
Abstract
Introduction
Hypopharynx squamous cell carcinoma (hypopharynx SCC) is one of the most common cancers of the head and neck cancer and is considered to occur frequently after 40 years old.1,2 Approximately 70% to 85% of the patients reported have disease at presentation in large series, and the 5-year overall survival rate is reported to be around 15% to 45%. The primary therapeutic strategy for patients has been chemoradiotherapy and systemic therapy, and surgery has been reserved based on a multitude of factors.3-5
With the development of treatment strategies, the survival of patients with hypopharynx SCC has been significantly improved. 3 The introduction of immunotherapy targeting the programmed death-1/programmed death–ligand-1 axis has represented a turning point in the treatment of head and neck squamous cell carcinoma.6-10 However, seldom study looked into the patients who died early after diagnosis. Patients with high risk of early death (ED) should be timely identified so that individualized treatments and/or supportive care can be scheduled to improve their survival and life quality. Therefore, the objective of this study is to evaluate the early mortality rate and associated factors for ED in a large cohort of patients with hypopharynx SCC.
Materials and Methods
Cohort Population
The Surveillance, Epidemiology and End Results (SEER) database (http://www.seer.cancer.gov/seerstat) consists of 18 population-based cancer registries that covers approximately 28% of the United States population, and is freely available for cancer-based epidemiology investigation and survival analysis. Patients with hypopharynx SCC were extracted from the SEER database between 2004 and 2014. According to the previous literature, the ED was defined as overall survival time ≤3 months after initial diagnosis.11,12 We selected patients with only one primary malignancy in their lifetime. A total of 2659 hypopharynx SCC patients were included.
Statistical Analysis
Log-rank test and the Cox proportional hazard models were used to determine the risk factors. All statistical analyses were made using IBM SPSS 24.0. P values were two sided and P < .05 were considered significant.
Results
Incidence and Cause of ED
