
Abstract
Keywords
Introduction
Otogenic brain abscess (OBA) with high mortality rate, is one of the intracranial complications of otitis media. This condition affects the brain parenchyma and can lead to brain hernia. The development of antibiotic products and imaging technology, as well as the increasing attention paid to middle-ear diseases, mean that OBA is rare but still appears sporadically. Indeed, due to the lack of specific symptoms and signs in early stages, OBA is easy to delay diagnosis or miss diagnosis. 1 Moreover, there are no recognized standard treatment guidelines and even few related studies were reported referring to OBA. Thus, different medical institutions have their own experiences in the diagnosis and treatment of OBA. To deeply explore the clinical characteristics of OBA and summarize its diagnosis and treatment experience, we analyzed and summarized the clinical data of patients with OBA who were treated in the First Affiliated Hospital of Wenzhou Medical University between February 2015 and February 2020 as well as the Aksu First People’s Hospital of Xinjiang between April 2020 and April 2021.
Patients and Methods
The clinical data of 10 patients with OBA treated in the above hospitals (the First Affiliated Hospital of Wenzhou Medical University between February 2015 and February 2020 as well as from the Aksu First People’s Hospital of Xinjiang between April 2020 and April 2021) were analyzed retrospectively. All patients received interdisciplinary consultation for comprehensive diagnosis and treatment. The comprehensive diagnosis evidence includes medical history (including symptoms, signs, past medical history, and medical history, etc), imaging examination results, etiology examination results, intraoperative findings, and the consultation opinions of specialists (form the department of infectious disease, neurology, and neurosurgery). The comprehensive treatment plan is surgical treatment combined with anti-infection treatment. The initial antibiotic selection is mostly empirical, and it is adjusted according to the results of etiological examination (including bacterial culture and fungal culture) of ear canal secretion, middle-ear surgery cavity pathological tissue, and brain abscess pus.
Results
General Data
Among the 10 patients, there were 7 males and 3 females. The age ranged from 8 to 69 years. The time from the onset of the first symptom to the diagnosis of OBA varies from 1 day to 2 months. Except for 1 case of multiple and bilateral abscesses, all other cases were unilateral. In the 9 unilateral cases, the brain abscess and the affected ear were on the same side, with 2 cases in the left ear and 7 cases in the right ear, and 6 temporal lobe abscesses and 4 cerebellar abscesses, including 2 temporal lobe abscesses combined with cerebellar abscesses. Five cases were accompanied by 1 or more intracranial complications, including meningoencephalitis, hydrocephalus, cavernous sinusitis, thrombophlebitis, cerebral hernia, and subdural abscess (Table 1).
Information of First Diagnosis, Initial Symptoms, Consultation, and Brain Abscess.
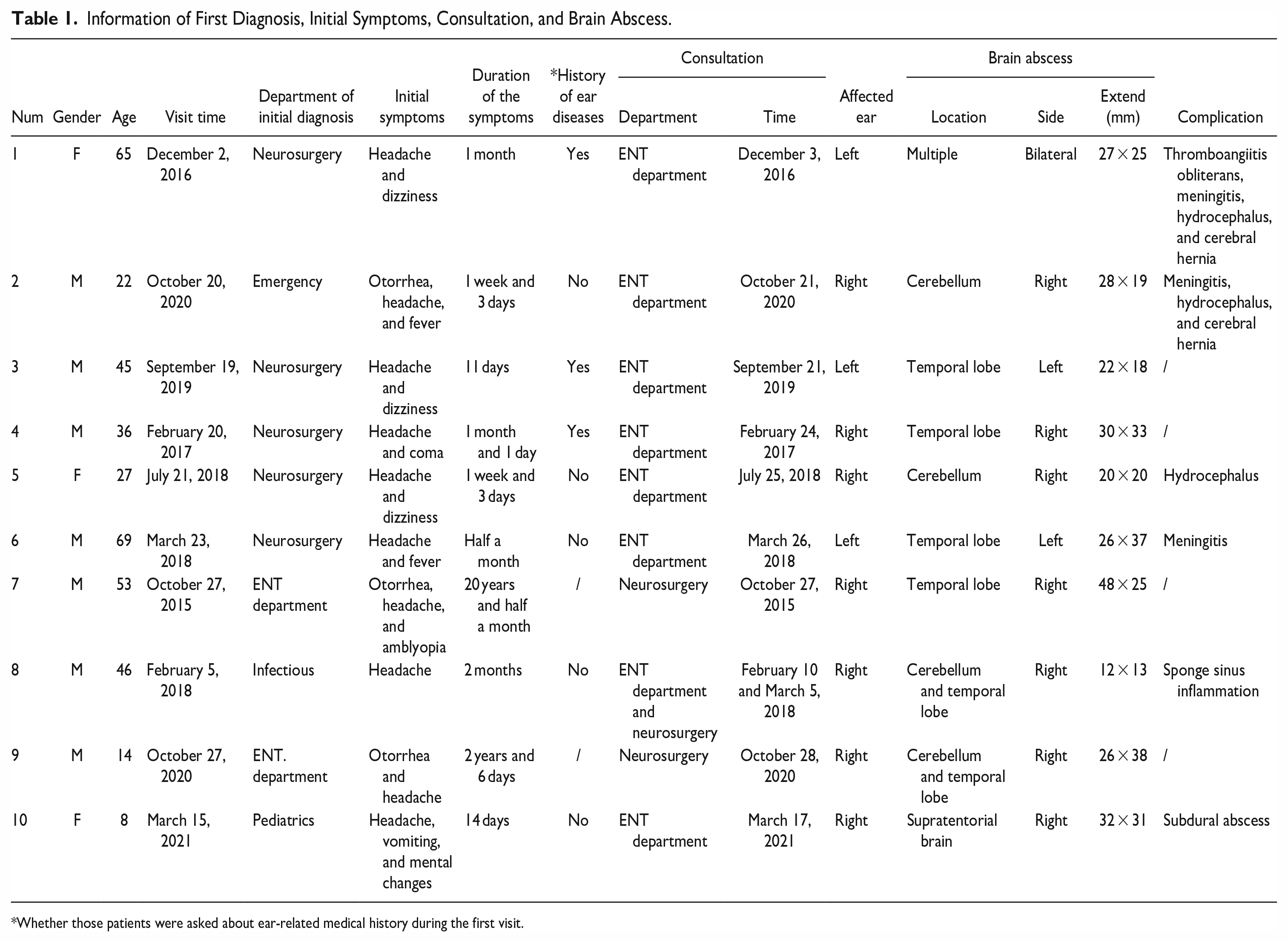
Whether those patients were asked about ear-related medical history during the first visit.
