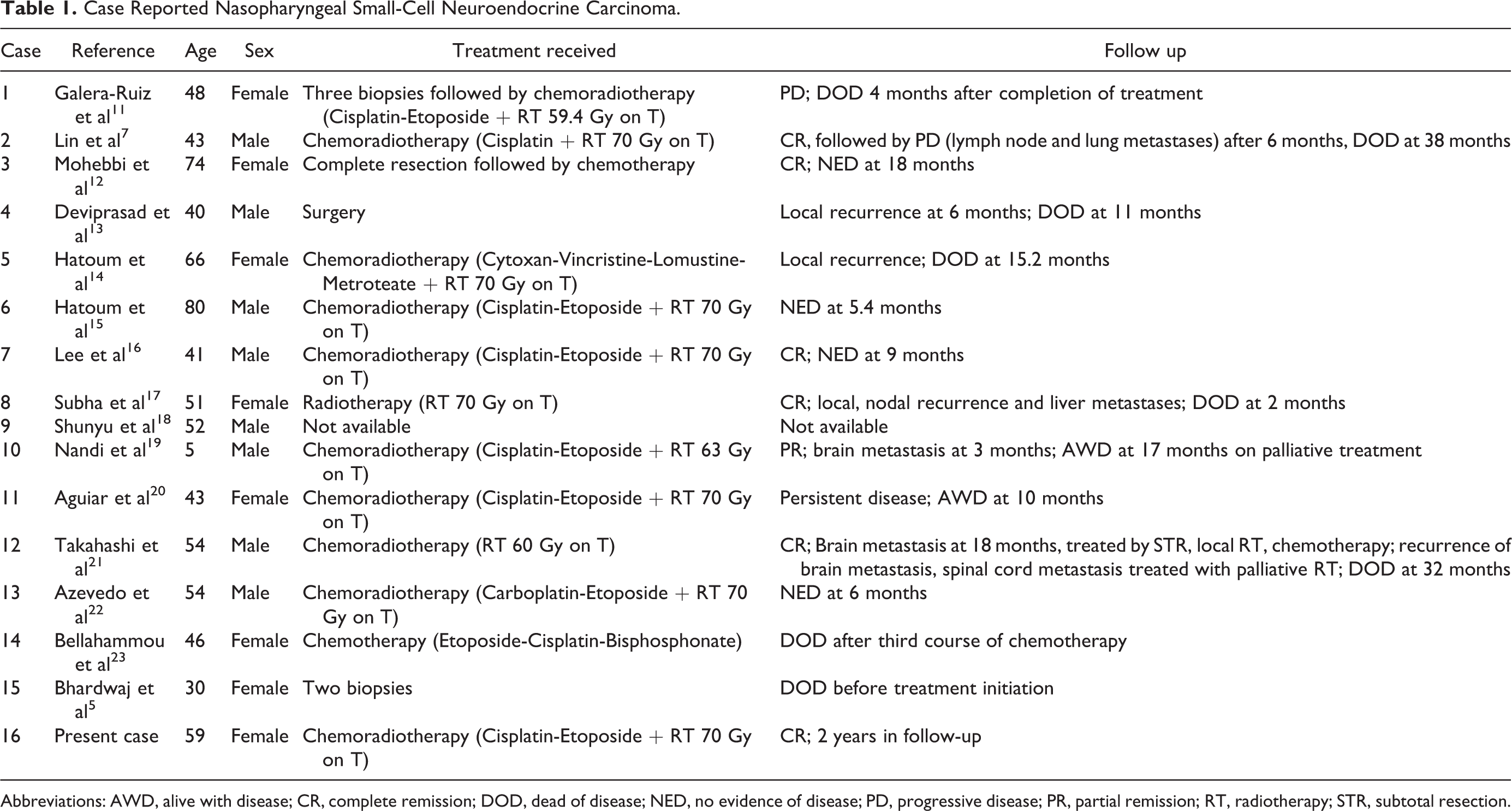
Abbreviations: AWD, alive with disease; CR, complete remission; DOD, dead of disease; NED, no evidence of disease; PD, progressive disease; PR, partial remission; RT, radiotherapy; STR, subtotal resection.
