
Abstract
Introduction
Pediatric obstructive sleep apnea (OSA) is a disorder of sleep in which partial or complete airway obstruction leads to impaired ventilation. It is accompanied by snoring, breathing pauses, and awakenings that can result in behavioral problems.1,2 OSA is diagnosed by polysomnography (PSG), which can also quantify the severity of the disorder.3,4 Adenotonsillectomy (T&A) is the first-line surgical intervention for pediatric OSA. 4
T&A is commonly performed in children over 3 years and often resolves OSA. 5 Children under 3 years less frequently undergo T&A but experience improvement in quality of life—caregiver concerns, physical suffering, and sleep disturbance—and in sleep parameters –apnea-hypopnea index/AHI, baseline oxygen saturation, minimum oxygen saturation, and sleep efficiency.5-9 T&A for OSA can also contribute to reduction in anxiety, emotional lability, and aggression. 7
Despite observed clinical improvements in OSA in children under 3, concerns remain about limited outcomes data in this group. Young children undergoing T&A are more likely to have increased risk of post-operative complications such as respiratory compromise, require overnight observation, and have persistent OSA and adenoid tissue regrowth.3,5,8,9 Children under 3 years with OSA are also more likely to present with comorbidities (e.g., gastroesophageal reflux disease (GERD), prematurity, and cardiovascular malformations).10,11
In a previous study of 413 children under 3 years of age, we reported that young children with OSA were more likely to be male and have GERD. We showed that Down syndrome and tonsillar hypertrophy were predictors of severe OSA in children under 3 years and recommended further studies on the outcomes of T&A for OSA in children under 3. In addition, an updated Clinical Practice Guidelines for Tonsillectomy in Children 12 highlighted the need for studies determining percentage of patients who have full, partial, or no resolution of OSA and the impact of PSG findings to determine who would benefit from post-operative PSG. This study addresses this knowledge gap in young children. Previous studies have been limited by small study populations, lack of PSG for objective diagnosis and quantification of OSA, and lack of racial/ethnic diversity.
The objectives of this study are to identify predictors of OSA after T&A, especially persistent severe OSA, and to describe the characteristics of children with OSA undergoing T&A in an ethnically diverse population of children under 3 years of age.
Patients and Methods
Surgical Procedure
All children in the study underwent complete adenotonsillectomy for OSA. Tonsils were removed bilaterally using guided Bovie monopolar electrocautery, and adenoids were removed using suction cautery.
Study Participants
This study was IRB approved (STU 042014-001), with need for consent exempted. This retrospective observational study included children under 3 years who had T&A at Children’s Medical Center Dallas/UT Southwestern between August 1, 2012 and March 1, 2020. Data was collected from electronic medical records (EPIC® production, Version August 2018). AHI was used to define OSA, and pre- and post-operative PSG were required for objective comparison. Children were excluded if they did not undergo T&A, have pre- and post-T&A PSG, or have complete data. Data was also collected from the first 100 children under 3 years who underwent T&A without post-operative PSG, for comparison.
Collected Information
We scanned clinic and PSG notes to collect the following data: age in years at time of pre- and post-operative PSG and T&A, sex, race/ethnicity, birth status, height (cm), weight (kg), tonsil size, presence of comorbidities (allergic rhinitis, asthma, GERD, down syndrome (DS), craniofacial abnormalities, neuromuscular disorders, or sickle cell disease), and post-operative complications.
We defined sex as male or female. Race/ethnicity was self-selected by the caregiver as White/Caucasian, Black/African American, Hispanic, or other (includes Asian and Mixed). We classified birth status into pre-term (gestational age under 37 weeks) or full-term. The World Health Organization Child Growth Standards BMI-for-age from birth–2 years and 2–5 years was used to calculate BMI z-score using height and weight at time of first PSG. 13 Children were placed into CDC-defined BMI categories based on age-and-sex adjusted BMI percentiles and were then categorized as non-obese (<95th percentile BMI) or obese (≥95th percentile BMI). 13 Tonsil size was defined by the Brodsky grading scale, with tonsillar hypertrophy defined as tonsil grade of 3+ or 4+. 14 Comorbidities were obtained from the problem list. Post-operative complications included bleeding, re-admissions, and recurrent surgery within 3 months of T&A.