Diagnosis Process
Out of the 10 patients, 2 were initially diagnosed in the ENT department, 5 in neurosurgery, and 3 in other departments (emergency department, infection department, and pediatrics). Out of the 8 non-otorhinolaryngologic first-diagnosed cases, only 3 (37.5%) were asked about ear-related medical history; all 8 patients were referred to the ENT department for consultation. The consultation was conducted 1 to 5 days after admission, with an average of 2.75 ± 0.52 days (Table 1).
Clinical Manifestations
A headache of varying degrees was a common manifestation in all cases; 3 cases coexisted with otorrhea. (During this study, it was learned through telephone follow-up that another 7 cases suffered otorrhea in the past). The remaining clinical manifestations were fever in 2 cases and mental changes in 7 cases (comprising 4 cases of coma, 3 cases of drowsiness and listlessness), dizziness and unsteady walking in 2 cases, nausea and vomiting in 2 cases, limb convulsions in 2 cases, and speech ambiguity in 1 case (Table 1). All cases had negative pathological signs and no symptoms or signs such as visual field defect, epilepsy, and papilledema.
Etiological Examination
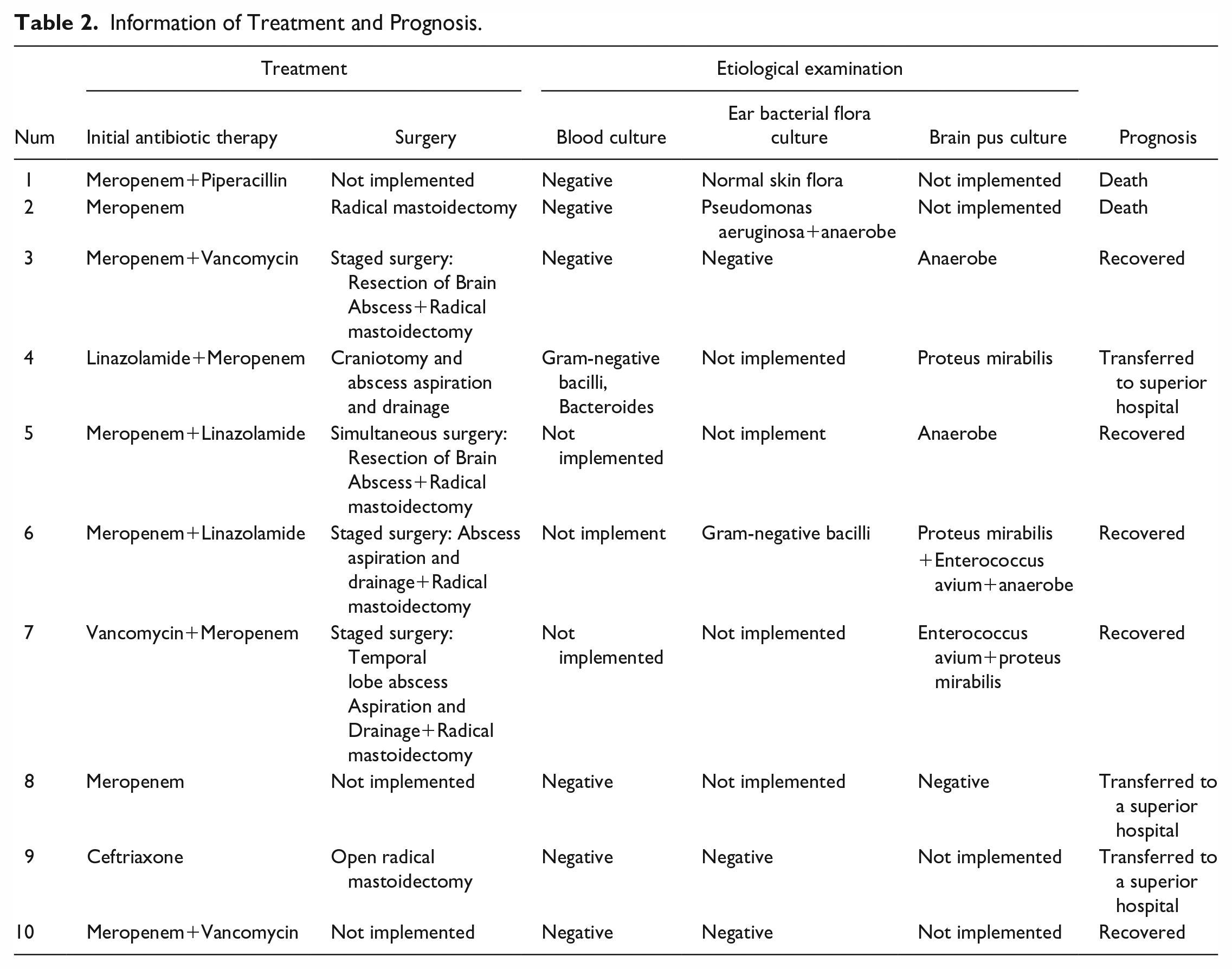
All patients underwent etiological examination, while only 1 patient underwent complete blood culture, ear secretion culture, and brain abscess secretion culture. Blood culture was performed in 7 cases; 1 was positive (with a positive rate of 14.3%); ear bacterial flora culture (the samples from auditory canal secretions or surgical cavity tissue or moist tympanic chamber through perforated tympanic membrane) was performed in 6 cases; 2 of these were positive (positive rate is 33.3%); and brain pus (puncture fluid, surgical cavity drainage fluid, etc.) were cultured in 6 cases; a total of 5 of these cases were positive (positive rate is 83.3%); notably in 1 case that the bacterial culture was negative in samples collected by abscess puncture and