
Abstract
This is the first report of vestibular examinations before and after the successful treatment of vestibular migraine (VM), a common cause of recurrent vertigo, with calcitonin gene-related peptide (CGRP) receptor inhibitor. We evaluated a 42-year-old female with VM and concomitant probable Meniere’s disease, whose headache and dizziness have improved promptly with the administration of erenumab, a CGRP receptor inhibitor. The sensorineural hearing loss in pure-tone audiometry, dysfunctions shown in vestibular examinations (cervical and ocular vestibular evoked myogenic potentials), and mild endolymphatic hydrops shown in gadolinium-enhanced inner ear magnetic resonance imaging, all in the right ear, revealed no change compared with those observed before treatment. This case suggests that VM may be treated by blocking CGRP in the trigeminal ganglion, which suppresses the effects on the vestibular nucleus; herein, no effects were observed in the inner ear despite the clear amelioration of dizziness.
Keywords
Introduction
Vestibular migraine (VM) is one of the most common causes of spontaneous episodic vertigo, 1 akin to Meniere’s disease (MD). 2 The condition is characterized by recurrent episodic vestibular symptoms associated with migraine features, occurring in patients with migraine or a history of migraine, and diagnosed using the criteria developed by the Barany Society and International Headache Society. 3 The prevalence of VM is estimated to be between 1% and 5%, with a recent US population-based survey finding it to be approximately 2.7%. 1 Although the pathophysiology of VM remains unclear, in addition to anti-vertigo medications, prophylactic therapies are performed based on traditional migraine. In the past half-decade, several medications targeting the calcitonin gene-related peptide (CGRP) molecule or the CGRP receptor for acute and prophylactic treatment of migraines have been developed. However, whether CGRP and its receptors are viable therapeutic targets in migraine patients with vestibular symptoms (including VM) remains unclear. 4 Hoskin et al 5 and Russo et al 6 reported the effectiveness of anti-CGRP medications in patients with VM, although they did not assess the examination results of vestibular function.
Recently, we encountered a case of VM and concomitant probable MD in which both headache and dizziness significantly improved with the administration of erenumab, a CGRP receptor inhibitor. As we performed vestibular examinations and gadolinium-enhanced inner ear magnetic resonance imaging (MRI), which may visualize endolymphatic hydrops (EH) in MD, before and after the treatment, we report the details of the clinical course and discuss the possible pathophysiology of VM.
Case Presentation
A 42-year-old female patient was referred to our department of otorhinolaryngology from otolaryngology clinic because of the fullness of her right ear lasting for 2 months and intractable dizziness for a month despite oral administration of isosorbide, adenosine triphosphate disodium hydrate, methylcobalamin, and prednisolone.
This was the patient’s first episode of dizziness, which did not correlate with changes in body position, but sometimes lasted all day, causing her to miss work since the first attack. She had no history of hearing loss or tinnitus. Although she had not complained of headaches by herself, a medical interview revealed that she had been experiencing frequent headaches since her teenage. Headaches with migrainous features (lasting until 1 d, pulsatile, accompanied by photo- and phonophobia, worsening with daily movements, nausea, located around the depth of the nose, and spread to the hemicranium, without aura) occur 8 times a month. She did not receive any medical treatment for the headache.
On her first visit to our department, the patient did not show any gaze nystagmus, non-gaze spontaneous or positional nystagmus, or head-shaking nystagmus. Non-gaze nystagmus and head-shaking nystagmus were observed with glasses, using an infrared charge-coupled device camera.
The results of neurological examinations are summarized in Figure 1. Pure-tone audiometry revealed a slight sensorineural hearing loss in the right ear, although the patient did not recognize any hearing differences between the ears. Glycerol administration did not improve the pure-tone audiometry. Canal paresis was not detected in either ear during the caloric testing. Cervical vestibular evoked myogenic potential (cVEMP) testing showed smaller amplitudes in the p13-n23 wave of the right ear, whereas ocular VEMP (oVEMP) showed smaller amplitudes in the p1-n1 wave of the right ear, indicating dysfunction of the otolith in the right inner ear. The tuning property test, 7 using the response to 500 and 1000 Hz short-tone burst in cVEMP, did not indicate EH in the saccules. After these examinations were performed, EH was evaluated using MRI. A standard dose of gadodiamide hydrate was injected intravenously, and a 3-Tesla MRI scan was performed 4 h later and subtraction images were evaluated. As a result, a mild EH was observed in the vestibule in the right ear according to a criterion for grading EH using MRI, 8 and no abnormal findings were revealed in the brain.
