
Abstract
Introduction
It is a common understanding that social support, especially spousal support, plays an important role in improving cancer outcomes.1-6 In addition, many researches in recent years have demonstrated that marital status could independently affect survival in several cancer types.7-9 However, further analysis of marital subgroups was neglected, which might reveal the potential mechanism generating the influence of marital status on prognosis.
Hypopharynx squamous cell carcinoma (SCC) is one of the most frequent head and neck cancers (HNSCC), and is considered to occur frequently after 40 years of age.10,11 About 2500 to 3000 cases of hypopharyngeal cancer (HC) are diagnosed annually in the United States, with a 5 year overall survival (OS) of only 30% to 33%.12-14 Multiple primary SCC of the head and neck is increasing in frequency, especially in the hypopharynx and esophagus.15-19 According to the Surveillance Epidemiology and End Results (SEER) database, the percentage of cases diagnosed in a localized stage decreased from 23.0% to 9.3% during 1974 to 1999; disease with distant-stage decreased from 25.7% to 18.6%.12-14 Compared with the dismal 5 year OS of one-third for HC, localized disease has a survival rate of 56.0%.12-14 Human papilloma virus (HPV)-associated head and neck carcinoma is quite heterogeneous and most of the tumors arise in the oral cavity, oropharynx, hypopharynx, and larynx.20-25 In addition to HPV exposure, tobacco and alcohol are very strongly associated with the development of HC.26-28 The efficacy of the current HPV vaccines, Cervarix and Gardasil, in preventing HPV-related HNSCC is at present unknown. Any reduction in tobacco or alcohol intake would be an effective strategy to mitigate HC risk, as well as the risk of few other neoplasms. 29
Understanding the interaction between marital status and gender, race, and age is important for developing tailored interventions aimed at improving socio-emotional support for patients. Therefore, the objective of this study is to explore the correlation between marital status and hypopharynx SCC and whether the association varied by age, race, and gender using the SEER database.
Materials and Methods
Patient and Public Involvement
This research was done without patient and public involvement. Patients were not invited to comment on the study design. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Cohort Population
We obtained data from the current SEER database, which consists of 18 population-based cancer registries. This database collects and publishes cancer prevalence and survival data covering approximately 28% of the total population in the United States. SEER*Stat Version 8.3.4 (http://www.seer.cancer.gov/seerstat) from the National Cancer Institute was used to identify eligible patients in this study. Because the SEER database began collecting information on the presence or absence of metastases at the time of diagnosis in 2010, we included patients diagnosed with microscopically confirmed hypopharynx SCC between January 1, 2010, and December 31, 2014. We selected patients with only one primary malignancy in their lifetime. We excluded patients for whom the aforementioned data were missing. A total of 1686 hypopharynx SCC patients were included.
Statistical Analysis
Descriptive statistics were performed to investigate patients’ baseline characteristics and clinical characteristics were compared between different categories of marital status using the chi-squared test. The primary study outcomes were OS (time to the date of death due to any cause or the date of last follow-up) and cancer-specific survival (CSS: time from initial treatment to death due to cancer). Kaplan-Meier curves and the log-rank tests were used to evaluate the OS and CSS rates among different categories of marital status. Multivariate Cox proportional analyses were used to assess the influence of marital status on OS and CSS. A 2-sided P value of <.05 was considered as statistically significant. All statistical analyses were performed using SPSS Software, Version 22.0 (SPSS).
Results
Clinical Characteristics of all Patients
The median age was 64 years (range: 31-95 years) and more than half of the patients (1381/1686, 81.9%) were males. A total of 797 (47.3%), 293 (17.4%), 415 (24.6%), and 181 (10.7%) patients were married/partnered, divorced/separated, never married, and widowed, respectively. Married/partnered patients received more surgeries. The rate of being married was higher among Asian or Caucasian, and this rate decreased with higher tumor stage. Black patients, as well as patients younger than 50 years, showed the highest rate of being single (Table 1).
Demographic Characteristics of Hypopharynx SCC Patients Who Were Stratified by Marital Status.