A total of 2659 hypopharynx SCC patients were included in this population-based study, and 307 (11.5%) patients died within 3 months after cancer diagnosis, among whom 243 (79.2%) patients died from cancer-specific cause. Patients with non-cancer-specific ED mainly died from heart disease (25.0%) (Figure 1).
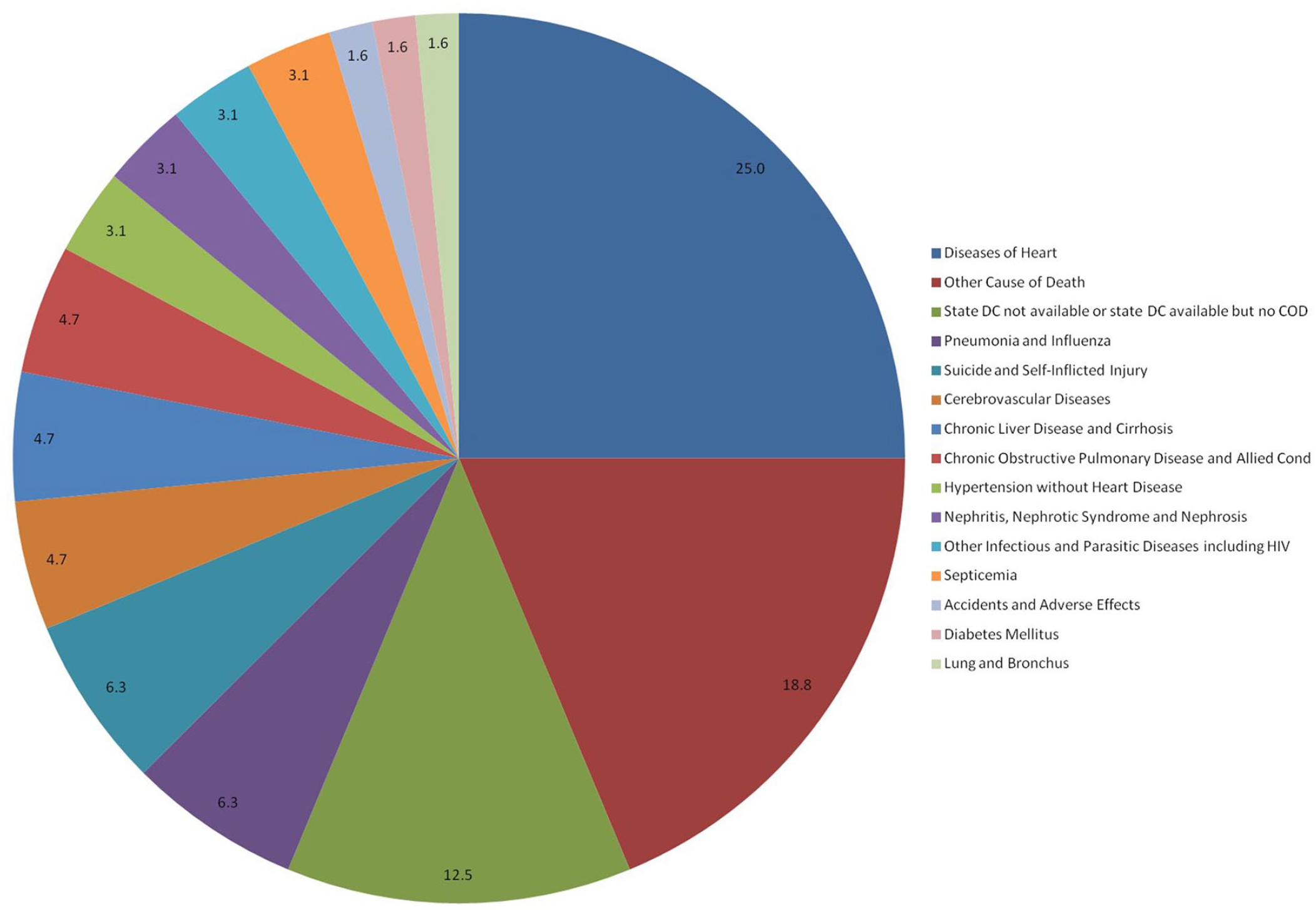
Distribution of the incidence of non-cancer-specific early death among hypopharynx SCC patients. SCC, squamous cell carcinomas.
Demographic and Clinical Characteristics of all Patients
The mean age of patients was 62 years old (range: 23-95 years old). Most patients with ED were black, divorced/single/widowed (DSW), advanced T stage, distant metastasis, not receiving surgery, and diagnosed after 62 years old (P < .001, respectively). The basic clinicopathological information is summarized in Table 1.
Demographic Characteristics of Hypopharynx SCC Patients.
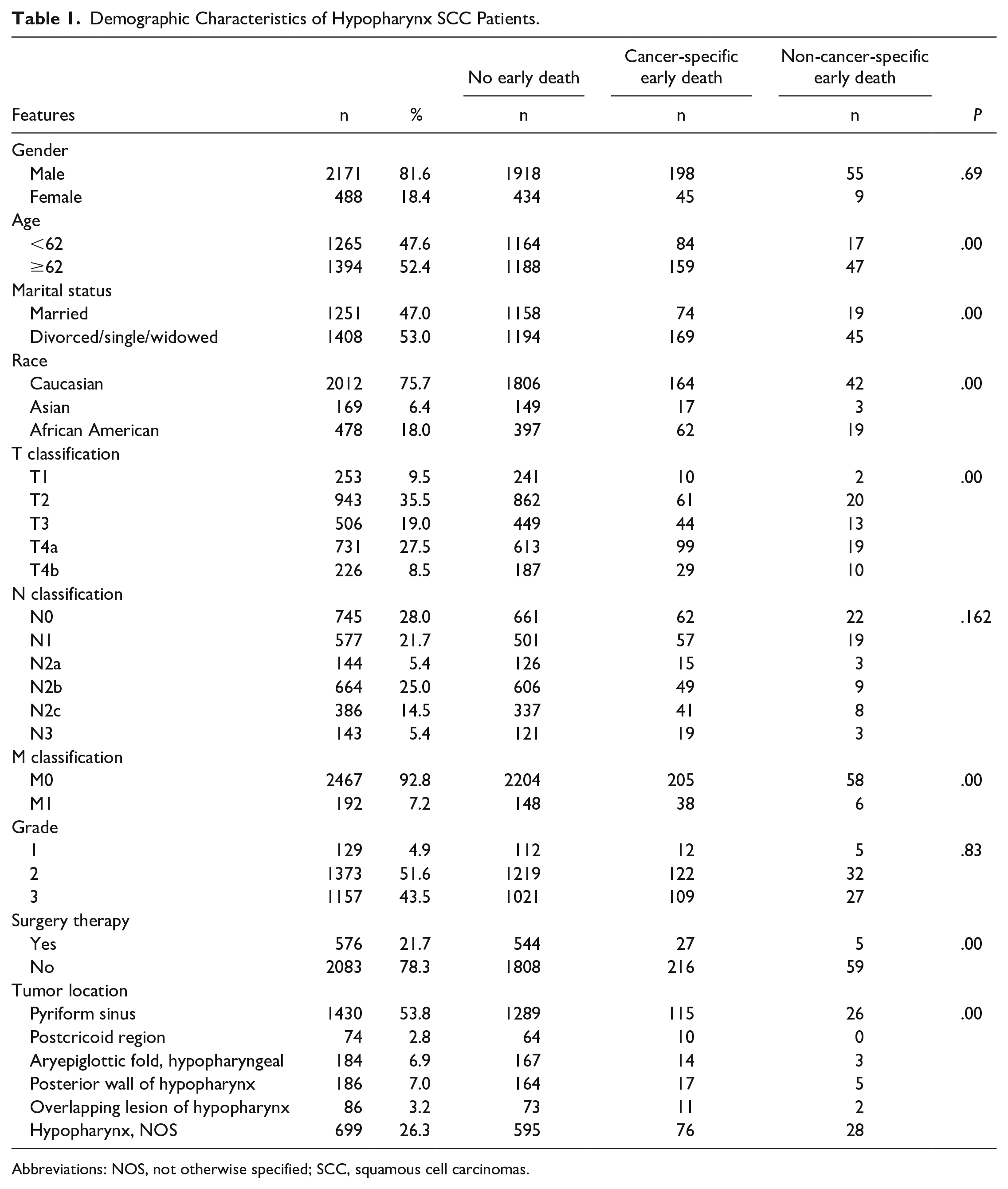
Abbreviations: NOS, not otherwise specified; SCC, squamous cell carcinomas.
Risk Factor Analysis for ED
As shown in Table 2, advanced age, DSW, non-Caucasian, advanced T stage, distant metastasis, and no surgery were significantly associated with all-causes and cancer-specific ED (P < .05, respectively) (Table 2).
Univariate Logistic Regression of Risk Factors for Early Death.