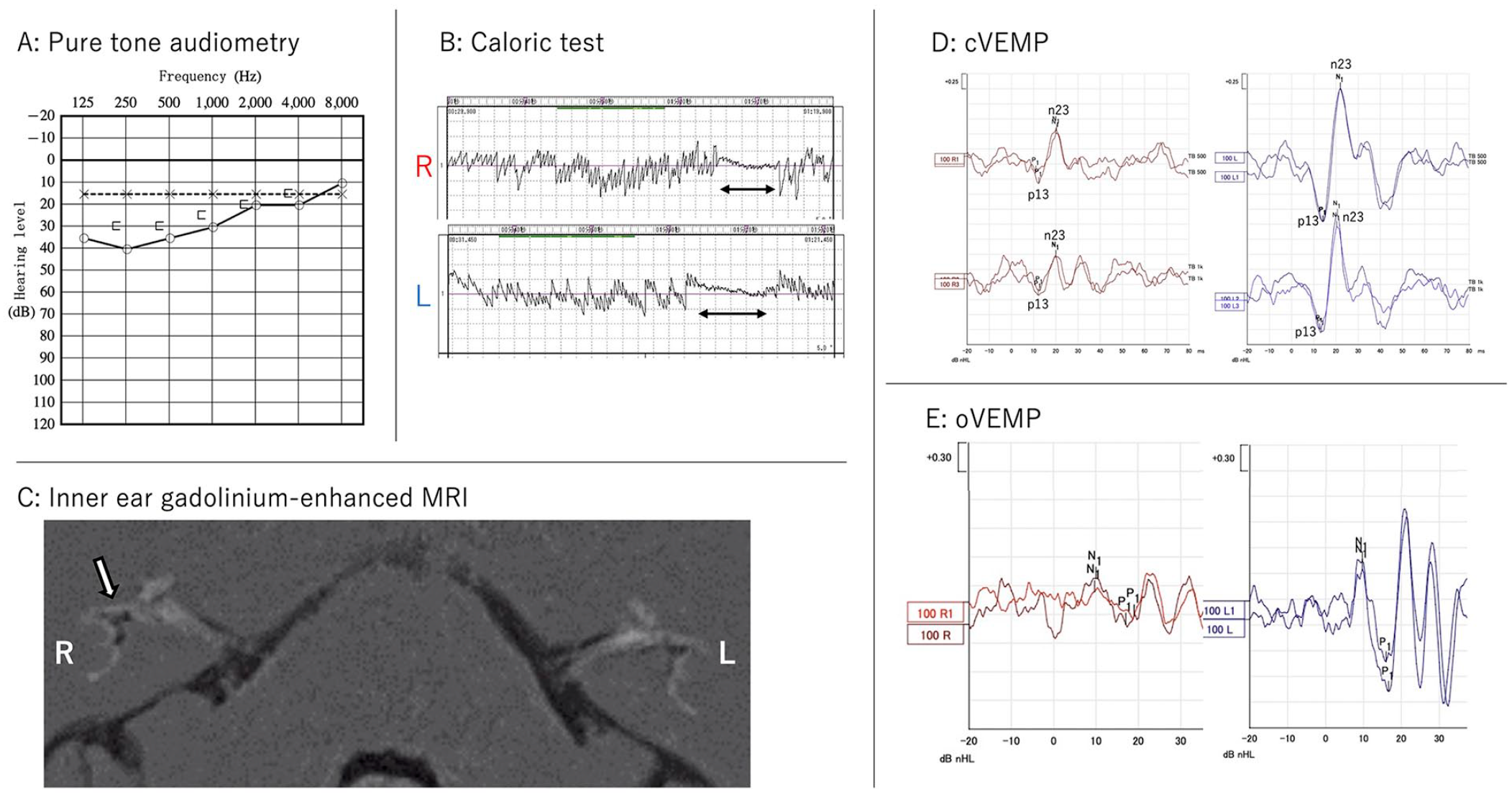
Results of neurotologic examinations before the administration of CGRP receptor inhibitor.
The patient was diagnosed with probable MD, and VM was suspected as some of her dizziness was associated with headaches. Daily oral administration of Goshuyuto, a traditional Japanese Kampo of which effectiveness against migraine and tension-type headaches had been reported, 9 was initiated as a treatment for migraine because dizziness, fullness of ear, and headache were not relieved by prior MD medication. Dizziness and headache were alleviated to some extent in 3 months; however, the symptoms flared again after 6 months. She was then referred to a headache specialist in the Department of Neurology and re-diagnosed with migraine without aura. At that time, the patient was diagnosed with VM because more than half of her dizziness was associated with headaches. Additional treatment with lomerizine and valproic acid relieved the symptoms, although she needed to take rizatriptan benzoate 7 times in a month. She then received a subcutaneous injection of erenumab (70 mg/month); subsequently, both dizziness and headaches decreased promptly and almost disappeared within 2 months. The patient was mildly symptomatic for 1 year with continuous administration of erenumab, valproic acid, and a reduced amount of lomerizine without adverse events.
Self-perceived impairment in daily life also improved, and the Dizziness Handicap Inventory, Migraine Disability Assessment (MIDAS), and Headache Impact Test (HIT-6TM) before and after the administration of the CGRP receptor inhibitor were 58/8, 57/9, and 66/42, respectively.
