
Abstract
Introduction
Hypopharynx squamous cell carcinoma (HPSCC) is one of the most frequent head and neck cancers and is considered to occur frequently after 40 years.1,2 Standard treatment for hypopharynx SCC is dependent on the stage. Early stages can be treated with either surgery or radiotherapy; while locally advanced hypopharynx cancer can be treated with surgery followed by postoperative radiotherapy or with concurrent chemoradiotherapy.3-5
A lack of understanding of the disease results in more aggressive tumors and brings great difficulties to the treatment. The common metastatic sites of HPSCC are the lung, bone, and liver, with the lung being the most common site.5-9 Predicting the development of lung metastases (LM) may contribute to improvements in both decision-making in terms of adjuvant chemotherapy and survival. However, seldom studies looked into the patients with high risk. Therefore, the objective of this study was to analyze the risk factors and prognosis of LM in a large cohort of patients with HPSCC.
Materials and Methods
Cohort Population
The Surveillance, Epidemiology, and End Results (SEER) database (http://www.seer.cancer.gov/seerstat) consists of 18 population-based cancer registries that cover approximately 28% of the US population and is freely available for cancer-based epidemiology investigation and survival analysis. We included patients diagnosed with microscopically confirmed HPSCC between January 1, 2010 and December 31, 2013 because of information on the presence or absence of metastases at the time of diagnosis in 2010 in the SEER database. The inclusion criteria for selection data in this study were as follows: (1) AJCC (7th edition) stage; (2) diagnosis confirmed by positive histology; and (3) only one primary tumor. The exclusion criteria included the following: (1) data, such as race, gender, age, T classification and N classification, incomplete and (2) diagnosis before 2010. The distributions of categorical demographic and clinicopathological variables were determined for different age groups (31-49, 50-59, 60-69, 70-79, and 80-95 years). The SERR database only had metastatic information related to bone, brain, lung, and liver metastases.
Statistical Analysis
Log-rank test and the Cox proportional hazard models were used to determine the risk factors. All statistical analyses were made using IBM SPSS (Statistical Product and Service Solutions) 24.0. P values were two-sided and P < .05 were considered significant.
Results
Analysis of Information on All Patients
