
Abstract
Unilateral tonsillar enlargement is a common indication for tonsillectomy, but there are varying rates of malignancy among tonsils removed for asymmetry and a lack of clear guidelines for management within the literature. Lymphoma of the palatine tonsils is among the concerns leading to tonsillectomy, but chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) of the tonsil is rare. We report a case of primary CLL/SLL of the palatine tonsil in a 51-year-old gentleman who presented with tonsillar asymmetry and obstructive sleep apnea (OSA) but lacked signs and symptoms suspicious for malignancy, including lymphadenopathy and “B-symptoms.” To our knowledge, only 7 cases of CLL/SLL of the palatine tonsil have been reported in the English literature, with the tonsil being the primary site of involvement in only 4 of those cases. Our unique case highlights the importance of thorough physical exam, family history, and tissue biopsy in patients presenting to the otolaryngologist with OSA and asymmetric tonsils.
Introduction
Tonsillectomy is a frequently performed procedure by otolaryngologists for the management of obstructive sleep apnea (OSA), recurrent tonsillitis, or for tissue diagnosis in the setting of asymmetric tonsils. 1 Traditionally, it has been taught that unilateral tonsillar enlargement (UTE) requires tonsillectomy for tissue diagnosis due to the risk of malignancy, which can include squamous cell carcinoma or lymphoma.2,3 However, rates of malignancy in patients who undergo tonsillectomy for UTE vary widely within the literature—ranging from as low as 5%4 -6 up to 39%. 7 Non-Hodgkin lymphoma of the head and neck most commonly occurs within Waldeyer’s ring, 8 with the tonsils accounting for 80% of cases.9,10 Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) of the tonsil is exceedingly rare, with only 7 cases reported in the English literature and only 4 with the tonsil as the initial site identified. 11 We recount a unique case of a middle-aged male with UTE that was found to have CLL/SLL involving bilateral tonsils.
Case Report
A 51-year-old male with a 15-year history of mild OSA diagnosed by sleep study presented to clinic for the evaluation of a possible tonsillectomy for management of OSA. He also reported a history of frequent infections associated with enlarged tonsils and an 11-year history of asymmetric tonsils. He denied constitutional symptoms but did endorse apnea and snoring consistent with his known diagnosis of OSA. Family history was significant for myelodysplastic syndrome in his mother, diagnosed 1 year prior. Physical exam revealed 4+ palatine tonsils on the right and 2+ palatine tonsils on the left. Neck exam was without lymph-adenopathy.
He underwent total tonsillectomy primarily for airway management and secondarily for tissue diagnosis 1 month later. Bilateral total tonsillectomy was performed in standard fashion via monopolar cautery dissection on an outpatient basis. Specimens were sent fresh for lymphoma workup. Surgical specimens measured 4.0 cm × 2.7 cm × 1.7 cm on the right and 4.7 cm × 2.3 cm × 1.7 cm on the left. Gross examination of the left tonsil revealed a tan, fleshy, smooth surface with pitted architecture and a moderate number of green-gray debris occupying pits. Grossly, the right tonsil had a homogeneous pink-tan fleshy cut surface with crypt architecture. No masses or lesions were grossly appreciated on either tonsil.
Pathology results revealed that the normal architecture was effaced by small mature lymphocytes with irregular nuclear contours and scant cytoplasm. The neoplastic cells were positive for CD5, CD20, CD23, CD43, BCL-2, and LEF1 and negative for CD10, BCL6, and Cyclin D1 by immunohistochemistry. Concurrent flow cytometric analysis of both tonsils revealed that an atypical dim kappa-restricted B-cell population was also positive for CD5, CD19, dim CD20, and CD23 and negative for CD10, CD25, and lambda light chain. The overall findings support a diagnosis of kappa-restricted CD5/CD19 double positive B-cell population consistent with CLL/SLL of bilateral tonsils. Pathology slides are depicted in Figure 1.
