
Abstract
Objectives:
Masses in the parapharyngeal space often pose a diagnostic and therapeutic challenge due to an inaccessible location for biopsy and proximity to critical neurovascular structures of the neck. The aims of this study are to describe a rare case of Castleman disease (CD) presenting in the parapharyngeal space.
Methods:
Case report of a 38-year-old male presenting to a tertiary care center and literature review.
Results & conclusions:
The parapharyngeal space is an unusual location for CD. Surgeons, radiologists, and pathologists must be aware of this disease entity within the differential diagnosis to provide appropriate perioperative counseling for patients.
Introduction
In 1956, Benjamin Castleman first reported the histologic findings of a mediastinal mass in a 40-year-old male with lymph node hyperplasia and follicles with small hyalinized foci. This pathology entity was subsequently termed Castleman disease (CD). Castleman disease has since been recognized as a rare heterogeneous group of lymphoproliferative disorders, and further knowledge has led to classification based on focality, histology, and etiologies of the disorder. 1 Idiopathic, unicentric Castleman disease (UCD) often presents as asymptomatic lymphadenopathy.1,2 Rarely, symptoms will be reported by patients due to mass effect. The head and neck is the second most commonly affected region of the body in CD after the mediastinum. 1 Only 4 cases of parapharyngeal CD have been previously reported in the literature.
Case Report
A 38-year-old male was referred to a head and neck clinic for incidental imaging findings after presenting to a tertiary-care hospital with 24 hours of self-resolving left-sided facial numbness. The patient was asymptomatic at the time of specialist evaluation, healthy, and had no past medical history. Physical examination was unremarkable and did not reveal any cranial nerve deficits, facial numbness, facial weakness, neck masses, or lymphadenopathy. Office flexible nasolaryngoscopy was unremarkable. Consent was obtained for photo documentation and use of images and de-identified information for research and publication purposes.