We present the case of a nasopharyngeal small-cell neuroendocrine carcinoma, which, as far as we know, is the 16th case reported in literature.5,7,11,13,16,18–21,23–26
Case Report
A 59-year-old female presented to our Clinic with nasal obstruction, ipsilateral epistaxis, and rhinorrhea for 2 months. A complete basal blood test was found normal, including blood and urine protein electrophoresis. With Fiber-optic endoscopy a friable neoformation was observed, blood striated, in the left nasal cavity and nasopharynx. Computed tomography (CT) performed with contrast showed the presence of an expansive tissue of the nasopharynx that appeared uneven after injection of contrast medium. The mass occupied the left choana and appeared not dissociable from the long muscles of the head. No adenopathies were found (Figure 1).
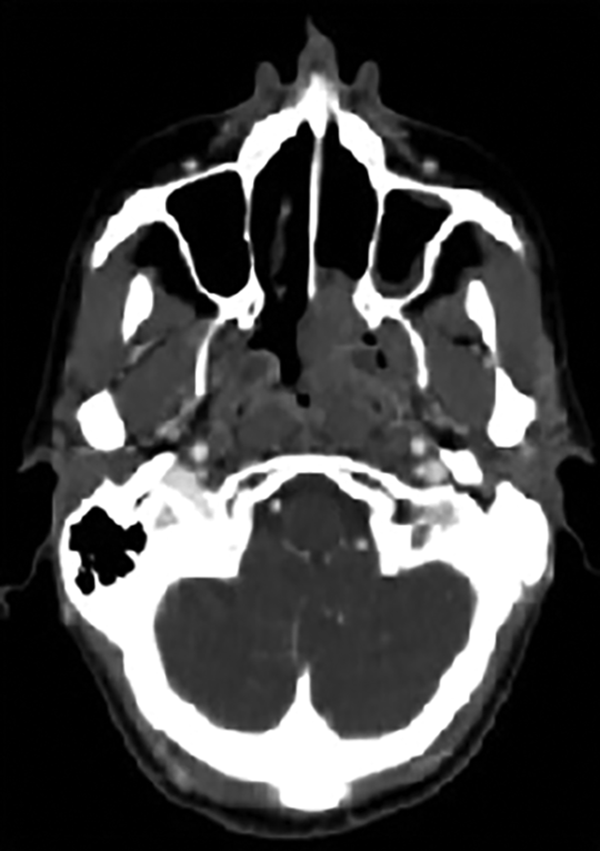
Pretreatment computed tomography (CT) with contrast.
Contrast-enhanced magnetic resonance imaging (MRI) confirmed the presence of the mass in both the nasopharynx and left nasal cavity with hyperintense signal in T1 and Fluid-Attenuation Inversion Recovery (FLAIR) sequences and hypointense signal in T2 (Figure 2).
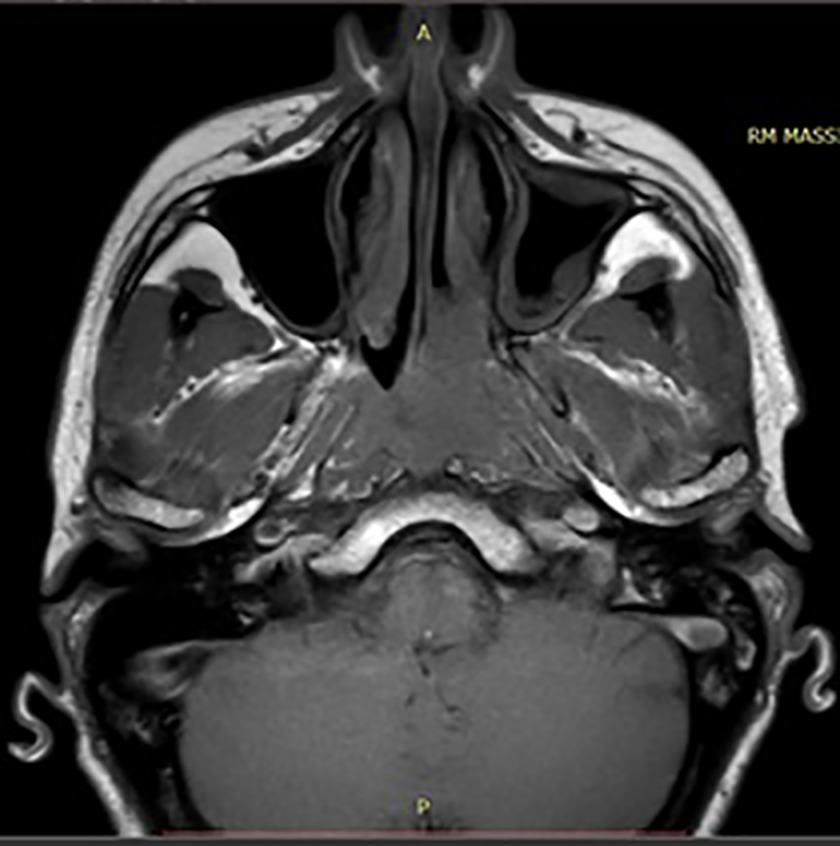
Pretreatment magnetic resonance imaging (MRI) with contrast.