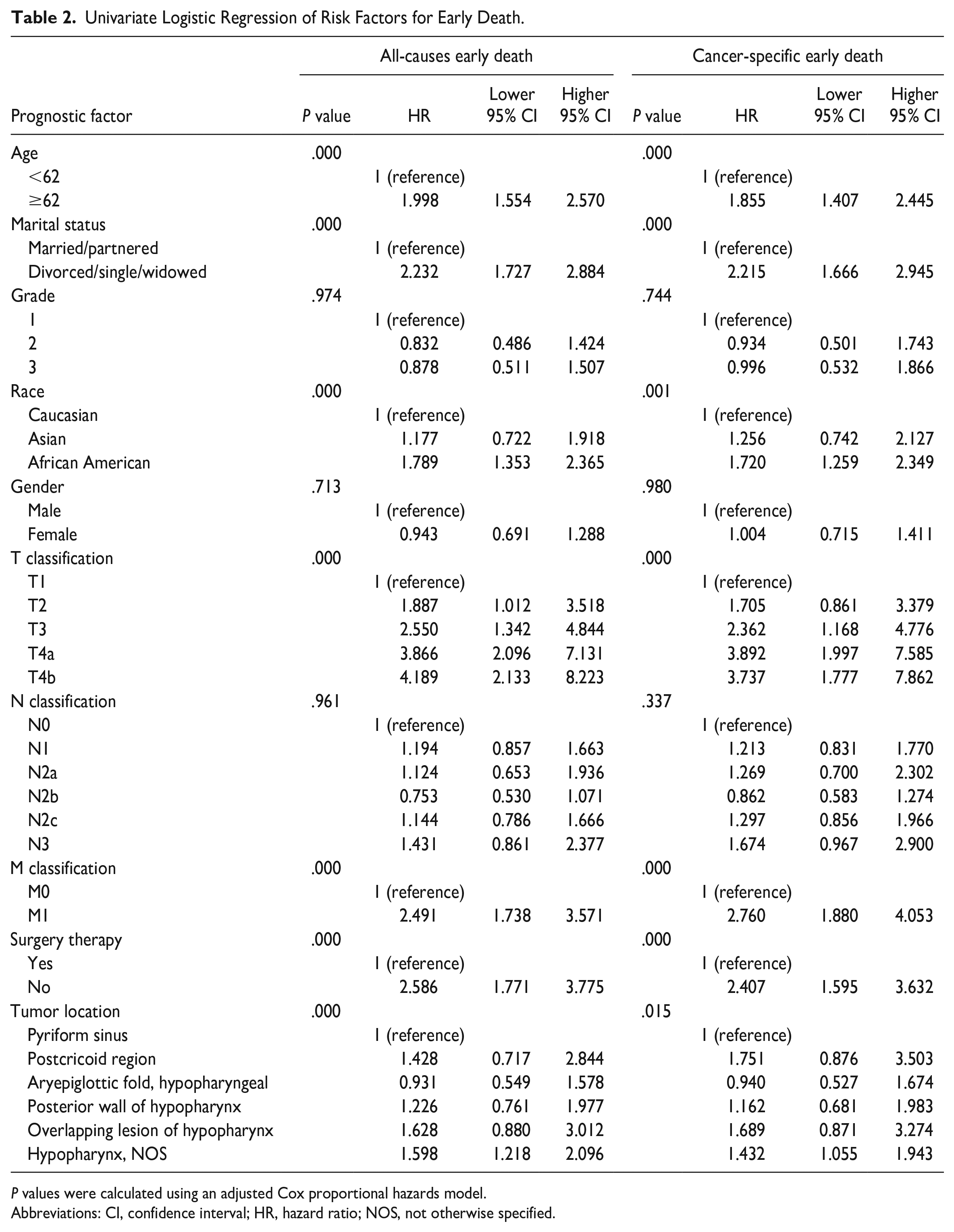
P values were calculated using an adjusted Cox proportional hazards model.
Abbreviations: CI, confidence interval; HR, hazard ratio; NOS, not otherwise specified.
These risk factors associated with all-causes and cancer-specific early mortality, identified in the univariate logistic regression analyses, were included in the multivariate logistic analyses, which found that advanced age, DSW, advanced T stage, distant metastasis, and no surgery were significantly associated with all-cause and cancer-specific ED (P < .05, respectively) (Table 3).
Multivariate Logistic Regression Analysis of Risk Factors for Early Death.