Data for a total of 1683 patients, including 70 patients (4.2%) with synchronous LM and 1613 patients without synchronous LM (95.8%), were investigated. The median age was 64 years (range, 31-95 years). LM is related to gender (P = .011), race (P = .015), grade (P = .002), T classification (P = .006), N classification (P = .000) (Table 1).
Demographic Characteristics of Patients With and Without Lung Metastases.
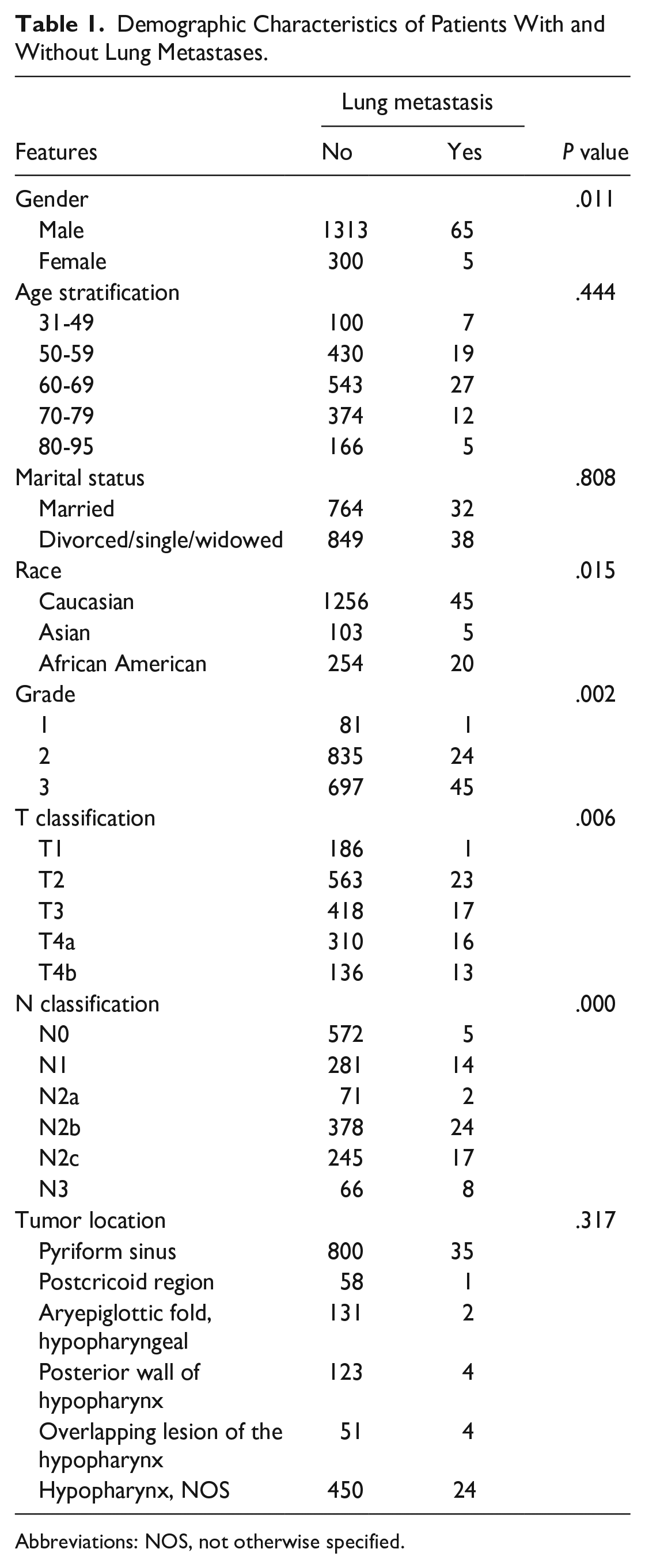
Abbreviations: NOS, not otherwise specified.
Identification of High-Risk Factors for Lung Metastasis
Univariate analysis results suggest that Caucasian females who harbored lower T or N classification, highly differentiated disease were associated with a significantly lower risk of LM. The single-factor significant factors were included in the multivariate logistic regression and the results showed that Caucasian (P = .038) who harbored lower T (P = .026) or N classification (P = .000), highly differentiated disease (P = .002) were associated with a significantly lower risk of LM (Table 2).
Univariate Logistic Regression and Multivariate Logistic Regression Analysis of Risk Factors for Lung Metastasis.
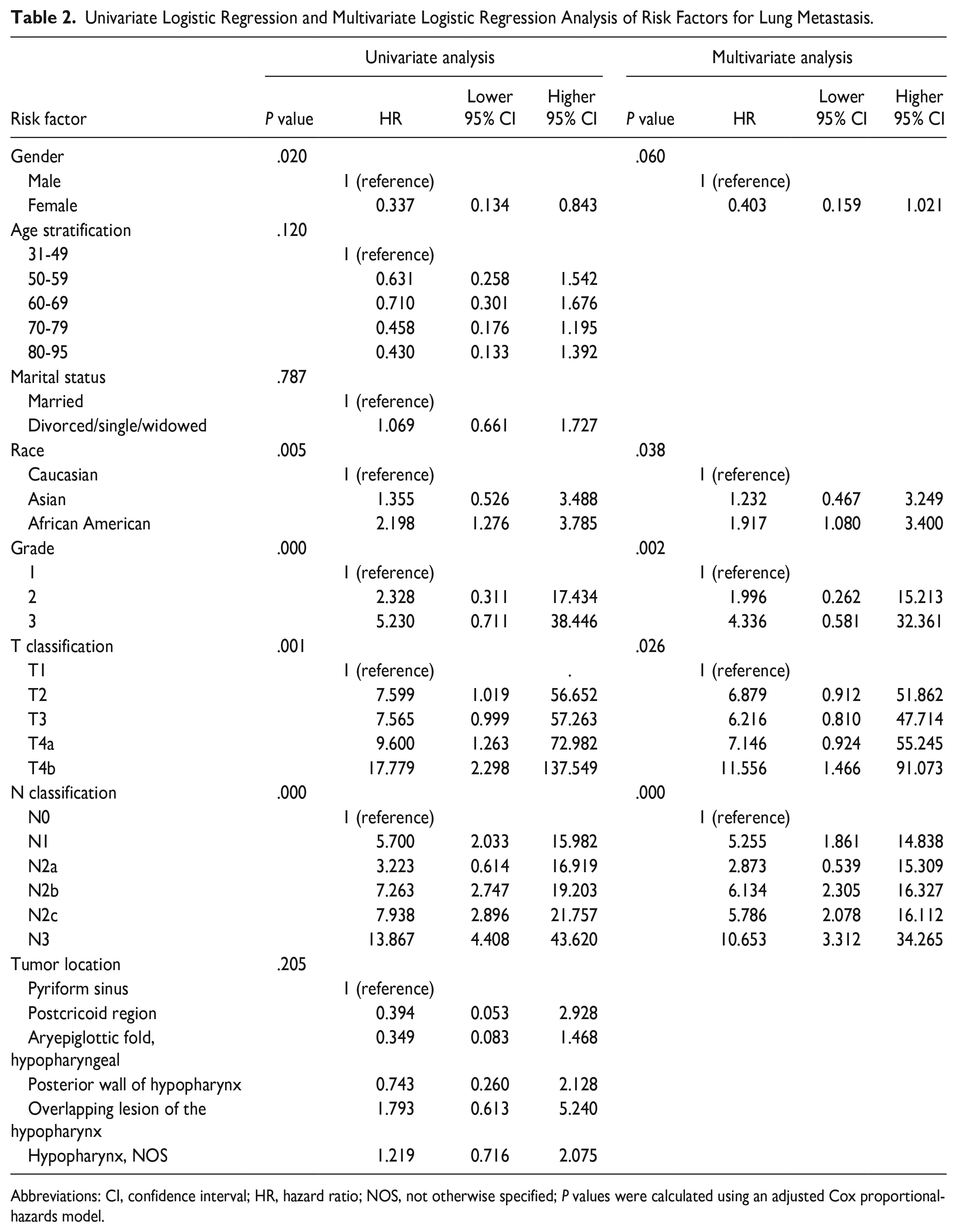
Abbreviations: CI, confidence interval; HR, hazard ratio; NOS, not otherwise specified; P values were calculated using an adjusted Cox proportional-hazards model.