Parameters recorded from pre- and post-T&A PSG reports included sleep efficiency, percentage of REM sleep, arousal index, central apnea index (CAI), obstructive apnea-hypopnea index (AHI), oxygen saturation nadir (SaO2 nadir), peak CO2, percentage of time spent under 90% oxygen saturation, and percentage of time spent over 50 mmHg CO2. We defined sleep efficiency as percentage of study time that the patient was asleep. We defined arousal index as number of arousals from sleep that the patient experienced per hour. An obstructive apnea was defined as ≥90% reduction in oronasal airflow for greater than two respiratory cycles despite respiratory effort. 15 A hypopnea was defined as decrease in airflow of ≥30% for at least 2 breaths accompanied either by an arousal or 3% decrease in oxygen saturation. 16 AHI was represented by number of obstructive apnea and hypopnea events per hour of sleep. CAI was defined as number of central apnea events per hour of sleep. We defined OSA as AHI greater or equal to 1, with mild OSA as AHI of 1–4.99, moderate OSA as AHI of 5–9.99, and severe OSA as AHI greater or equal to 10. 17
Statistical Analyses
Continuous data are presented as means with standard deviations (SD) and categorical data as counts with percentages. Demographics, comorbidities, and pre-T&A PSG parameters were compared between children with and without post-T&A PSG. Differences between pre- and post-PSG parameters were compared using the student’s t test. Demographics, comorbidities, and pre-T&A PSG findings were also compared within three groups: post-T&A AHI ≥1 versus <1, AHI ≥5 versus <5, and AHI ≥10 versus <10. We performed univariate analysis to determine differences between groups, using analysis of variance (ANOVA) for continuous variables and the Pearson X2 test for categorical variables.