drainage. Culture results were mainly anaerobic bacteria: Proteus mirabilis in 7 cases, Avium enterobacterium in 5 cases, Bacteroides polymorpha in 3 cases, and Providencia rosenbergii in 3 cases (Table 2).
Information of Treatment and Prognosis.
Imaging Examination
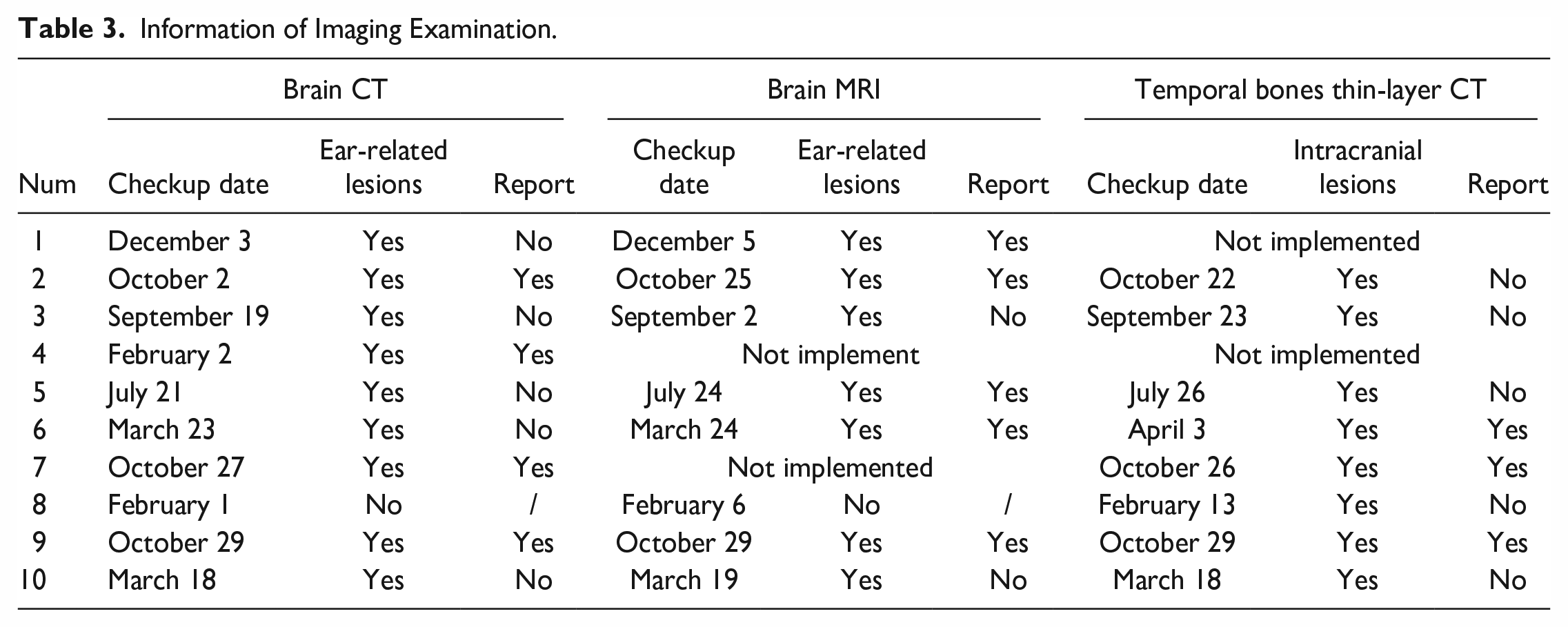
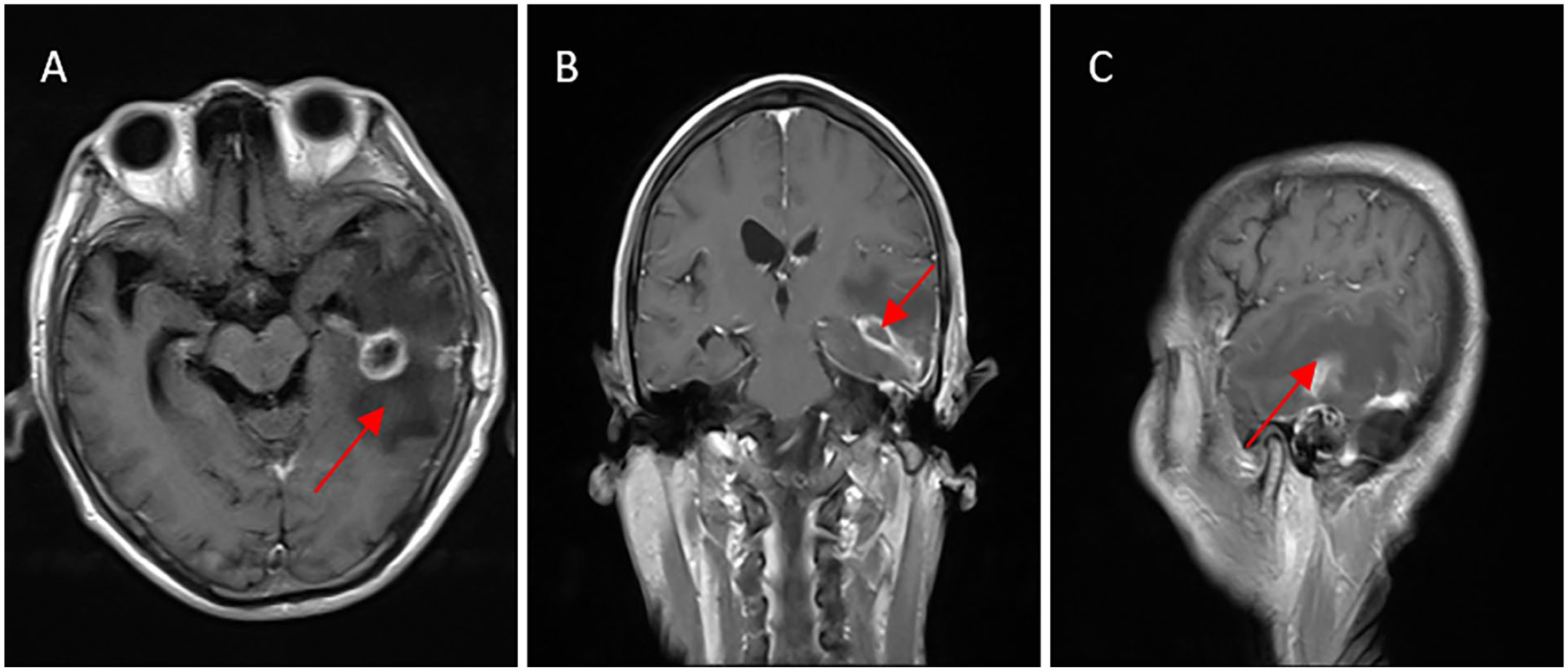
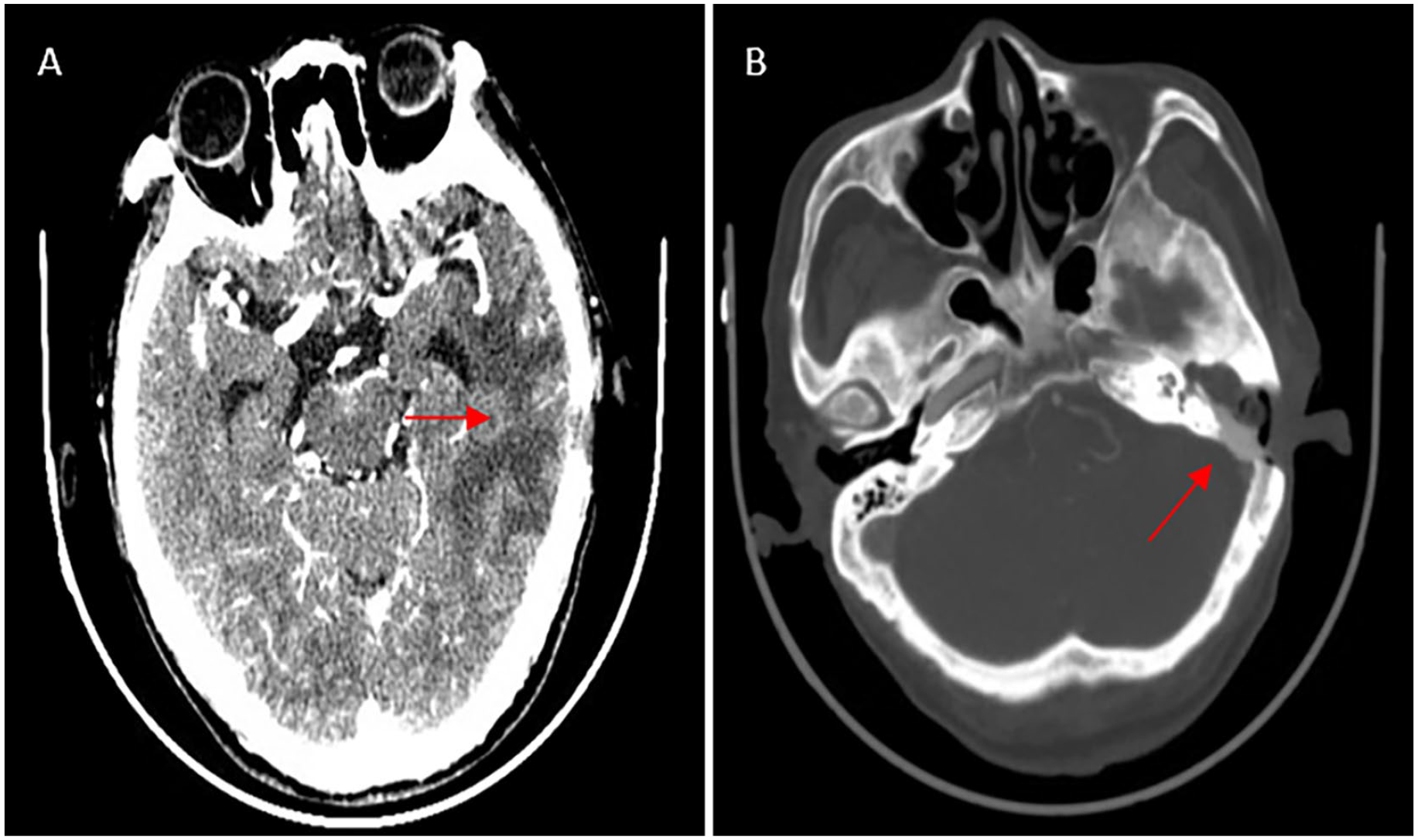
After admission, this group of patients underwent 10 brain CT examinations, 8 brain MRI examinations, and 8 temporal bones thin-layer CT examinations. The first implementation times of these examinations were 14.4 ± 8.1 h, 60.0 ± 12.8 h, and 90.0 ± 28.2 h from the patient’s admission time, respectively. In all patients with brain abscesses, the lesions showed 1 or several circles with short T1 and long T2 on MRI and significant enhancement at the lesion edges (Figure 1A to C) and high Diffusion weighted imaging (DWI) signal intensity. One case of sigmoid sinus thrombophlebitis showed thickening of the wall of the sigmoid sinus on MRI (Figure 1D). MRI of hypertrophic meningitis shows thickening and enhancement of the cerebral surface meninges in the cerebellar tentorium, temporal lobe, and cerebellar hemisphere, with equal or long T1 and short T2 signals. When enhanced, the enhancement can be seen, and the cavernous sinus is involved. Brain parenchyma abscess was found in 9 cases of cranial CT examination (Figure 1E), 2 cases of abscess ruptured into the ventricle, cerebellar abscess accompanied by peripheral cisterns, tentorial regions, and subdural empyema in 1 case. Nine cases receiving brain CT showed different degrees of middle-ear cavity lesions (Figure 1F), and 5 of them did not describe ear-related lesions in the issued reports. All 8 cases of temporal bone thin-section CT examination found soft tissue shadows in the mastoid cavity, 6 cases had bone defects of the mastoid canopy, and 1 case had moth-eaten bone around the sigmoid sinus with osteomyelitis changes (Table 3).