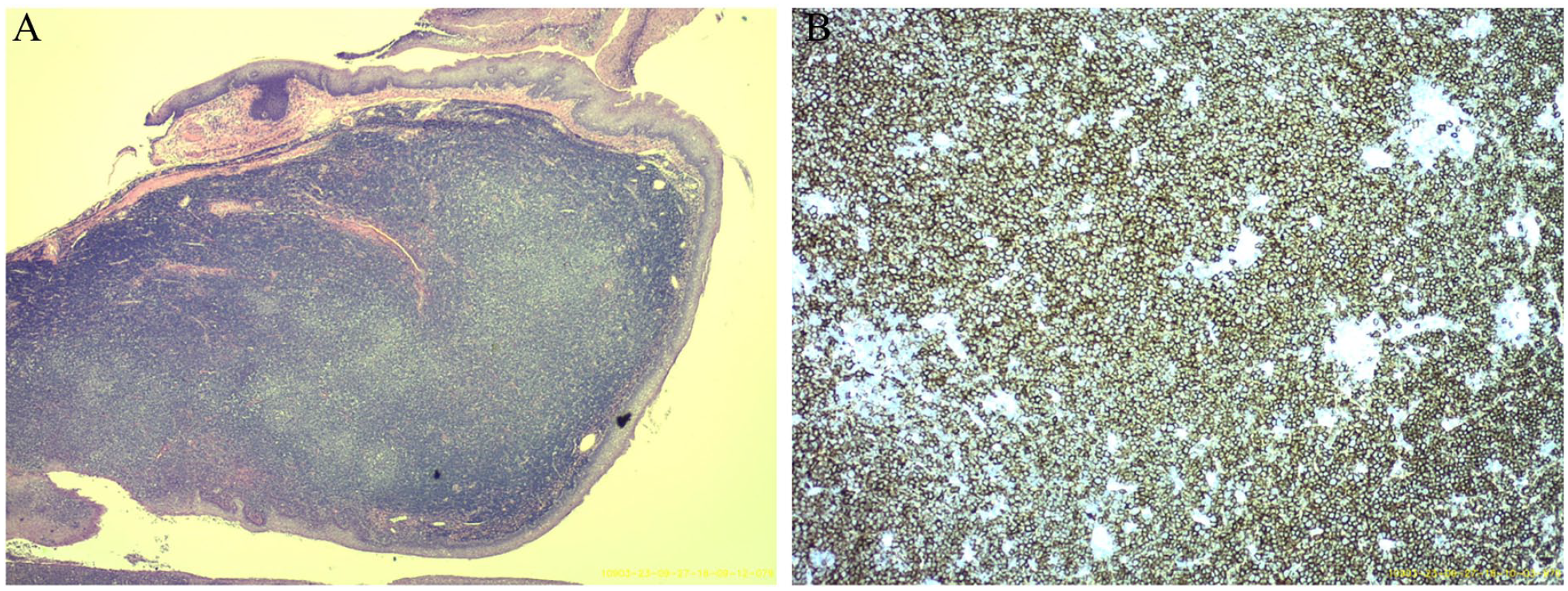
Hematoxylin and eosin preparation of the left palatine tonsil at 2× magnification (A). CD 20 immunostaining of the left palatine tonsil at 10× magnification (B).
Pathology results were discussed at the 1-month follow-up visit after surgery. Flow cytometric analysis of the peripheral blood revealed a kappa-restricted monoclonal B-cell population (1218/µL) The patient was referred to the Department of Hematology/Oncology for further workup, staging, and management of his newly diagnosed CLL/SLL.
Discussion
We report a unique case of bilateral tonsillar CLL/SLL that presented as OSA and tonsillar asymmetry. UTE is a frequent reason why patients undergo tonsillectomy due to concern for malignancy; however, there are varying rates of malignancy reported in the literature in patients who underwent tonsillectomy for UTE.4,6,7 Recently, growing pediatric literature revealed low rates of malignancy in children who underwent tonsillectomy for UTE with about 75% of asymmetric tonsils being a result of benign causes. 12 However, there is a paucity of literature within the adult population. Addison et al. 1 recount a 32% rate of malignancy in patients with UTE and cervical lymphadenopathy, compared with 0% in patients with UTE alone, indicating that lymphadenopathy is an important finding that should heighten a clinician’s suspicion for malignancy. Hwang et al. 13 propose a pathway for evaluation and management of UTE in adults, suggesting periodic follow-up in patients with isolated UTE and imaging with PET or Positron Emission Tomography/Computed To-mography (PET/CT) or tissue sample in patients with additional findings, including lymphadenopathy, abnormal tonsillar consistency or appearance, “B-symptoms,” or history of malignancy. 13 Tonsillectomy is preferred over deep tonsil biopsy for tissue diagnosis. 14
Interestingly, our patient lacked symptoms or physical exam signs consistent with malignancy. Notably, he did have a family history of myelodysplastic syndrome in his mother. While there are no documented reports of CLL/SLL being linked with myelodysplastic syndrome, family history could be a key indicator for increased malignancy risk in patients with UTE. Our patient did present with OSA, which is a common presentation of tonsillar CLL/SLL, as 4 of the 7 cases of tonsillar CLL/SLL in the English literature were associated with OSA. 11
Interestingly, although the tonsils appeared asymmetric on physical exam, surgical specimens were similar in size. The literature reveals varying correlations between tonsillar size assessment on oral exam and size at the time of surgical removal. Addison et al. 1 found that suspicious tonsils are significantly more likely to be larger at the time of surgery, but Harley 15 found no difference in the degree of asymmetry. This could be the result of tonsils sitting at varying depths within the tonsillar fossa.
Conclusion
Tonsillar CLL/SLL is exceedingly rare within the literature but can manifest with OSA. Our patient highlights the importance of conducting thorough physical exam, family history, and tissue biopsy in patients presenting with OSA and asymmetric tonsils.
Footnotes
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, AMO.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because our institution does not require approval for individual cases.