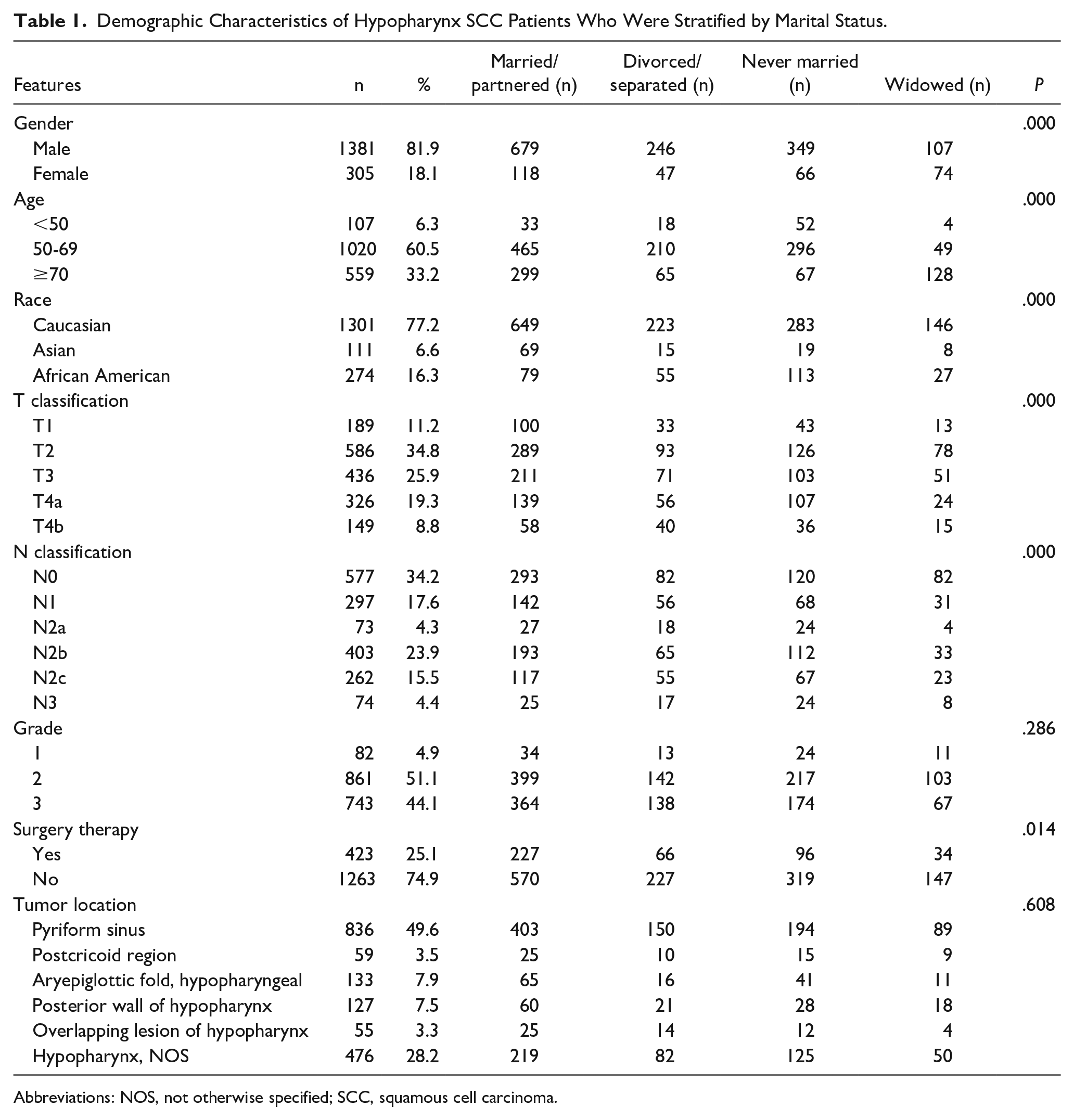
Abbreviations: NOS, not otherwise specified; SCC, squamous cell carcinoma.
Survival
Median follow-up was 13.0 months (range: 0-59 months). Univariate analysis showed that age, tumor location, marital status, grade, T category, N category, distant metastases, and surgery therapies to the primary tumor were significantly associated with OS and CSS (P < .01). Married subgroup showed significantly better OS and CSS than the unmarried groups (P < .05), while there was no significant difference of OS and CSS between the never married and the widowed groups (Figure 1).