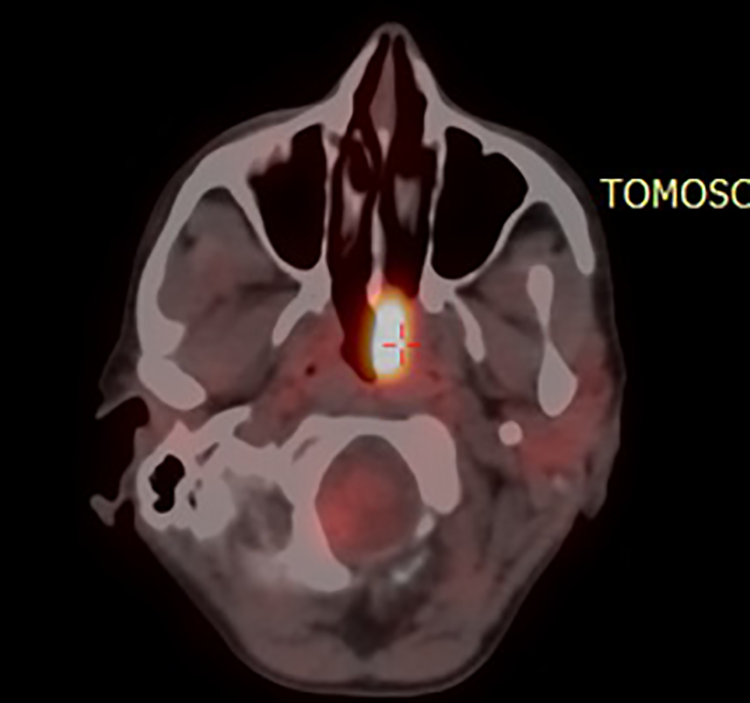
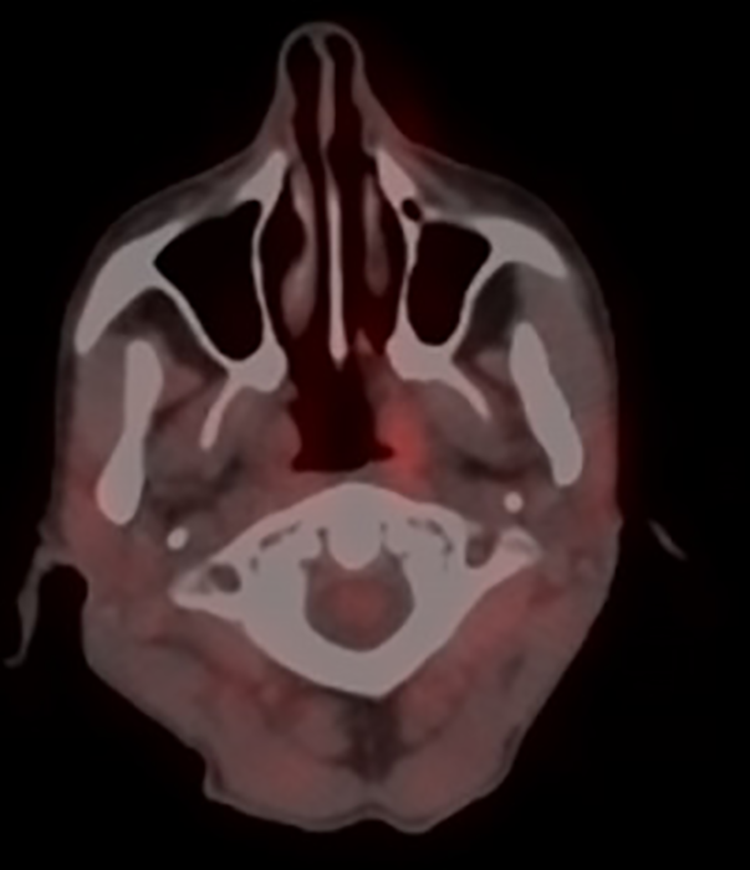
Total body positron emission tomography–CT (PET/CT; 68 FDG) revealed a pathological radiopharmaceutical’s uptake into the left nasopharyngeal region reaching the contralateral nasopharyngeal region (SUV max 14.5). The remaining districts analyzed were negative (Figure 3).