To describe the relationship between persistent severe OSA and demographic and clinical factors, we performed a multiple logistic regression analysis. We used forward stepwise regression of variables that showed significance in the univariate analysis (i.e., ANOVA and X2 test), followed by sequential removal within the logistic model of non-significance variables until the final model was determined. The model’s goodness of fit was determined with the Hosmer–Lemeshow test and validated with jackknife regression. Based on an assumption that 25% of children referred for PSG have severe OSA, a power analysis showed that detecting a 20% difference at the P < .05 level in severe OSA rates would require approximately 78 patients with pre- and post-T&A PSG. 18 All statistics were performed with Stata Statistical Software, Version 16, College Station, Texas. Significance was set at P < .05.
Results
A total of 439 children under 3 years of age underwent PSG during the study period, of which 229 were excluded because they did not undergo T&A and 123 were excluded because they did not have post-T&A PSG. The final study population included 87 children with post-T&A PSG that were compared to the first 100 children who underwent T&A without post-operative PSG.
Baseline Characteristics of Children under 3 years with OSA: A Comparison of Children With and Without Post-T&A PSG.
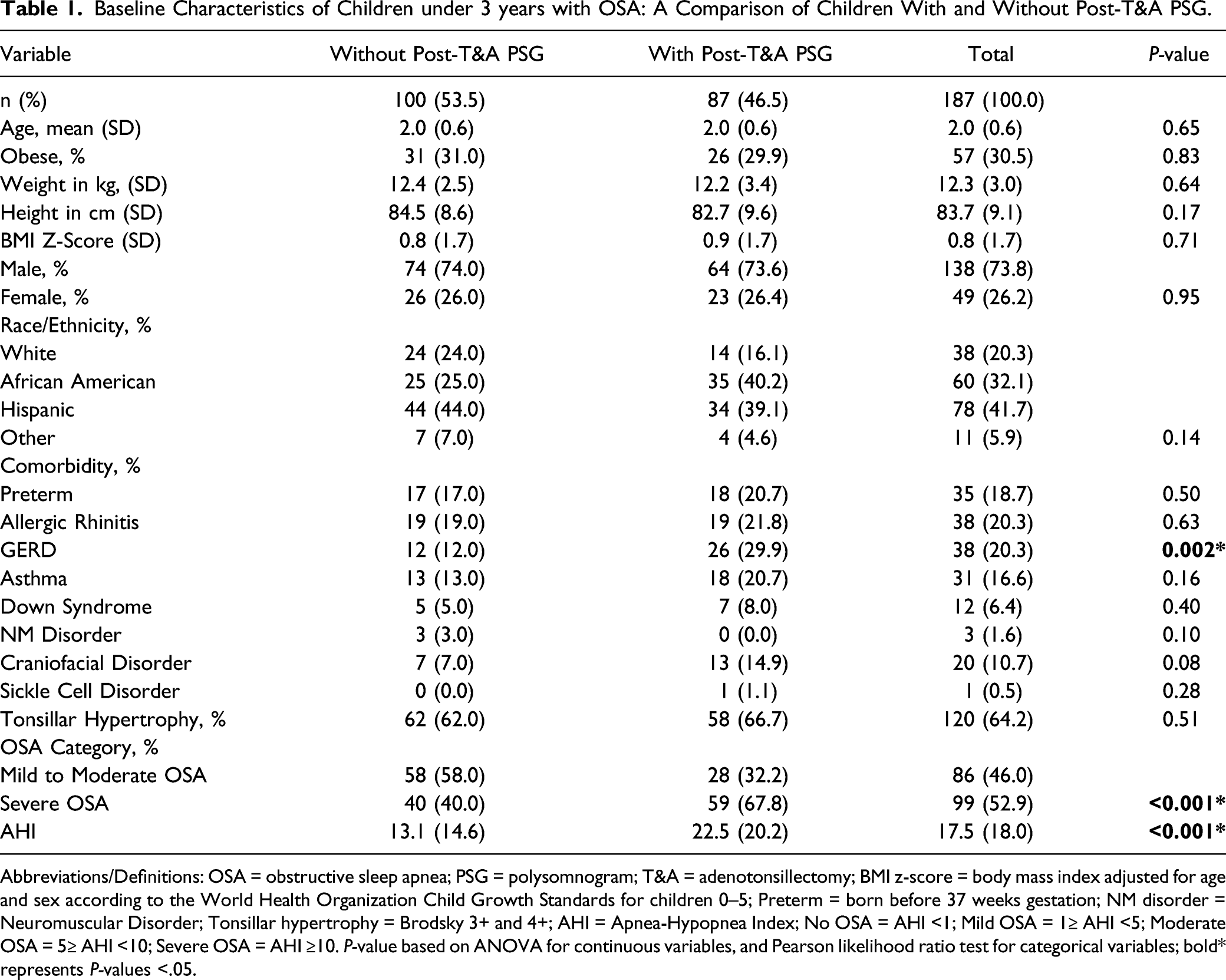
Abbreviations/Definitions: OSA = obstructive sleep apnea; PSG = polysomnogram; T&A = adenotonsillectomy; BMI z-score = body mass index adjusted for age and sex according to the World Health Organization Child Growth Standards for children 0–5; Preterm = born before 37 weeks gestation; NM disorder = Neuromuscular Disorder; Tonsillar hypertrophy = Brodsky 3+ and 4+; AHI = Apnea-Hypopnea Index; No OSA = AHI <1; Mild OSA = 1≥ AHI <5; Moderate OSA = 5≥ AHI <10; Severe OSA = AHI ≥10. P-value based on ANOVA for continuous variables, and Pearson likelihood ratio test for categorical variables; bold* represents P-values <.05.
Polysomnographic Parameters in Children under 3 years old With Obstructive Sleep Apnea Pre- and Post-Adenotonsillectomy.