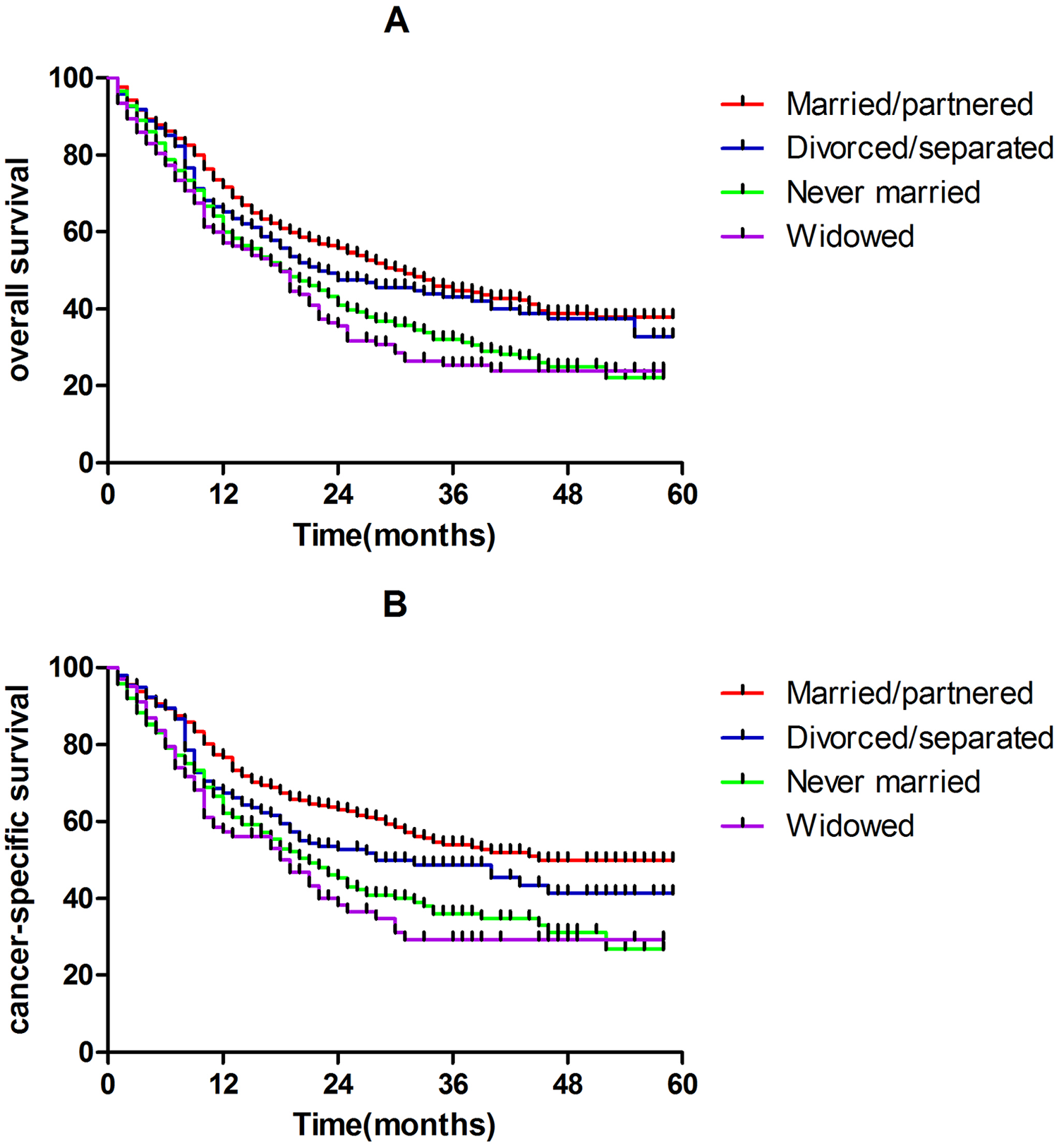
Kaplan-Meier analysis of OS (A) and CSS (B) for hypopharynx SCC stratified by marital status. OS, overall survival; CSS, cancer-specific survival; SCC, squamous cell carcinoma.
Age, tumor location, marital status, grade, T category, N category, distant metastases, and surgery therapies to the primary tumor were selected in the multivariate model, which were independent prognostic factors in the multivariable analysis (Table 2). Compared to married/partnered patients, the hazard ratios (HRs) for divorced/separated, never married, and widowed patients were 1.164 [95% confidence interval (CI): 0.952-1.422], 1.452 (95% CI: 1.216-1.733), and 1.461 (95% CI: 1.173-1.820), respectively. The same results were found in CSS.
Multivariable Logistic Regression for OS and CSS in the SEER Cohort.