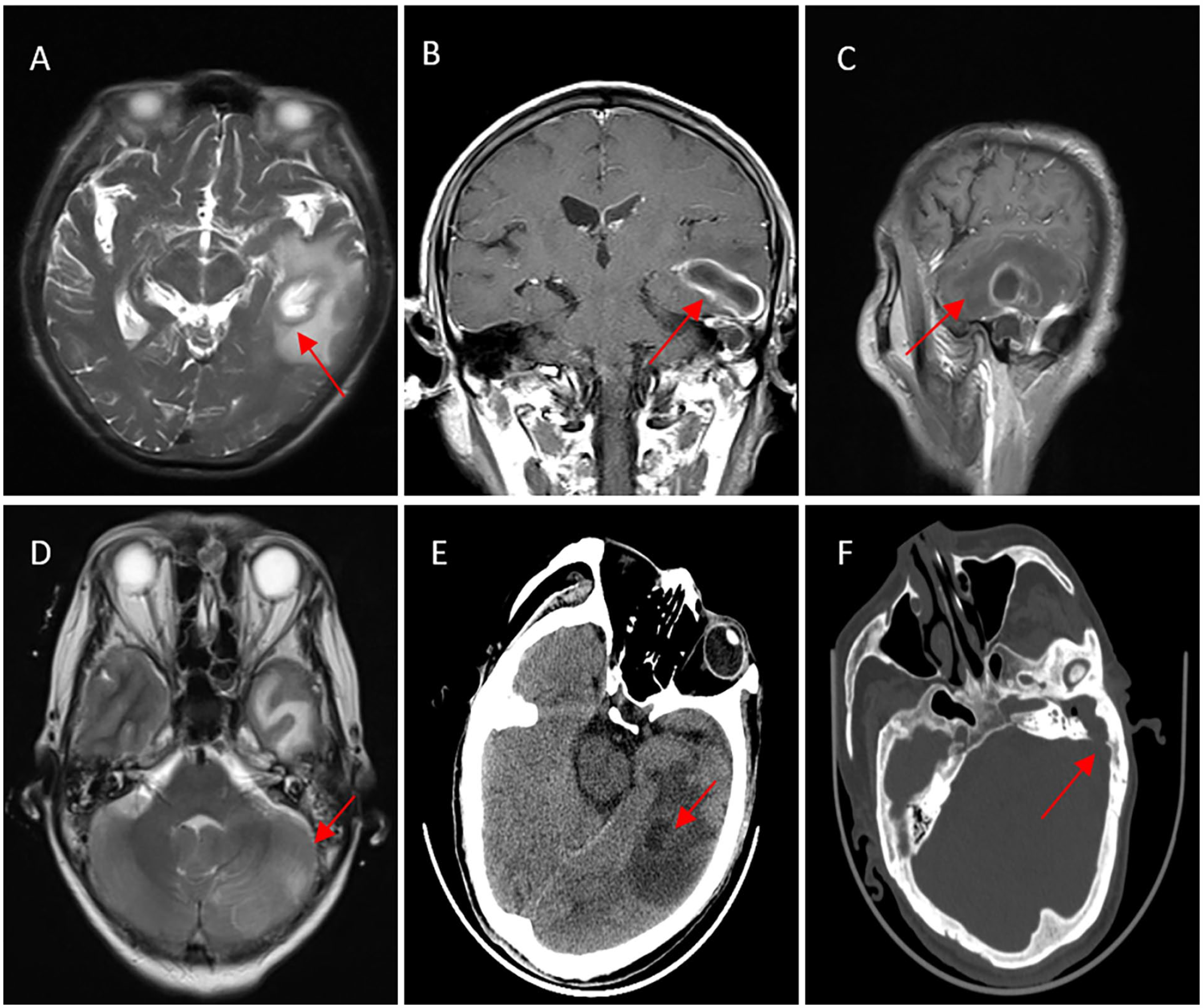
Preoperative imaging examination of typical brain abscess. (A) (T2WI, horizontal position). (B) (T1WI-enhanced, coronal position). (C) (T1WI-enhanced, sagittal position): The left temporal lobe has a gourd-shaped abnormal signal, high signal on T2WI, and obvious edema around the lesion. The size ranges from approximately 26 × 26 × 23 mm and presents circular enhancement. (D) (T2WI, horizontal position, enhanced). Thickening of the wall of the left sigmoid sinus (the red arrow). (E) Cranial CT (horizontal position, soft tissue window): Low-density nodules can be seen in the left temporal lobe (the red arrow), and large areas of edema can be seen around. (F) Cranial CT (horizontal position, bone window): The left mastoid process is filled with a soft tissue signal, and the posterior wall bone is destroyed, communicating with the brain (the red arrow).
Information of Imaging Examination.
Treatment
All patients had no previous ear or brain surgery history, and no history of traumatic brain injury, and did not receive regular treatment for brain abscess before hospitalization. One case of cerebral abscess and brain herniation was admitted. At that time, the patient was in a state of central respiratory depression and received conservative treatment. One patient was transferred to a higher level hospital for treatment due to misdiagnosis of tuberculous encephalitis and meningitis (receiving antituberculosis treatment during hospitalization). One patient refused surgery due to requesting further treatment from a superior hospital. The remaining 7 cases were all treated with comprehensive treatment of surgery and antibiotics, and other treatment methods included eliminating edema and nourishing brain nerve cells. Meropenem is the main choice of antibiotic based on the results of bacterial culture. In otology surgery, radical mastoidectomy was performed in 6 cases according to the preoperative imaging data, and the granulation or cholesteatoma tissue in the operation cavity was removed completely. In brain surgery, stereotaxic abscess puncture and drainage for brain abscess was performed in 3 cases, and abscess removal was performed in 3 cases. One patient with multiple brain abscesses was transferred to a higher level hospital for further treatment of brain abscess after radical mastoidectomy and 35 days of continuous anti-inflammatory treatment in our hospital. The postoperative condition improved in 1 patient who underwent radical mastoidectomy, and then lethargy reappeared. MRI reexamination revealed the formation of cerebellar abscess with hints of cerebellar abscess, accompanied by surrounding brain cisterns, cerebellar tentorium, and subdural empyema. Neurosurgeons recommended further neurosurgical treatment. The families could not accept the risk of surgery and refused relevant surgical treatment. Of the 7 patients who underwent ear surgery and/or brain abscess surgery, 1 patient underwent only radical mastoidectomy, 1 patient underwent only craniotomy and abscess drainage, and 2 patients underwent ear mastoidectomy and brain abscess surgery during the same period (Table 3).