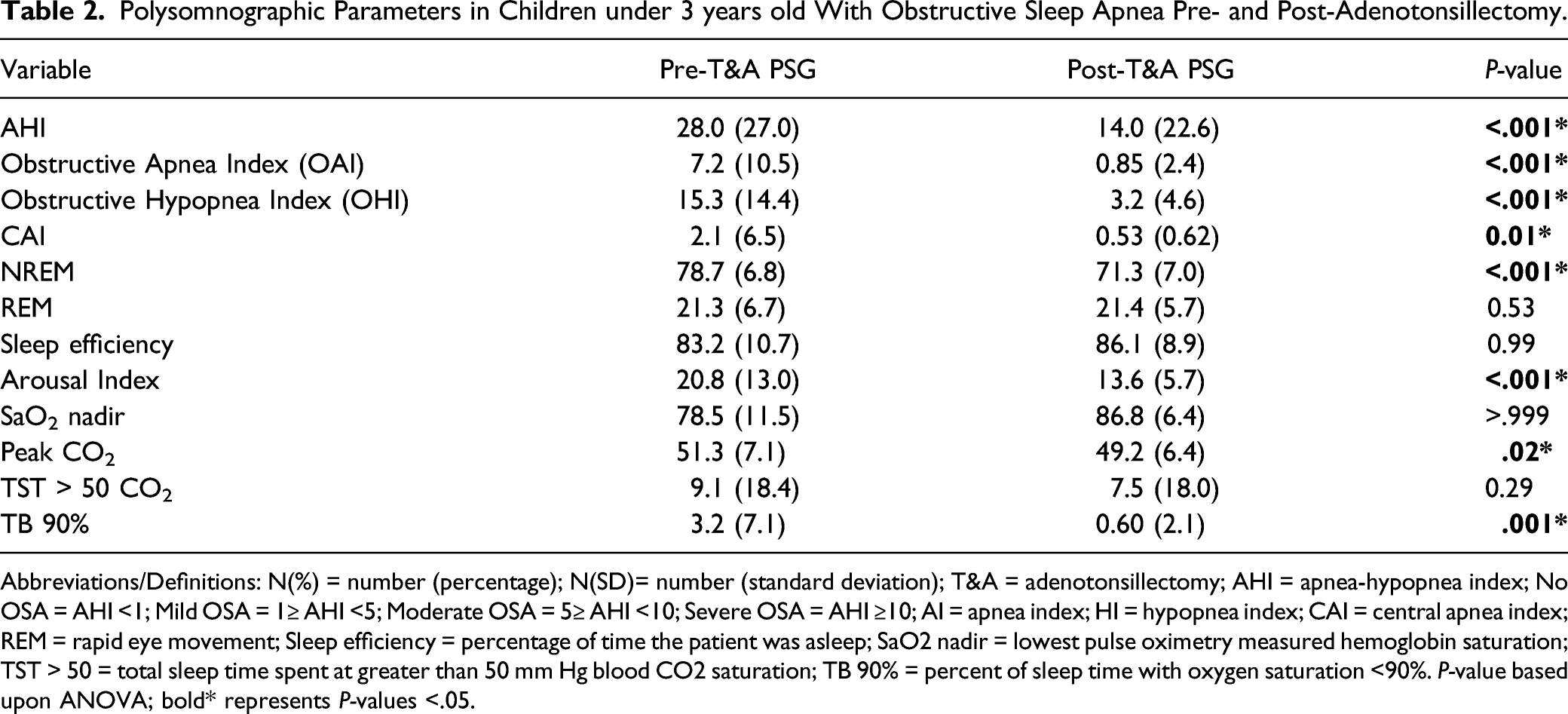
Abbreviations/Definitions: N(%) = number (percentage); N(SD)= number (standard deviation); T&A = adenotonsillectomy; AHI = apnea-hypopnea index; No OSA = AHI <1; Mild OSA = 1≥ AHI <5; Moderate OSA = 5≥ AHI <10; Severe OSA = AHI ≥10; AI = apnea index; HI = hypopnea index; CAI = central apnea index; REM = rapid eye movement; Sleep efficiency = percentage of time the patient was asleep; SaO2 nadir = lowest pulse oximetry measured hemoglobin saturation; TST > 50 = total sleep time spent at greater than 50 mm Hg blood CO2 saturation; TB 90% = percent of sleep time with oxygen saturation <90%. P-value based upon ANOVA; bold* represents P-values <.05.
Most children (78%) had persistent post-operative OSA (AHI ≥1), including all 7 children with DS. Those with, versus without, moderate to severe OSA post-T&A (AHI ≥5) were more likely to have GERD (50% versus 24%, P = .025), a craniofacial disorder (30% versus 10%, P = .025), or DS (20% versus 5%, P = .031). Of children with AHI ≥5 after T&A, 75% had severe OSA before T&A, with a pre-T&A mean AHI of 23.4. Those with, versus without, severe OSA (AHI ≥10 versus AHI <10) post-T&A were more likely to have DS (29% versus 6%, P = .04). Of the 7 children with severe OSA after T&A, 5 had severe pre-operative OSA, with a pre-T&A average AHI of 36.