Survival
The median follow-up time was 13.0 months (range, 0-59 months). Univariate analysis revealed that age, marital status, race, tumor location, T classification, N classification, surgery therapy, and distant metastases significantly affected the Overall Survival (OS) and Cancer-Specific Survival (CSS) (Table 3).
Univariate Logistic Regression and Multivariate Logistic Regression Analysis of Overall Survival.
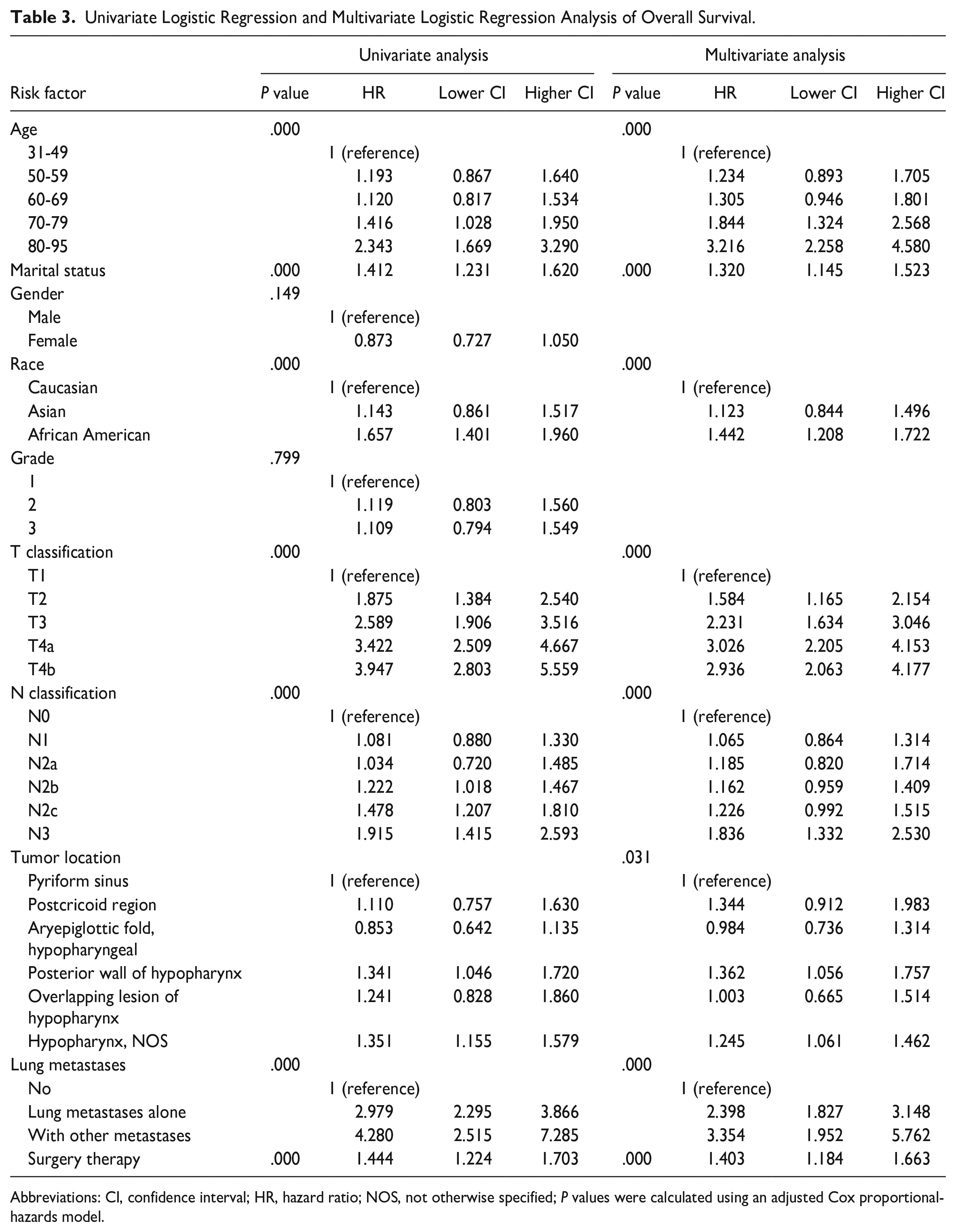
Abbreviations: CI, confidence interval; HR, hazard ratio; NOS, not otherwise specified; P values were calculated using an adjusted Cox proportional-hazards model.
The single-factor significant factors were selected in the multivariate model. Age (P = .000), marital status (P = .000), race (P = .003), tumor location (P = .046), T classification (P = .000), N classification (P = .000), distant metastases (P = .000), and surgery therapy (P = .001) significantly affected the CSS (Table 4). Elderly not married patients with advanced T or N classification, no surgical therapy to the primary tumors, and multiple sites of metastases were more likely to reduce life expectancy.
Univariate Logistic Regression and Multivariate Logistic Regression Analysis of Cancer-Specific Survival.