Prognosis and Outcome
Two patients died, including 1 patient with central respiratory failure due to cerebral hernia, and the other patient died due to diffuse subdural abscess in the cerebellum. Three patients were transferred to a superior hospital for further surgical treatment: one patient underwent open mastoidectomy of the right ear and was transferred to a superior hospital for brain abscess resection, the other patient underwent craniotomy and puncture drainage for brain abscess and the condition got stable after surgery; later, this patient requested to go to a superior hospital for further treatment. They were followed up by phone and reported recovery and discharge. Five patients (including 1 patient with an abscess that ruptured into the ventricles of the brain and developed cerebral hernia) recovered after comprehensive treatment in our 2 hospitals and were discharged (Figures 2 and 3). They were followed up for half a year to 5 years, and there were no recurrent cases (Table 3).
MRI examination 10 days after brain abscess surgery. The images were T1WI enhanced in the horizontal position (A), coronal position (B), and sagittal position (C). The left temporal lobe showed a strip-shaped abnormal signal (image A), which showed ring potentialization after enhancement (image A and B), with a size of approximately 32 × 10 mm. The surrounding edema was obvious (image C), and the lesion was significantly smaller before the operation.
CT examination 21 days after brain abscess surgery. (A) After surgery, there was a partial absence of the left skull, and a large area of patchy low-density shadow was seen in the left temporal region (the red arrow), which was smaller than before surgery. (B) Dense shadows (bone powder filling) can be seen at the mastoid defect (the red arrow) and the outer ear, and soft tissue density filling can be seen in the ear canal.
Discussion
Middle-ear cholesteatoma is the most common cause of OBA. 2 Bacteria invaded into brain parenchyma through the damaged mastoid canopy or bone in the posterior fossa. Cholesteatoma can not only erode bone but also often form bacterial biofilms, rendering antibiotics useless. OBA is the most serious complication of otitis media and has a high mortality rate. 3 In 1991, the editorial board of the Chinese Journal of Otolaryngology compiled data from 21 medical units in China, and the mortality rate of 768 OBA cases was 22.7%. 4 Over the past 30 years, all diagnostic and therapeutic techniques, including surgery, pharmacology, and imaging, had been rapidly developed. However, the mortality rate of OBA cases in this study is still as high as 20%, which is similar to that in 1991. The high fatality rate reminds us that even today, all aspects of the diagnosis and treatment of OBA still need to be vigilant.
Similar to other brain abscesses, the pathological evolution of OBA also experienced 3 stages: acute suppurative meningoencephalitis, suppurative, and capsule formation. Therefore, patients with OBA lack specific clinical symptoms, mainly manifested as fever, headache, and focal neurological deficits, which is a typical triad of brain abscesses. Most literature reports show that headache is the most common symptom of brain abscess, 5 and the results of this study are consistent with those findings. Because of headache and fever, patients often choose to go to the neurology department, neurosurgery department, infection department, or ICU for treatment first. Clinicians focused mainly on the relevant medical history of their specialty and tend to ignore the middle-ear medical history, signs, and related examination results, which greatly delays the time for the patient to obtain the relevant consultation from the otolaryngologist. In this study, cranial CT of 9 patients showed lesions in the middle-ear cavity, with a positive rate of 90%. However, due to the inappropriate slice thickness of the brain CT examination and the professional limitations of some non-otolaryngologists and imaging physicians, ear lesions are easily overlooked, which delays the timely examination of temporal bone thin-section CT and ultimately causes the primary lesion of middle-ear cholesteatoma to be neglected, delaying the timely participation of otolaryngologists in the diagnosis and treatment and ultimately affecting the making of correct treatment decisions. MRI is the preferred examination method for the diagnosis of brain abscess, while in the diagnosis and treatment of chronic suppurative otitis media and cholesteatoma, CT and MRI examinations are essential. The lesions in middle ear show a granular characteristic signal pattern with a very high-intensity area in T2-weighted images of MRI, thin-section CT of the temporary bone are needed for ear surgery because of its clear display of lesions and surrounding bones. 6 Therefore, the precise diagnosis made by the first-diagnosed clinicians is based on a comprehensive analysis of MRI and temporal bone thin-section CT, which they should timely order and then be accurately imaging-diagnosed by an experienced radiologist for the discovery of primary lesions in the middle ear, the determination of the existence of cholesteatoma, and the judgment of the location, number, size, and capsule formation of brain abscesses.