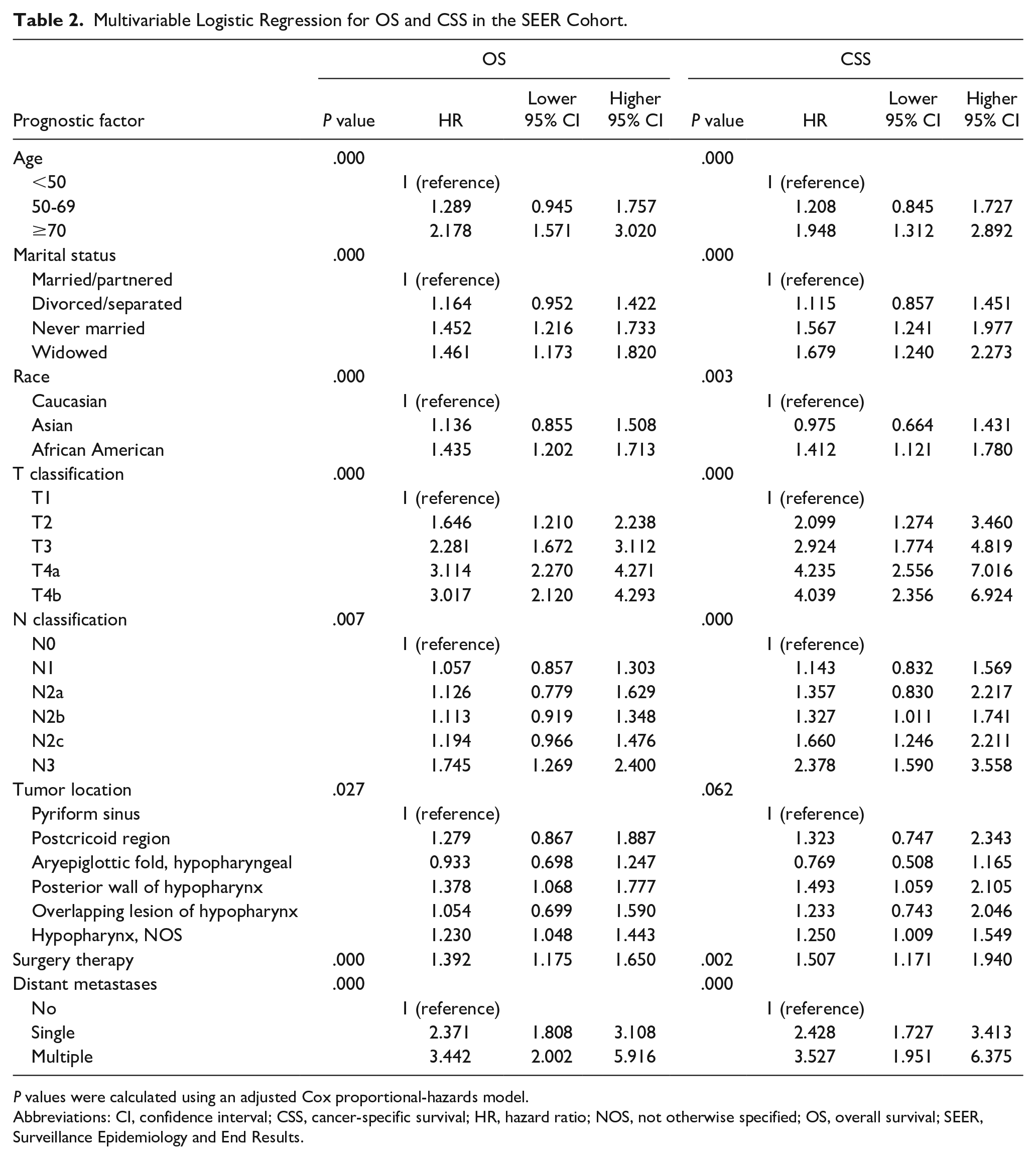
P values were calculated using an adjusted Cox proportional-hazards model.
Abbreviations: CI, confidence interval; CSS, cancer-specific survival; HR, hazard ratio; NOS, not otherwise specified; OS, overall survival; SEER, Surveillance Epidemiology and End Results.