Figure 1 presents the outcomes of T&A for OSA based on post-T&A AHI. Nineteen children had resolution of OSA after T&A (AHI <1), 82 (94%) had an improvement in AHI, and 5(6%) had worsening of AHI. The average increase in AHI for these 5 children was 3.5 (0.4, 2.0, 2.2, 3.4, and 9.4), with one increasing from 4.7 to 14.1 after T&A. Sixty-nine children (79%) improved in OSA severity category, 15 (17%) remained in the same category, and 3 (3%) had a worsening in their OSA severity category post-T&A. For the 59 children with pre-T&A severe OSA, 12 (20%) had no OSA, 32 (54%) had mild OSA, 10 (17%) had moderate OSA, and 5 (8%) had severe OSA after surgery. Changes in Outcomes by Severity after Adenotonsillectomy (T&A) for Obstructive Sleep Apnea in Children under 3 years. Abbreviations/Definitions: PSG = polysomnogram; OSA = obstructive sleep apnea; T&A = adenotonsillectomy. No OSA = AHI <1; Mild OSA = 1≥ AHI <5; Moderate OSA = 5≥ AHI <10; Severe OSA = AHI ≥10.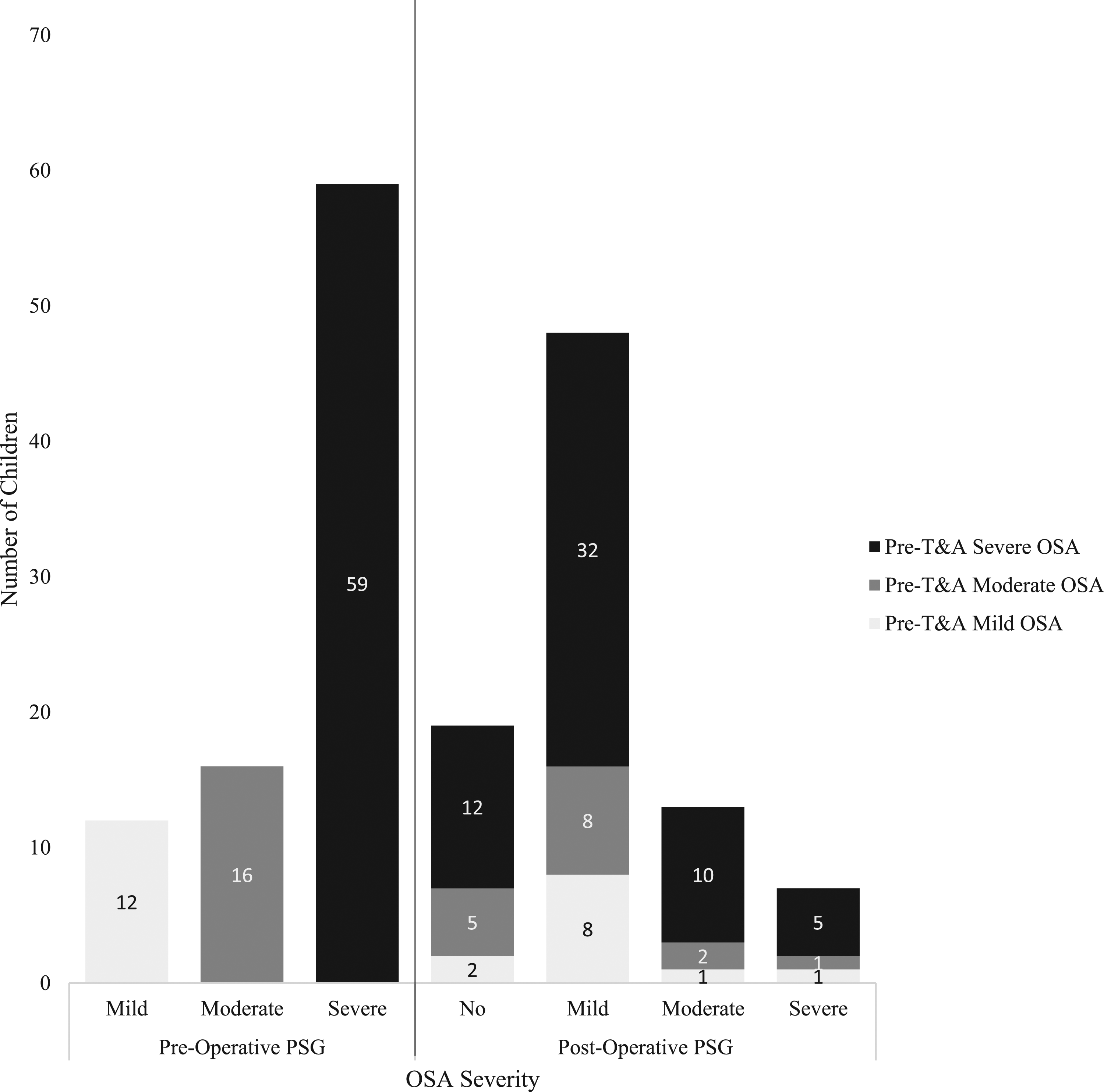
Multiple Logistic Regression of Predictors of Persistent Severe Obstructive Sleep Apnea (OSA) Among Children Less Than 3 Years of Age.