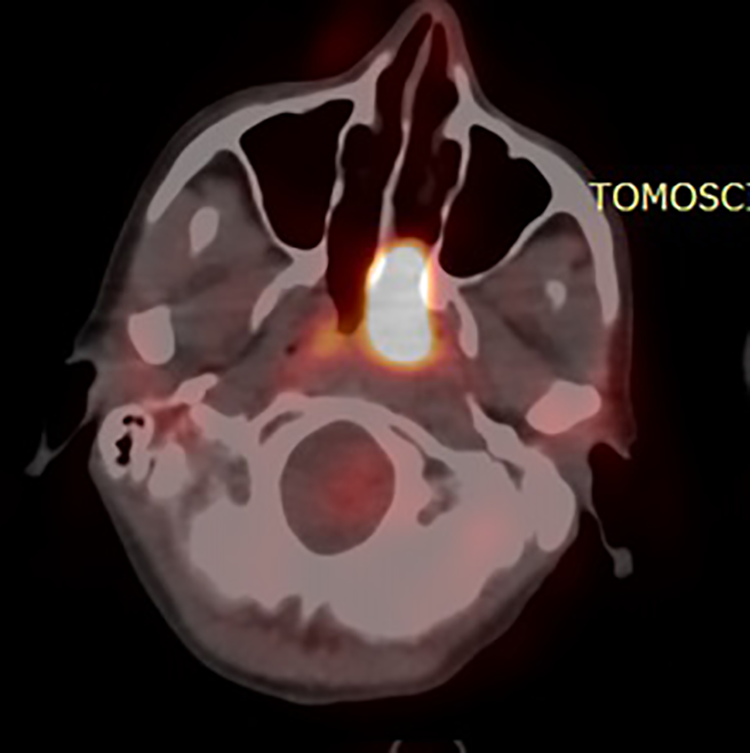
Pretreatment positron emission tomography–computed tomography (PET/CT) scan tumor.
A biopsy was performed from the nasal cavity under local anesthesia. Histological examination showed small-cell carcinoma with high malignancy’s grade (MIB: 70%) not EBV associated. Immunohistochemistry showed positivity to chromogranin, synaptophysin, pancytokeratin, and CD 56 (Figure 4).
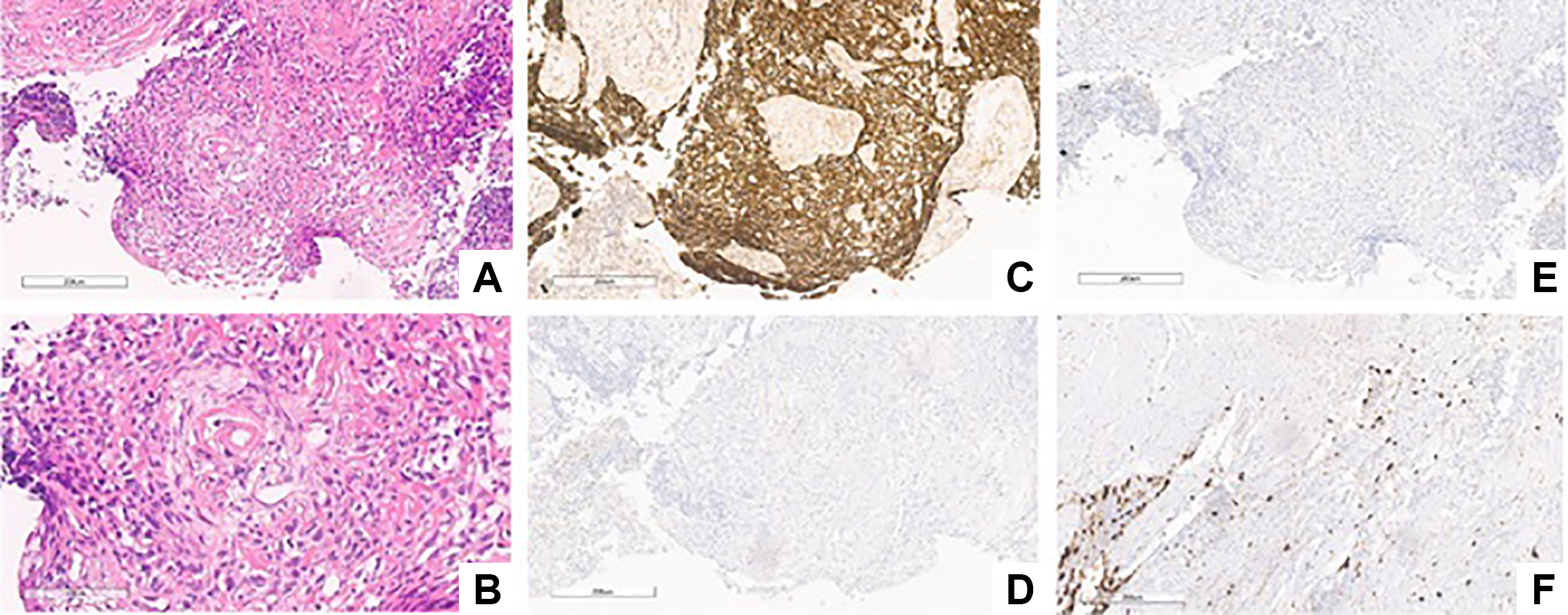
The ematossilina-eosin dichromatic coloring (EE) images (A, ×10 and B, ×20) show a tumor composed of small/medium-sized cells, gathered innodules and/or infiltrating the stroma. The cell nuclei are variably shaped, from roundish to spindle; cytoplasms focally show a clear perinuclear halo. Immunohistochemistry: strong expression for CKAE1/AE3 (C, ×10); negative expression for chromogranin (D, ×10); nonconclusive signal for synaptophysin (E, ×10); and irregular nuclear staining for Ki-67/MIB-1 (F, ×10).
The patient was treated with 3 cycles of neoadjuvant chemotherapy according to the Cisplatin-Etoposide scheme and then radiotherapy with a total dose of 70 Gy by linear accelerator. After 2 months of treatment, the patient repeated radiological imaging examinations.