Magnetic resonance imaging (MRI) was negative for intracerebral pathology, but revealed a 4.3 × 3.1 × 1.9 cm left poststyloid parapharyngeal mass (Figure 1). The well-circumscribed mass was T1-isointense and T2-hyperintense, contained regions of central low intensity, and exhibited peripheral enhancement on contrast administration. There was posterolateral displacement of the internal carotid artery and internal jugular vein with no encasement or invasion. No cervical lymphadenopathy was noted. Preoperative differential diagnosis included a schwannoma versus pleomorphic adenoma given its location in the poststyloid parapharyngeal space and MRI findings of T2-hyperintensity and enhancement. In discussion with the interpreting radiologist, the mass was thought to be incidental and physiologically unrelated to the patient’s initially presented altered facial sensation.
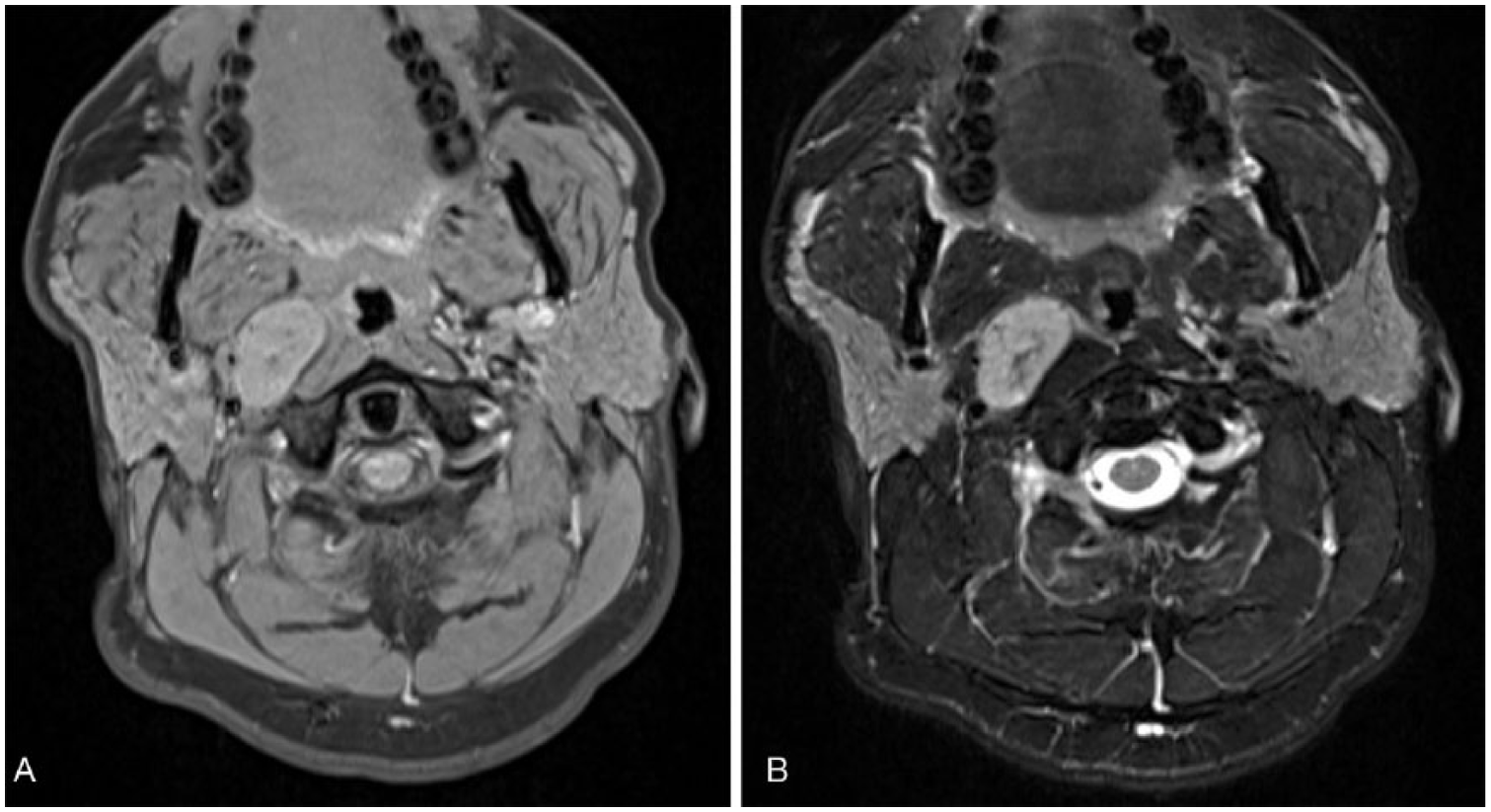
Magnetic resonance imaging of the patient demonstrating a right parpapharyngeal mass with posterolateral displacement of the internal carotid artery. Mass demonstrating (A) T1-weighted isointensity and (B) T2-weighted hyperintensity to surrounding musculature.
After discussion with the patient, a decision was made to surgically remove the mass for diagnostic purposes. Intraoperatively, the parapharyngeal space was entered through a transcervical approach with removal of the submandibular gland. The stylohyoid and posterior belly of the digastric muscle were inferiorly retracted to identify the mass, and it was bluntly dissected free from surrounding tissues (Figure 2). Intraoperative inspection and recurrent laryngeal nerve monitoring confirmed that the mass was not arising from the vagus nerve, another nervous structure, or surrounding vasculature. Hemostasis was achieved with bipolar cautery, and a Jackson-Pratt drain was placed into the wound bed. No complications were encountered, and the patient was kept overnight for observation with the drain removed prior to discharge. Postoperative flexible nasolaryngoscopy revealed normal vocal fold function bilaterally.

Gross intraoperative appearance of surgically excised right parapharyngeal mass.