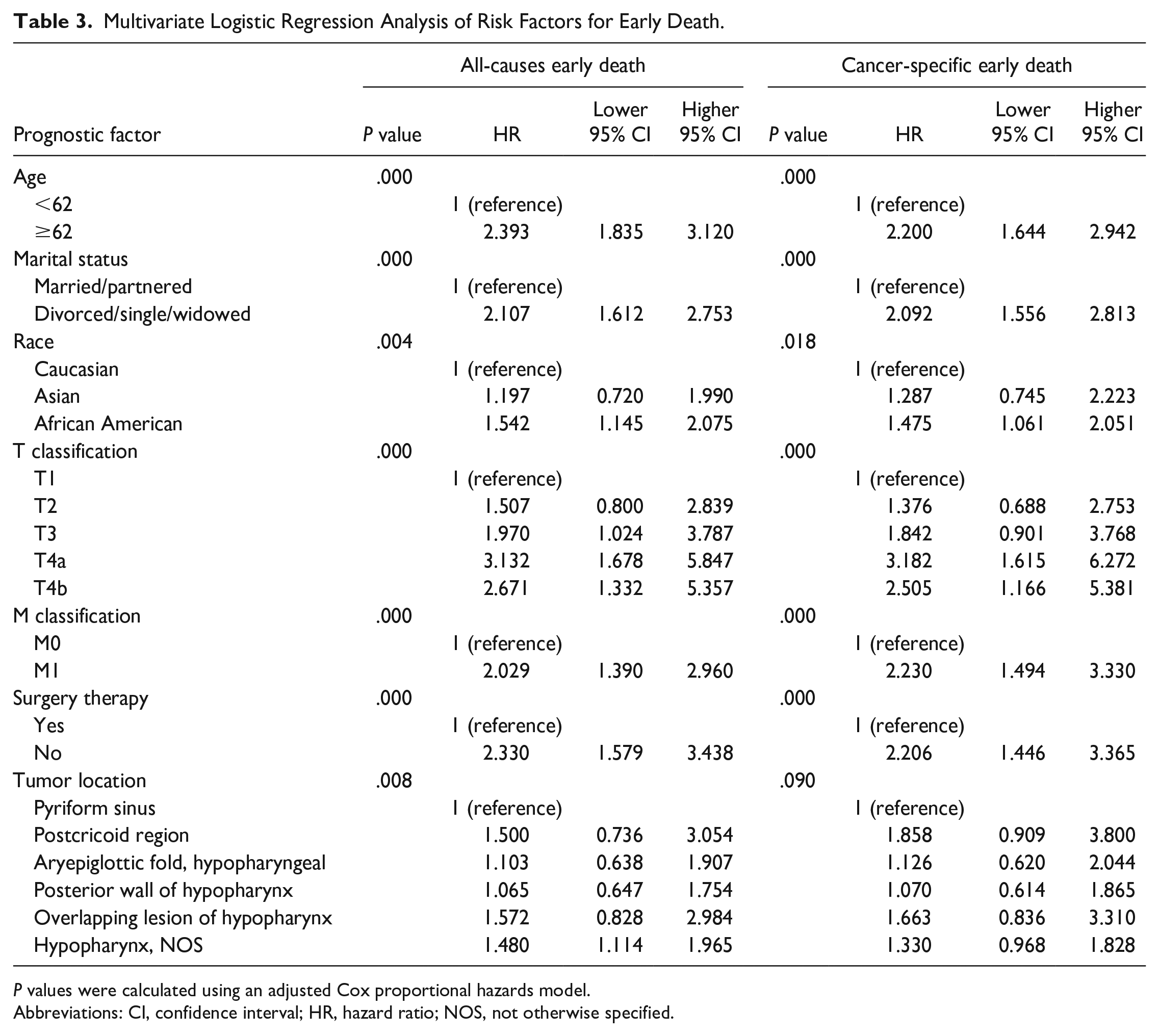
P values were calculated using an adjusted Cox proportional hazards model.
Abbreviations: CI, confidence interval; HR, hazard ratio; NOS, not otherwise specified.
Discussion
Studies on the prognosis of malignant tumors usually focus on the long-term survival of patients; only a few studies have focused on ED.13,14 The risk of ED is higher for more aggressive or advanced tumors. The definition of ED varies from study to study.12,13,15 Some studies defined it as 30 days or 3 months after surgery. Different definitions of the time of ED correspond to different early mortality rates. If the definition of ED is too short, the number of patients in the ED cohort is too small and the study bias is large. Finally, our study defined ED as 3 months after surgery. Identifying patients at risk of ED is critical for reducing the burden on patients, for whom the side effects of treatment and the inconvenience of getting to the hospital may outweigh the benefits of treatment. Therefore, we assess the early mortality rate and associated factors for ED in a large cohort of patients with hypopharynx SCC.