Total body PET/CT (68 FDG) revealed a considerable reduction of radiopharmaceutical’s uptake of left nasopharyngeal region (SUV max 9.1) and absence of pathological tissue in the right region. The remaining districts analyzed were free from disease (Figure 5).
Positron emission tomography–computed tomography (PET/CT) total body after 2 months by treatment.
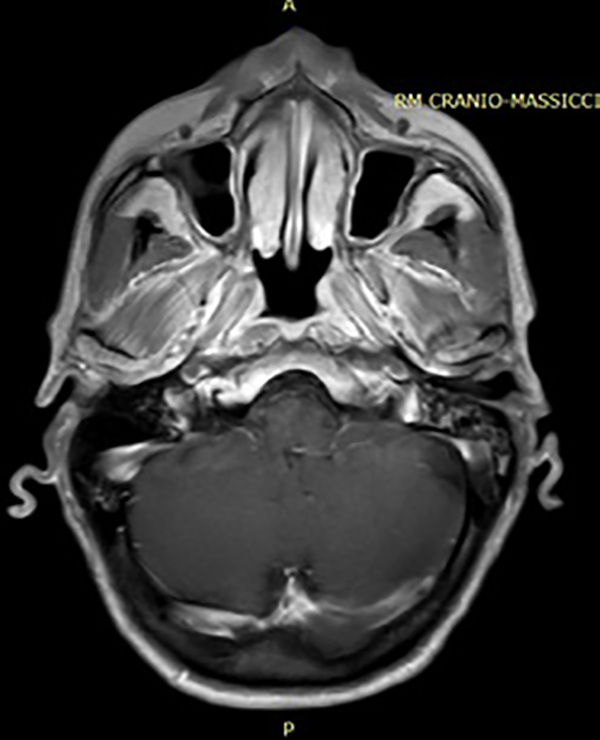
After 6 months after treatment, the patient repeated imaging studies. Maxillofacial MRI with contrast showed that the nasopharynx’s neoformation appeared significantly reduced. Absence of neck adenopathies (Figure 6).

Magnetic resonance imaging (MRI) with contrast after 6 months by treatment.
Total body PET/CT (68 FDG) showed a considerable reduction of the radiopharmaceutical’s uptake of the left nasopharyngeal region (SUV max 3.5). The remaining districts analyzed were normal (Figure 7).
Positron emission tomography–computed tomography (PET/CT) total body after 6 months by treatment.
After one year of treatment, imaging MRI with contrast was normal with a regular nasopharynx thickness and uniform contrast distribution. Absence of neck adenopathies (Figure 8).
Magnetic resonance imaging (MRI) with contrast after one year by treatment.