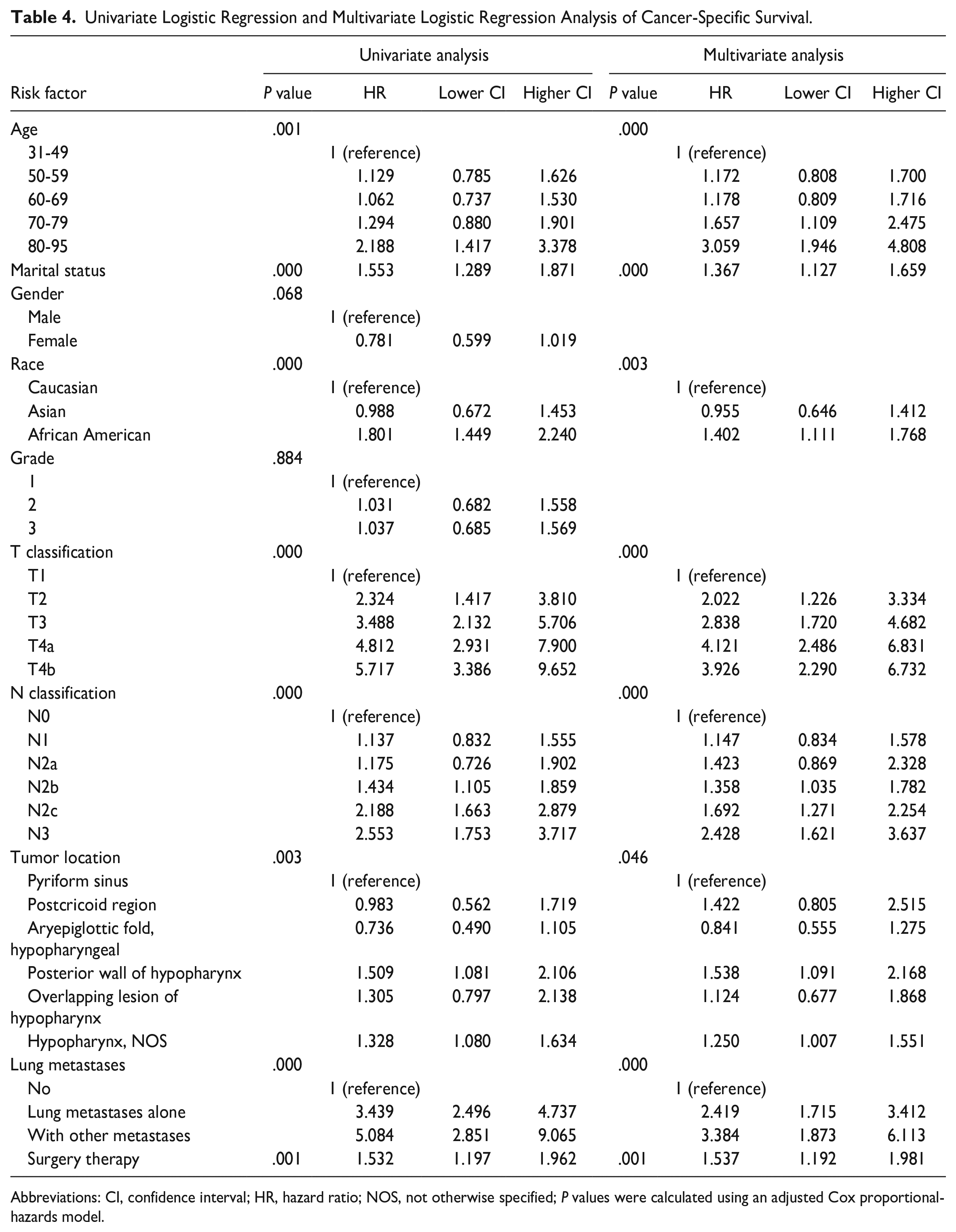
Abbreviations: CI, confidence interval; HR, hazard ratio; NOS, not otherwise specified; P values were calculated using an adjusted Cox proportional-hazards model.
The 1-year overall survival rates of patients with non-lung metastasis, lung metastasis alone, and with other metastases were 68.32%, 30.31%, and 11.03%, the 2-year survival rates were 50.67%, 12.03%, and 11.03%. The survival rate of the group with LM alone and LM with other metastases groups was significantly lower than that of the non-metastatic group. The overall survival rate difference between the three groups was statistically significant (P < .001, Figure 1). We observed the same pattern of associations for CSS.