In this study, the cancer-specific cause was proved to be the most important reason, resulting in 79.1% of all the EDs in the patients with hypopharynx SCC. The American Joint Committee on Cancer (AJCC) stage was not the only predictive factor for ED; other social factors and treatment measures, such as older age, non-Caucasian, unmarried status, and no surgery, were also associated with higher all-causes ED and cancer-specific ED. The AJCC staging system is a commonly used method to evaluate the prognosis of hypopharynx SCC, but its limitations make it unable to provide a personalized prognosis prediction.
The prognostic effect of patients’ age at diagnosis for patients with hypopharynx SCC has been suggested by several studies, with the results showing that younger patients will have longer survival than older patients.16,17 In the present study, we found that patients’ age at diagnosis also had an effect on the early mortality of patients with hypopharynx SCC and advanced age was an independent risk factor for all-causes ED and cancer-specific mortality. Older age and ED can be significantly correlated for several reasons. Life-threatening non-infectious chronic disease, including other cancer, cardiovascular, cerebrovascular, chronic obstructive pulmonary diseases, and diabetes are more prevalent in the older population. This patient population is more likely to have weak immune systems, which accelerates deterioration leading to early mortality.18-21
Previous studies assessing the effect of marriage on outcomes showed that marriage was associated with better survival, and the protective effect of marriage might result from that married people were associated with earlier stage and more likely to receive recommended or aggressive treatment, which was known as “spousal surveillance.”22-27 In addition, married patients were considered to have more financial and emotional support, which may account for the results that being unmarried resulted in the higher early mortality probability.28-30
As to the tumor behaviors, advanced T stage and distant metastases were associated with higher odds of total, and cancer-specific ED. Distant metastases were related to unfavorable prognoses in hypopharynx SCC patients. Li 5 found that 5-year overall survival are 53.1% and 29.2% for localized and regional hypopharynx SCC patients, respectively, which are much higher than metastatic hypopharynx SCC patients (24.6%). This study also found that ED was associated with advanced T stage and distant metastasis, which was due to vital organ damage and tumor load increase to lethal levels. All these serious aggressive factors should be considered in the estimation of early mortality.
Among the investigated variables in this study, surgery was one of the most important protective factor for early mortality. As with all retrospective reviews, there was a possible patient selection bias contributing to the better results in the patients after surgery. Patients with better conditions and less risk were reported to be more likely to receive surgical interventions. 31
This study was the first to directly evaluate the incidence and risk factors for recognizing the ED of hypopharynx SCC patients. It is important to describe some of the limitations in this study. First, retrospective studies are inherently biased. Second, the lack of data on additional predictors of earth death such as comorbidities, performance status, and systemic therapy prevented us to adjust our analyses for these important factors due to the data limitations of the SEER database. Despite these limitations, the population-based design and large number of patients make the results generalizable to the American population, which gives insight to predict ED to provide better personalized treatment hypopharynx SCC patients at high risk of early mortality probability.
Conclusion
Our results showed that a total of 11.5% patients with hypopharynx SCC suffered ED, among whom 79.2% patients died from cancer-specific cause. Predictors of ED are primarily related to age older than 62 years, advanced T stage, distant metastasis, and no surgery but also include unmarried status; better prognostic and predictive tools for select ED patients in larger sample size are needed.
Footnotes
Acknowledgements
None.
Author Contributions
Yujiao Li and Chaosu Hu have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be submitted.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Clinical research on health industry of Shanghai Health Commission (Grant number: 20214Y0025) and the Clinical research of Shanghai Pudong District Health Commission (grant number: PW2022A-41).
Ethical Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.