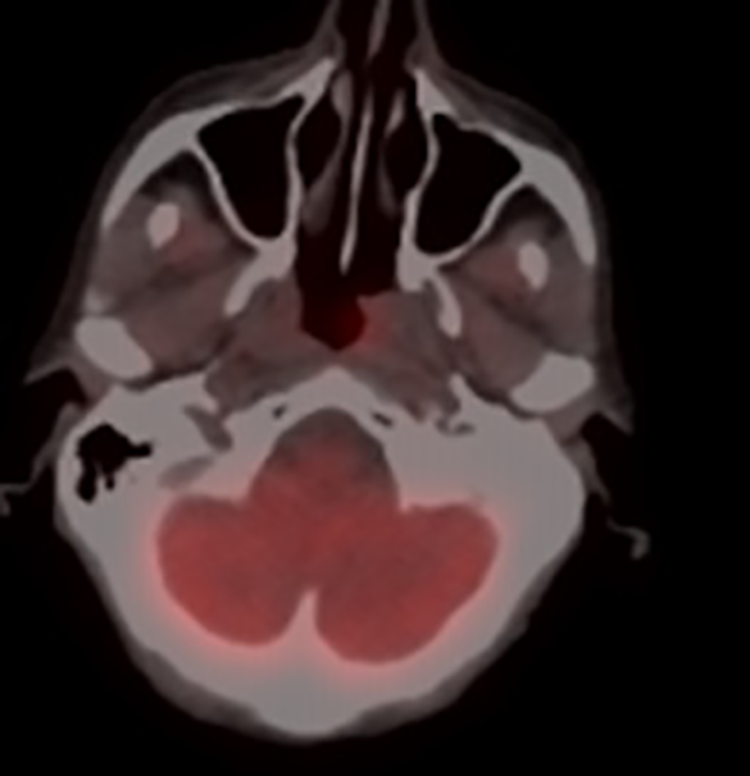
Total body PET/CT (68 FDG) showed absence of pathologic glucose’s accumulation of the examined nasopharynx tissues (Figure 9).
Positron emission tomography–computed tomography (PET/CT) total body after one year by treatment.
Nowadays, after 2 years from therapy, no recurrence has been observed at endoscopy and imaging studies.
Discussion
Small-cell carcinoma is a rare entity in nasopharynx. This kind of tumor is extremely aggressive, especially in larynx (5-year survival rate of 48%) more than the lung localization (5-year survival rate of 58%), probably because of those cases that should be classified as large-cell NEC. Immunohistochemistry is highly important for a correct diagnosis and to confirm epithelial and neuroendocrine nature of a small-cell carcinoma which expresses variably cytokeratin’s and neuroendocrine markers such as synaptophysin, neuron-specific enolase, chromogranin, and CD56.10,22
Multiple medical therapies have become available for the treatment of metastatic NET. All have shown their effect in randomized controlled trials, but head-to-head comparisons are not available. 27 The therapeutic options are surgery, radiotherapy (RT), Chemotherapy + RT (CRT), and chemotherapy. In the case of ESmCCs in the head and neck region, CRT is also a common treatment in both early and locally advanced disease. 4 Database analyses and other previous reports of ESmCCs in the head and neck district elucidated that the addition of surgery to RT and chemotherapy in patients with locally advanced disease did not result in improved survival compared with treatment with only RT and chemotherapy.4,7,26
Combined RT and CT are the standard approaches and surgery is reserved for limited cases such as initial disease or local relapse. After treatment, patients with extrapulmonary small-cell carcinoma have median survivals of 8 to 16 months. 20
Despite the lack of a consensual therapeutic modality, the multimodality approach (chemo and radiotherapy) showed an increase of the overall survival rate of patients with a sinonasal small-cell neuroendocrine carcinoma diagnosis. 22
No specific guidelines exist at present, various chemotherapeutic combination regimens have been explored in the first-line treatment including cisplatin and etoposide or Cyclophosphamide, Adriamycin, and Vincristine or Adriamycin, Cyclophosphamide and etoposide and Ifosfamide, carboplatin, and etoposide. 23
However, the best therapeutic results in locally advanced nasopharynx’s NET have been obtained using a small-cell lung cancer treatment regimen, consisting of a combination of chemotherapy (cisplatin + etoposide) and radiation therapy.5,7,11-14,16,19,20,22,24
Proper diagnostic criteria and treatment protocols need to be established to detect cases at an early stage and for an appropriate management, in order to limit morbidity and mortality.5,18,21,25
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.