Effects of Marital Status Stratified by Subgroups
To rule out the effects of these variables and further validate the effect of marital status on OS and CSS, we conducted the subgroup analysis based on these variables (Table 3). While marriage was associated with better survival for both married male and female, subgroups analysis shows a differential in OS based on gender, with males benefiting more than females. Patients who were divorced/separated (male HR = 1.214, 95% CI: 0.985-1.495; female HR = 1. 159, 95% CI: 0.691-1.945), never married (male HR = 1.476, 95% CI: 1.234-1.765; female HR = 1.422, 95% CI: 0.901-2.245), and widowed (male HR = 1.795, 95% CI: 1.390-2.317; female HR = 1.663, 95% CI: 1.081-2.559) had increased hazard of OS compared with married/partnered patients. Remarkably, the protective effect of marriage was consistent in all age groups. Better OS of the married patients was found only in Caucasian patients who harbored well/moderately differentiated and nonmetastatic disease (P < .001). The proportion of postcricoid region, aryepiglottic fold, and overlapping lesion of hypopharynx was obviously lower, in which the protective effect of being married did not occur.
The Effect of Marital Status on Overall Survival Based on Different Subgroup Variables.
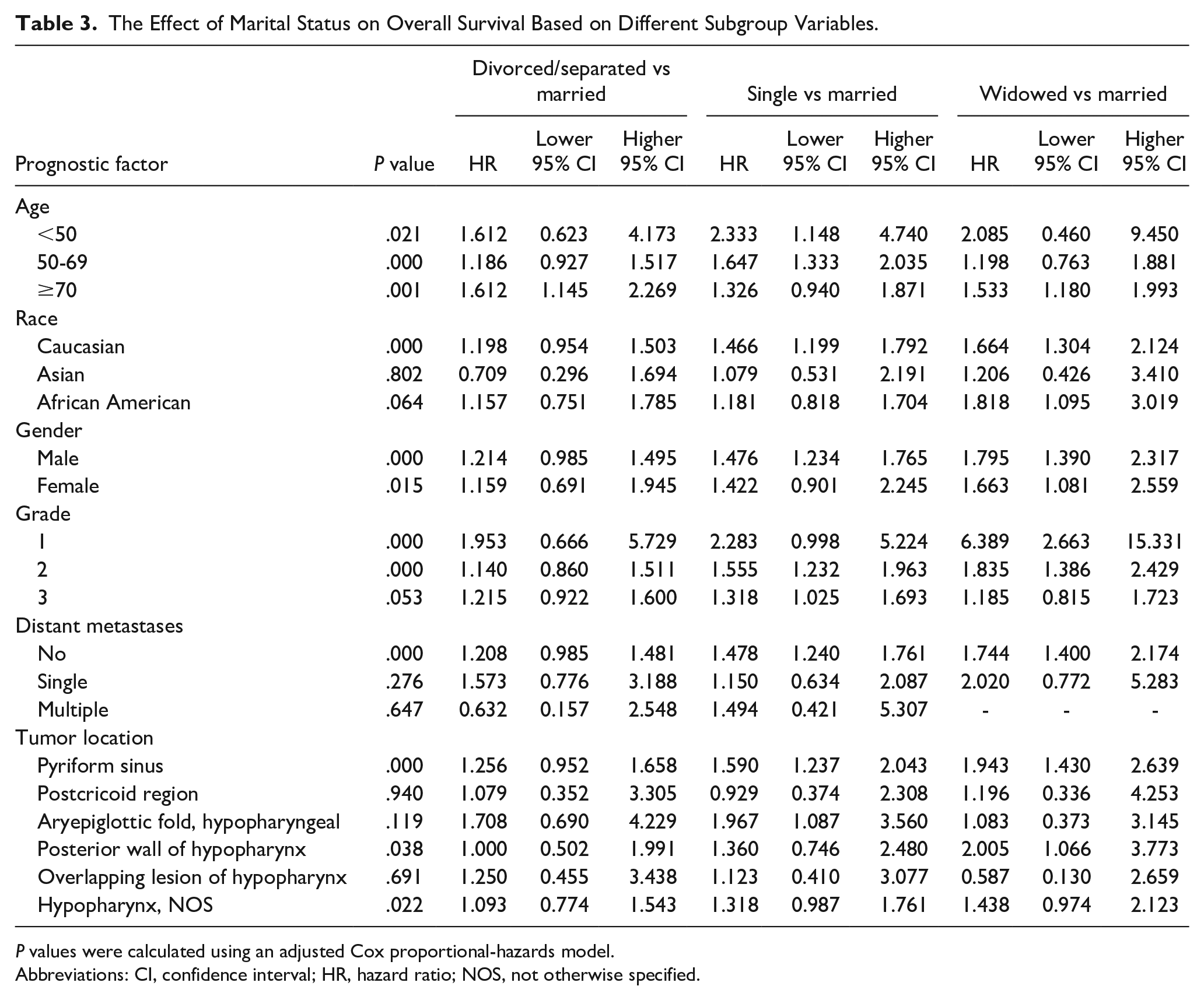
P values were calculated using an adjusted Cox proportional-hazards model.