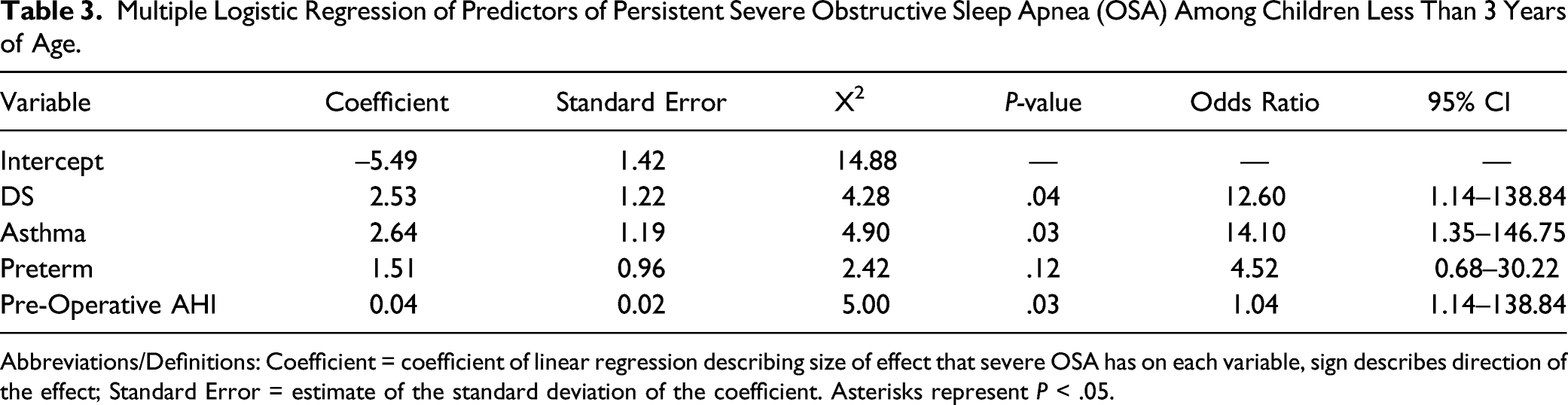
Abbreviations/Definitions: Coefficient = coefficient of linear regression describing size of effect that severe OSA has on each variable, sign describes direction of the effect; Standard Error = estimate of the standard deviation of the coefficient. Asterisks represent P < .05.
Discussion
This study evaluated the outcomes of T&A in children under 3 years of age with OSA. A previous study of children under 3 years of age with OSA reported that these children commonly had a history of prematurity or GERD, and approximately 35% had severe OSA. 11 This is a follow-up study to evaluate for resolution of OSA after T&A and to identify predictors of persistent OSA. By evaluating for resolution of OSA after T&A and predictors of persistent OSA, this study addresses a knowledge gap highlighted in the updated Clinical Practice Guidelines for Tonsillectomy in Children. 12 Children with post-T&A PSG, compared to children excluded for not having post-operative PSG, were more likely to have GERD, a higher pre-operative AHI, and severe OSA but were otherwise similar in demographics and comorbidities. Most children had an improved AHI (94%), but 78% had persistent OSA post-operatively. Nearly a quarter had moderate to severe OSA after T&A and these children were more likely to have GERD, a craniofacial disorder, or DS compared to those with mild persistent OSA. Severe OSA pre-operatively is also a major indicator for persistent OSA after T&A (72%). While there was a significant improvement in CAI, this may be due to latent obstructions being read as central apneas and subsequently improving with T&A. Additionally, six children had post-T&A complications, but this relatively small number precluded further evaluation or comparison.