The indications and timing of surgery for OBA have always been controversial. Radical mastoidectomy/extended radical mastoidectomy is the first choice for middle-ear cholesteatoma. 7 The granulation or cholesteatoma tissue in the operation cavity is surgically removed, and the diseased middle/posterior skull base bone is removed until the normal meninges or sigmoid sinus wall are exposed. Then, resection of the granulation on the surface of the meninges and sigmoid is performed to eradicate the primary lesion, which belongs to the etiological treatment. The treatment of brain abscess is symptomatic treatment, resection, and removal of intracranial infection lesions through craniotomy or stereotactic drainage led by neurosurgeons, coupled with long-term antibiotic treatment led by neurologists (typically 4-8 weeks, depending on the size of the brain abscess, the bacteria involved, and operability). 8 The indication for neurosurgery is a brain abscess with a diameter greater than 2.5 cm. Other surgical indications include impending cerebral hernia or periventricular abscess with a risk of rupture. 9 Although cholesteatoma is the primary lesion, it is not fatal. If brain abscess is not treated in time, it will easily lead to serious adverse prognoses, including death. Therefore, the priority of various treatment methods still needs to be determined after comprehensive evaluation by each department. We concluded and proposed the following: (1) The otolaryngology and neurosurgery teams make a personalized treatment plan together after fully evaluating the middle-ear lesion and the brain abscess, including whether there is an indication for surgery and whether the 2 departments perform simultaneous surgery or conduct the staging operation. If the staging operation is chosen, we recommend neurosurgery first to avoid further progression and poor prognosis of the brain abscess. If the abscess is close to the mastoid cavity, puncture and drainage through the mastoid cavity after adequate disinfection can also be considered. (2) If the patient is in critical condition and there is a sign of brain herniation, it is recommended to treat the brain abscess first and then remove the primary lesion by otological surgery after the patient’s condition is stable. (3)If the patient has a severe systemic infection and unstable vital signs, consultation and symptomatic treatment should be conducted with departments such as the infection department, ICU, and clinical pharmacy laboratory. Etiological treatment should be performed after the condition is stable. The outcome of patients in this study also reminds us that relying only on a single treatment by a certain department and lacking multidisciplinary comprehensive treatment, the patient’s condition is prone to be prolonged, or even aggravated.
Antibiotic therapy for OBA mainly addresses intracranial and/or systemic infections. The results of the etiological examination of the abscess play an important role in the determination of the pathogenic bacteria and the selection of antibiotics. The results of pathogenic bacteria culture in brain abscesses reported in past studies are different. Some studies reported that bacilli is the most common, 10 while others determined that anaerobic infection is of the domination. 11 However, some studies believe that the positive rate of bacterial culture in abscess puncture fluid is low. 12 The brain is the most common site of abscesses caused by anaerobic bacteria. 13 Staphylococcus aureus and Pseudomonas aeruginosa are the most common pathogenic bacteria in otitis media, while Pseudomonas aeruginosa and Bacteroides are the main pathogenic bacteria of cholesteatoma. Therefore, antibiotic treatment of OBA should be considered in combination with the above pathogenic characteristics. The etiological examination results of the cases in current study are mainly anaerobic bacteria, gram-negative bacilli and enterococci, and multiple bacterial infections coexisted. This result is also consistent with the above conclusions. Therefore, when the pathogenic results are unknown and empirical anti-infective treatment needed, the antibacterial spectrum of the selected antibiotic should cover the above flora. In terms of community-acquired OBA, considering its initial onset, the combination of ceftriaxone and metronidazole can be selected as the initial medication. If there is a possibility of methicillin-resistant Staphylococcus aureus (MRSA), vancomycin can be combined. If Pseudomonas aeruginosa is considered to cause the brain abscess, ceftriaxone can be replaced by cephalomepram. Linezolid has the characteristics of a strong ability to penetrate the blood–brain barrier and a broad antibacterial spectrum. In the event of the above treatment failure, the use of linezolid can be considered to address multidrug resistance.14,15 Of course, compared with empiric medication, anti-infection treatment based on the results of etiological examination is definitely more accurate. Un-fortunately, although surgery or physical examination of the relevant sites was performed, not all patients underwent pathogenic examinations related to these sites. This may due to overreliance on empirical anti-infective therapy and concerns that the time spent waiting for the results of pathogenic examination will delay and further aggravate the condition, and surgeons often prefer surgical treatment, thereby neglecting the importance of pathogen testing and subsequent accurate antibiotic therapy in treating OBA. In addition, the negative rate of bacterial culture in peripheral blood in this study was high, which may be related to the low bacterial content in peripheral blood and the long culture cycle.
Ratnaike et al. have shown that the state of consciousness is an important indication on the poor prognosis of brain abscesses. 16 Of the patients in this study, 4 were in a coma state at the time of treatment, and 2 of them recovered and were discharged uneventfully after comprehensive treatment with surgery and antibiotics. The other 2 cases were all accompanied by limb convulsions; 1 case with central respiratory failure had a left temporal lobe abscess breaking into the left ventricle; empyema on both sides of the ventricle, and the fourth ventricle, the other case died due to a cerebellar abscess, peripheral cistern, tentorial region, and diffuse subdural abscess in the cerebellar hemisphere during treatment.
In conclusion, the disease characteristics of OBA remind us that the process of diagnosis and treatment must be multidisciplinary. Therefore, OBA should still be considered by all relevant specialties, especially the emergency department, infection department, clinical pharmacy laboratory, otolaryngology, neurosurgery, and imaging department, as multidisciplinary consultation (MDT) is critical for the success of the first diagnosis of OBA. The diagnosis and treatment team develops personalized treatment plans by integrating MDT treatment opinions and combining the actual condition of patients, thereby making the diagnosis and treatment of OBA accurate and timely.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Zhejiang Province, China (LY20H130002), Basic public welfare scientific research project of Wenzhou Science and Technology Bureau (Y20210313).