Pathologic review of the mass revealed a parapharyngeal lymph node with features consistent with the hyaline-vascular subtype of CD, as shown by atretic follicles with “onion-skinning” of mantle zone lymphocytes, sclerotic blood vessels radially penetrating follicles, and marked interfollicular proliferation of sclerotic blood vessels (Figure 3). Immunohistochemistry for human herpesvirus 8 (HHV-8) and in situ hybridization for Epstein-Barr virus (EBV) were negative. Four small additional lymph nodes adjacent to the submandibular gland exhibited similar characteristics. Postoperative serologic workup to rule out human immunodeficiency virus (HIV), toxoplasmosis, and mononucleosis was negative.

(A) Parapharyngeal lymph node (H&E, 20×). (B) Parapharyngeal lymph node (H&E, 100×).
Given that the patient had no systemic symptoms suggestive of a multicentric disease process, and initial imaging had ruled out other cervical and mediastinal lymphadenopathy, a diagnosis of UCD was established. No further imaging or treatment was deemed necessary at this time, and the patient was discharged from follow-up after his first postoperative visit 3 weeks after surgery. He was instructed to contact his surgeon if needed if he developed any systemic symptoms or new lymphadenopathy anywhere in the body.
Discussion and Literature Review
Clinical characteristics of CD
Three main subtypes of CD have been universally described based on distinctive causative factors. Unicentric Castleman disease typically presents as an idiopathic asymptomatic mass, most commonly in the mediastinum and head and neck region. 1 Chang et al. have described clonality of UCD of likely stromal or follicular dendritic cell origin. 3
Studies based on insurance claims database screening have suggested the incidence of UCD to be approximately 16 per million. 4 A systematic review performed in 2012 of 404 CD cases identified a total of 278 cases of UCD (68%). The patients had a median age presentation at 34 years (ranging 2-84 years) and a slight female predominance (60%). 2 Of the 278 cases, the average size of involved lymph nodes was 5.5 cm, and the main sites of disease were the mediastinum (29%), head and neck (23%), abdomen (21%), and retroperitoneum (17%). 2
Conversely, multicentric Castleman disease (MCD) will typically present with generalized lymphadenopathy, hepatosplenomegaly, fevers, night sweats, and weight loss. Some patients will also develop an inflammatory vascular leak syndrome leading to pleural edema, ascites, pericardial effusions, and pleural effusions. 5 Other manifestations include anemia, thrombocytopenia, factor VIII deficiency, obliterative bronchiolitis, glomerulonephritis, and pemphigus. 5 Multicentric Castleman disease can further be subclassified into association with human herpesvirus 8 (HHV8) versus idiopathic MCD.1,5
Radiologic characteristics of CD
Radiologic characteristics of CD in the neck were described by Jiang et al 6 in a review of 21 cases. Twenty were of the unicentric hyaline-vascular type. Nine of these cases were solitary masses, and 11 cases were dominant masses with small satellite disease. The masses were located in level II (12 cases), level I (4 cases), level III (3 cases), and the parapharyngeal space (1 case). Computed tomography (CT) imaging in 15 of 16 patients revealed homogeneous, well-defined masses, with 1 case exhibiting a heterogeneous appearance without calcification. Magnetic resonance imaging revealed well-defined homogeneous isointense-to-muscle masses on T1 sequencing with intermediate contrast enhancement and intermediate-hyperintense masses on T2 sequencing. 6
Pathologic characteristics of CD
Castleman disease can be classified into 2 main histologic variants: hyaline-vascular and plasma cell. Unicentric Castleman disease has been found to have hyaline-vascular histology 95% of the time.7,8 Hallmark findings include aggregates of follicular dendritic cells or atrophic follicles with radially penetrating vessels.5,8 Lymphocytes will often form layers around dendritic cells, creating the appearance of “onion skin” layers. Interfollicular zones will often have vascular proliferation with perivascular hyalinization. The main pathologic differential diagnosis includes reactive follicular hyperplasia, follicular lymphoma, plasmocytomas, autoimmune-associated lymphadenopathy, infectious causes (HIV and toxoplasmosis), and IgG-4-related disease. 5 Multicentric Castleman disease is often associated with the histologic plasma cell variant subtype, which is typically a diagnosis of exclusion and may lack defining histologic attributes.