Our study population predominantly included Black/African Americans (40%) and Hispanics (39%), followed by White/Caucasians (16%) and “others” (5%). Our previous study reported a similar distribution of Hispanic (41%), Black/African American (28%), White/Caucasians (25%), and “others” (7%). 11 Most other previous studies on persistent OSA after T&A either did not report on race/ethnicity or had less diversity. Tauman et al. 19 reported a White to Black ratio of 3:2 and Nath et al. 8 reported a predominantly Black population (85%). This study is unique in having a large ethnically diverse population.
Most children had improved respiratory parameters post-operatively. Overall, 92% improved in OSA severity category. All with severe OSA improved in AHI after T&A (mean AHI 28 to 14). Similarly, Brigance et al. 5 reported that the mean decrease in AHI was 9.6. Nath et al. 8 and Mitchell et al. 9 reported more dramatic improvements (34.8 to 5.7 and 34.1 to 12.2, respectively). Additionally, studies of children older than 3 years report similar improvements in AHI after T&A.19,20
While most children improved, 78% had persistent post-operative OSA. No predictors of persistent OSA were found. However, all children with DS had persistent OSA, perhaps due to associated oro- and nasopharyngeal narrowing, macroglossia, and hypotonia in this syndrome. 21 Persistence of moderate to severe OSA is considered an indication for positive airway pressure therapy, and the percentage of these children in our study (23%) is similar to other studies in children under 3 years.8,9 Children with persistent moderate to severe OSA were more likely to have DS, GERD, or a craniofacial disorder. The association between GERD and persistence of moderate to severe OSA in children under 3 years, to our knowledge, has not been previously reported. In our previous study, we reported that 25% of children had GERD. 11 Jung et al. 22 reported 60% of patients with OSA have GERD perhaps due to increased transdiaphragmatic pressure, decreased intra-thoracic pressure, transient lower esophageal sphincter relaxation, and increased pressure across the lower esophageal gradient. 22 However, OSA may predispose to GERD rather than vice versa, which requires further research. Persistence of moderate to severe OSA in children with craniofacial abnormalities is explained by anatomic factors, such as poor motor tone, maxillary or mandibular hypoplasia, inferiorly placed hyoid bone, or other differences that narrow the upper airway.23,24
Children with persistent moderate to severe OSA were also more likely to have pre-operative severe OSA. We have previously reported that approximately 35% of children under 3 years of age have severe OSA. 11 Similarly, Nath et al. 8 reported that the severity of pre-operative OSA was a predictor of persistent moderate to severe OSA in those under 3 years. Other studies found that high pre-operative AHI was a risk factor for persistent moderate to severe OSA in older children.19,20 Overall, children under 3 years with DS, GERD, a craniofacial disorder, and/or severe OSA are at high risk of persistent OSA and may benefit from routine post-T&A PSG.
This was a retrospective study of over 80 children under 3 years of age with OSA who underwent T&A with pre- and post-operative PSG at a tertiary care children’s hospital. However, some limitations should be recognized. First, this study was conducted at a single institution with a racial/ethnic breakdown that may not reflect the general pediatric population or those under 3 years old with OSA in the community. It also has a selection bias as all children were referred for PSG for suspected OSA. Also, children that had more severe OSA were more likely to undergo post-T&A PSG and included in the study. Some data may be inaccurate or incomplete, and the study lacks a control population of children who did not undergo T&A. Furthermore, this study did not comprehensively evaluate post-operative complications, safety of T&A, or long-term outcomes in children under 3 years with OSA. Nonetheless, it has many strengths including the large diverse patient population, use of electronic medical records, and availability of PSG in all children.
Conclusions
In this ethnically diverse population, children under 3 years with OSA had marked improvements in OSA severity after T&A, though few normalized their sleep disorder. Children with persistent moderate to severe OSA were more likely to have DS, craniofacial abnormalities, GERD, or pre-operative severe OSA, and children with these comorbidities may benefit from post-operative PSG to evaluate for persistent OSA. Overall, we recommend T&A in children under 3 years with OSA. Further study is needed on post-operative complications and long-term outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.