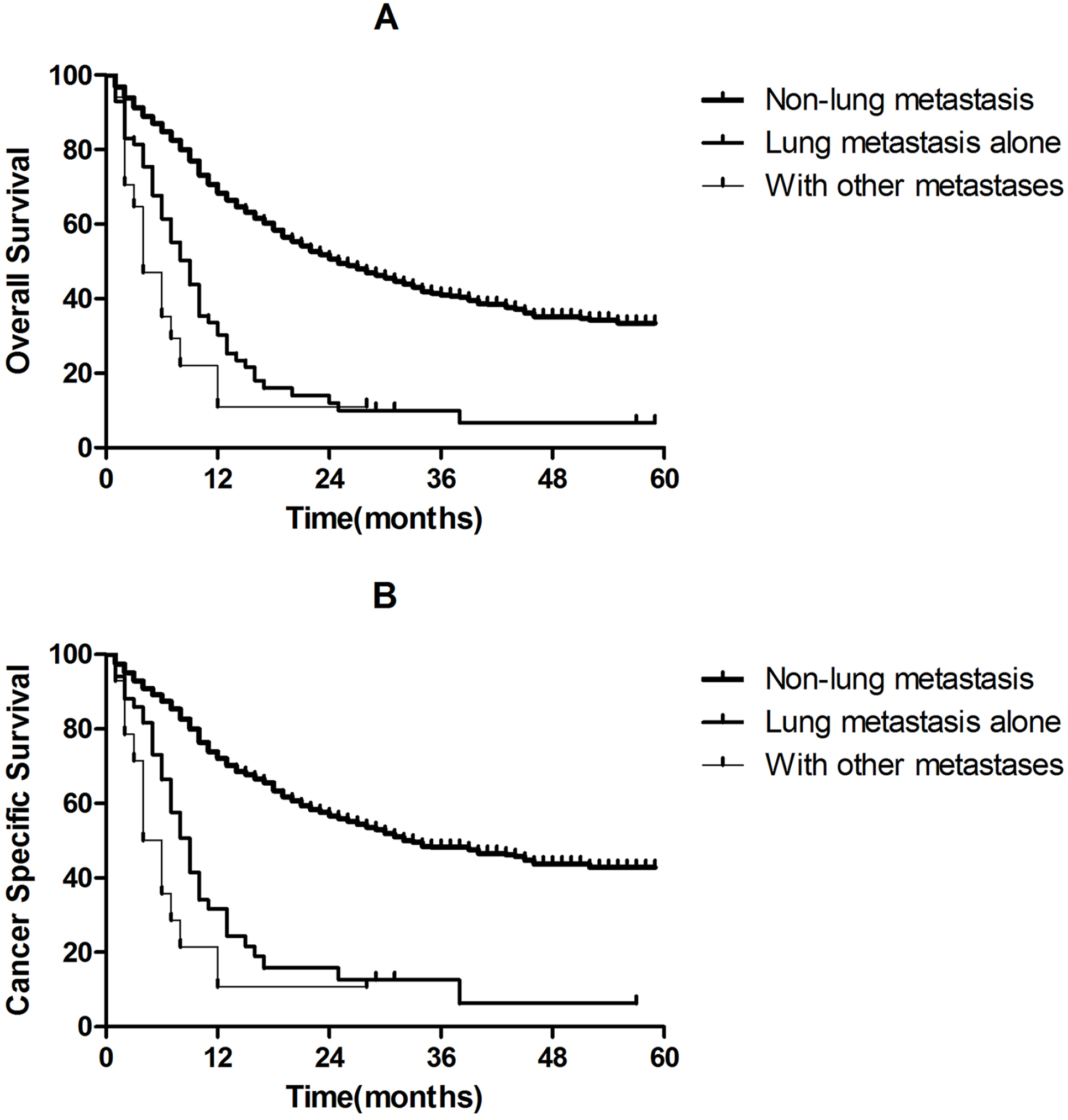
Kaplan-Meier analysis of overall survival and cancer-specific survival in lung metastasis and non-lung metastasis hypopharynx squamous cell carcinomas (HPSCC) patients. (A) Overall survival in non-lung metastasis, lung metastasis alone, and with other metastases HPSCC patients (P < .001). (B) Cancer-specific survival in non-lung metastasis, lung metastasis alone, and with other metastases HPSCC patients (P < .001).