Abbreviations: CI, confidence interval; HR, hazard ratio; NOS, not otherwise specified.
Discussion
In this study, we confirmed what previous studies had shown, that is, marital status affected OS of hypopharynx SCC patients. Social support can also lead to the pursuit of immediate and aggressive treatment options. Even if there is a general consensus that hypopharynx SCC is predominant in males,30,31 we further found that married/partnered males may benefit more than females, which relates to spousal influence on adoption of healthy behaviors, as well as support to quit harmful risk factors associated with worse survival outcomes. 32 Takagi et al 33 found that there was a spillover effect of the wife’s nonsmoking behavior only among men. Women tend to have a greater influence on their spouse’s health than men because women exert more effort to control their partners’ health habits.26,32 Generally speaking, the support received by male patients to adopt healthier lifestyles and have a positive outlook may explain their greater survival benefit from being married. The differential protective effect of marriage based on gender among hypopharynx SCC patients is a novel finding, which is important for care planning and needs further studies to reveal the potential mechanism generating the influence of marital status on prognosis. While not explored in this study, another mechanism that might explain the survival benefit of being married could be that unlike those not married, married HNC survivors are able to rely more on their spouses for everyday tasks, such as transportation, cleaning, and shopping. 34 Extant literature (about non-head and neck) as well as anecdotal evidence support the idea that being married improves oral intake and hydration especially among married men. 35 Another quality of life issue that might be affected by marital status is seeking transportation to treatment facilities. It could be that married patients are more able to rely on their spouses to help with transportation. A previous study on sarcoma survivors alluded to this and this idea also needs to be further tested among head and neck cancer (HNC) survivors. 36
We then explored the effect of marital status on prognosis by different subgroups, such as age, race, grade, and tumor location. Difference in protective effect of marriage was observed among variable subgroups, and the OS benefit of being married vanished in Asian/African American patients. Previous work has suggested that the effect of marriage on survival may differ between African American and Caucasian married men. 37 African American men have reported lower marital quality than Caucasian men, which may adversely affect their health by increasing negative health-related behaviors and promoting stress-related immune system suppression. 38 Some literature has suggested that marriage provides very little health-related protective effects for African Americans when compared with those for Caucasian men. 37
In further analysis, we found that the OS benefit mostly occurred in patients who harbored well/moderately differentiated and nonmetastatic disease. When considering patients affected by more aggressive disease, marital status was not significantly associated with higher risk of dying from hypopharynx SCC.
Several limitations should be noted in this study. First, the SEER database does not include change of marital status after cancer diagnosis. Second, the lack of data on additional predictors of OS such as performance status, comorbidities, tobacco smoking, and alcohol consumption prevented us to adjust our analyses for these important factors. Third, the study uses data up to 2014, which may not reflect more recent trends in cancer diagnosis and treatment. In addition, the study’s findings may be specific to the population covered by the SEER database and may not be generalizable to other populations. Finally, also due to the data limitations of the SEER database, positive surgical margins at final pathology were not analyzed between marital status and survival in this study.
Conclusion
As far as we know, this is the first study to determine that the effect of marital status on prognosis varies by the demographic and pathological factors in hypopharynx SCC. Our results demonstrated that while there are survival benefits for married patients with hypopharynx SCC, married/partnered males may benefit more than females, which affected by the age, race, and gender. Further studies should be conducted to clarify the specific influence and mechanism of these factors.
Footnotes
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Shanghai Municipal Health Commission (Grant Number: 20214Y0025) and the Shanghai Pudong New Area Heath Commission (Grant Number: PW2022A-41).
Ethical Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of Fudan University Shanghai Cancer Center Ethics Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The experimental protocols were also approved by Fudan University Shanghai Cancer Center Ethics Committee. Written informed consent was obtained from all individual participants included in the study.