The authors also advocate for use of the Castleman Disease Collaborative Network (available at https://www.cdcn.org) where patients and physicians can learn about CD, access recent landmark literature, enroll in active research studies, and communicate with other patients afflicted with CD.
Treatment of UCD
Surgical resection is considered the cornerstone of curative treatment for UCD and is the most widely accepted therapy in the literature. A systematic review by Talat et al 2 of 278 unicentric patients found that surgical resection resulted in 95% overall survival and 81.2% disease-free survival at 3 years. More specifically, of the 51 patients with unicentric neck disease, only 1 (1.8%) patient had death due to disease. A second study by Chronowski et al 9 described 8 patients with UCD, of which 6 were treated with complete resection and 2 with partial resection. All surgically treated patients were alive and disease free at the time of review. Four additional patients were treated with radiotherapy alone. At an average follow-up of 30 months, 2 patients were alive and disease free, while 2 patients had died without evidence of disease secondary to a motor vehicle accident and complications of pemphigus vulgaris, respectively.
Castleman disease in the parapharynx
To date, there have only been 4 previous reports of CD localized to the upper parapharyngeal space (Table 1). Including the current reported case, 2 were in female patients and 3 were in male patients. The patients’ ages ranged from 16 to 42 years, with a median of 38 years. Lesion size ranged from 4.3 to 9 cm in greatest dimension. 10 All cases were surgically excised with minimal complications, and all were found to be unicentric and of the hyaline-vascular subtype on histologic review.10–13
Previous case reports describing unicentric Castleman disease in the parapharyngeal space.

A significant proportion (47%) of parapharyngeal masses comprised neoplasms from minor salivary glands or deep lobe parotid, particularly in the prestyloid space. 14 Neurogenic tumors such as schwannomas and paragangliomas are also common (34%), 14 but are more likely to be localized to the poststyloid space due to their originating structures. 15
The authors would like to emphasize the difficulties and challenges with the preoperative diagnosis of CD of the parapharyngeal space due to its relatively inaccessible location for definitive tissue biopsy. With the limited numbers of cases in the literature, it is difficult to ascertain disease-specific imaging characteristics, although all previous cases have been described as being isointense on T1-weighted sequences and hyperintense on T2-weighted sequences. Furthermore, all reported cases have demonstrated lateral or posterolateral displacement of the internal carotid artery and abutment of the skull base.
For masses with T1-weighted isointensity and T2-weighted hyperintensity, parapharyngeal schwannomas of vagal and sympathetic chain origin rise to the top of the differential diagnosis. 15 An initial study by Furukawa suggested that splaying of the internal carotid artery and internal jugular vein is suggestive of a vagal schwannoma diagnosis. 16 Those of sympathetic chain origin will typically displace both vessels concurrently without splaying. However, subsequent studies have suggested that this is not a universal finding. 17 A multivariate-model analysis by Graffeo et al 18 predicted a 75% probability of vagal schwannoma in the presence of splayed vessels with anteromedial displacement of the carotid and an 87% probability of sympathetic chain schwannoma in the absence of splaying with lateral displacement of the carotid. Knowledge of these radiologic clues may guide surgeons to a more accurate preoperative diagnosis and allow for improved counseling and decision making with the patient regarding operative treatment.17,19 Another possible diagnosis to consider would be minor salivary gland neoplasms, such as benign mixed tumors. 15
Conclusions
This case is a reminder that CD may present as a mass within the parapharyngeal space, but is an exceedingly rare entity. With the number of reports increasing, radiologic findings may provide subtle diagnostic clues. However, open biopsy and excision of the lesion are crucial to accurate diagnosis. Once excised, no additional treatment is necessary, and overall prognosis is excellent for patients. The authors advocate for awareness of this rare clinicopathologic entity in the workup and treatment of parapharyngeal space masses.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
DC: Primary author of manuscript, editting and revision of manuscript;
KB: Revision of manuscript, secondary author, provision of figures;
AT: Principal investigator, editting of manuscript.