Discussion
Due to the improved locoregional control and the increasing number of head and neck squamous cell carcinoma (HNSCC) survivors in the last decades, data on LM development gained more importance, recently. 10 On the other hand, recognizing patients with a high chance of developing LM is essential, as these patients need to be screened before they undergo intensive treatment while costly imaging modalities can be spared in their counterparts who do not likely develop LM. In this study, we revealed that the niches of distant metastasis (DM) were predominantly located in the lungs and bones, in accordance with the literature.5-9 Higher T classifications increased the risk of LM and advanced regional diseases (N2 or N3 disease) are found in patients with a high risk of LM disease. Liu analyzed the NCDB (National Cancer Database) and found that patients with locally advanced tumors (T3-T4) had higher rates of metastasis than those with T1 tumors in the multivariate analysis (P = .064 in T3 vs T1; P < .001 in T4 vs T1) and N+ was an independent risk factor for DM in the multivariate analysis (P < .001, respectively). 11 In van der Kamp MF’s study, multivariable analysis identified advanced T-classification (HR = 1.61, 95% CI 1.09–2.38), regional lymph node metastasis (HR = 5.35, 95% CI 3.25–8.79), and extranodal extension of regional lymph nodes metastasis (HR = 3.06, 95% CI 1.39–6.72) as independent prognostic factors for the presence or development of DM, which was similar to our study. 12
For HPSCC, the effect of race on LM in HPSCC remains unclear and few studies have specifically studied a prognostic value of race on LM in patients with HPSCC. Our findings suggest that Caucasians were significantly associated with a lower risk of LM. Al-Othman found that the difference of black patients had a higher risk of distant metastases compared with white patients (27% vs 13%; P = .012) but the 5-year local-regional control rates of the two groups were similar (P = .275). 13 Gourin found that black patients had a higher incidence of stage IV disease and non-operative treatment (P < .0001, respectively). In addition, black patients resided in block groups with significantly lower income and education levels indicate that racial differences are primarily related to healthcare differences. 14
In addition, tumor grade is another risk factor affecting LM, and poorer differentiation was associated with a higher incidence of LM in multivariate logistic regression analysis. A few studies have found that grade 3 disease yields a higher risk of distant metastases.9,11 Van der Kamp MF found that poor differentiation grade was also found to be a significant independent predictor of DM. 12 These factors were also described as high-risk factors for DM in a review on DM in HNSCC. 10 However, Alvi found that in stage III and IV squamous cell carcinoma patients, histological grades were not associated with a higher risk for DM (P > 0.05, respectively). 15 These conflicting results may originate from the heterogeneity of the patients’ cohorts.
A few of the variables influencing the OS and CSS of HPSCC have been described previously (Table 4). In our study, Caucasians were associated with a better prognosis and several studies have shown that patients’ age is one of the prognostic factors in head and neck carcinoma including HPSCC in terms of age.4,5,16,17 As for race, Al-Othman 13 found that race was an independent predictor of freedom from absolute survival and cause-specific survival (P < .005, respectively) in multivariate analyses, which was similar to our study.
Furthermore, early diagnosis and treatment are particularly important for therapeutic planning; we observed that the survival rate of the group with LM alone and LM with other metastases group was significantly lower than that of the non-metastatic group (Figure 1). There are few effective therapies for LM of HPSCC and prognosis of metastatic HPSCC is always dismal. Predicting the development of LM may contribute to improvements. We conclude that a chest computed tomography (CT) scan would be an effective study and positron emission tomography/CT would be most effective in patients with higher risk of DM, such as advanced T and N classification hypopharynx cases.
The greatest strength of this study is the population-based nature of the study and the large sample size, which gives insight into how US doctors identify high risk of LM in HPSCC patients. However, there are some limitations in our study. It was a retrospective analysis based purely on the SEER database and important medical information, including performance status, positive surgical margins, alternative treatment, and comorbidities, is not available, which prevented us from adjusting our analyses for these important factors. Independent validation study is needed to confirm the findings in the future.
Conclusion
In our study, about 4.2% of HPSCC patients with synchronous LM at initial diagnosis and Caucasian, lower T or N classification, highly differentiated disease were associated with a significantly lower risk of LM. Elderly not married patients with advanced T or N classification, no surgical therapy to the primary tumors, and multiple sites of metastases were more likely to reduce life expectancy. More accurate assessments of LM will be imperative for early diagnosis and treatment in non-Caucasian patients who harbored higher T or N classification and poorly differentiated disease.
Footnotes
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Shanghai Municipal Health Commission (grant numbers: 20214Y0025).
The study was funded by the Shanghai Pudong New Area Heath Commission (grant numbers: PW2022A-41).
Ethical Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
Consent for Publication
Not applicable.