Pure-tone audiometry, cVEMP, oVEMP, and gadolinium-enhanced inner ear MRI performed again after treatment with erenumab revealed no improvement compared with those performed before treatment (Figure 2).
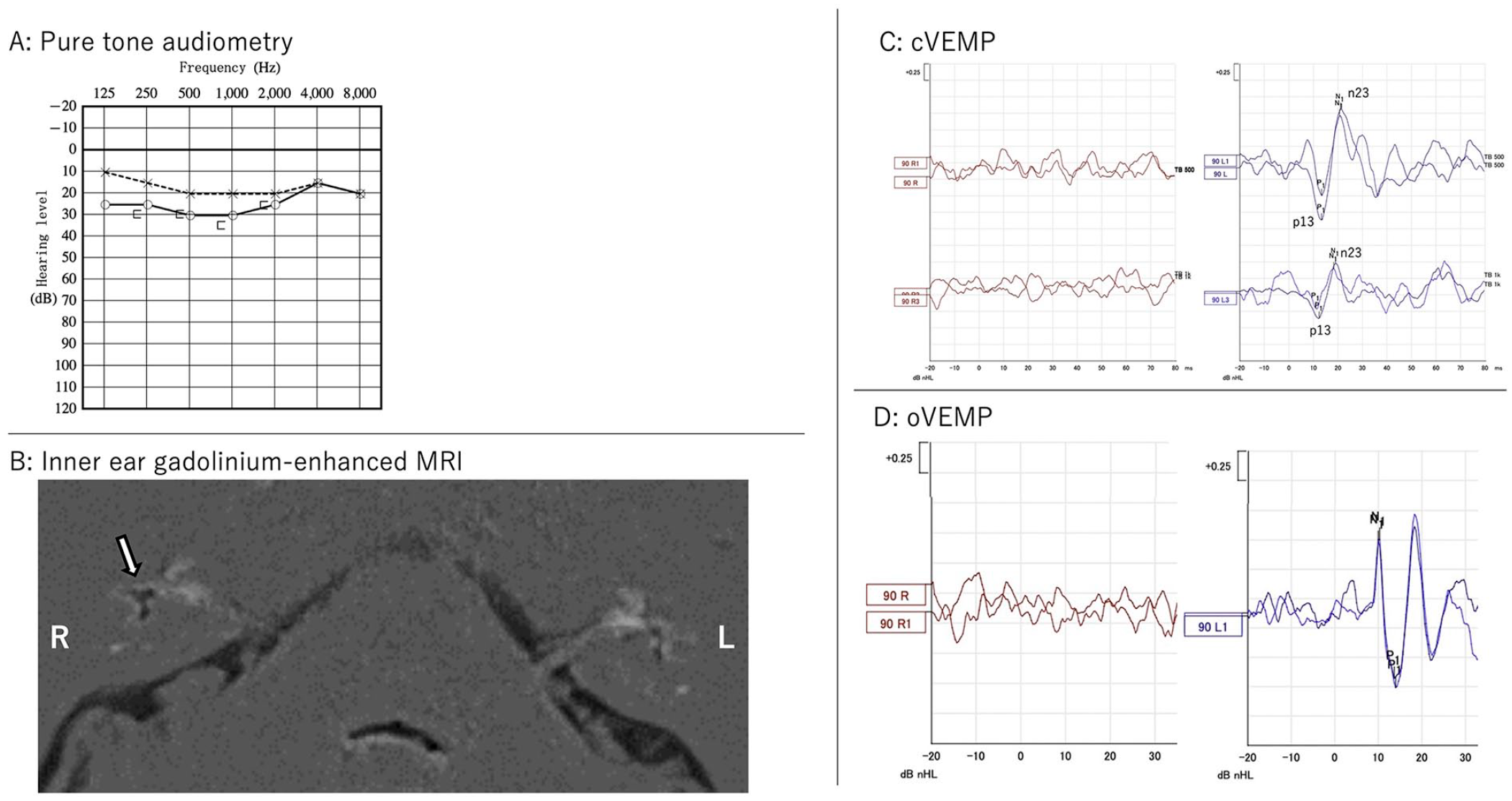
Results of neurotologic examinations after the administration of CGRP receptor inhibitor.
Discussion
A treatment strategy for VM remains unclear. This is the first literature report of vestibular examinations before and after the successful treatment of VM with CGRP receptor inhibitor. The effect of erenumab on our patient and the detailed investigation of vestibular function may provide insights related to understanding the etiology and treatment.
In addition to acute treatments of migraine with medication such as triptans, preventive treatment should be considered when acute management is insufficient. Goshuyuto, a Japanese Kampo medicine, is reported to be a suitable alternative for migraine prophylaxis although the mechanism of its action could not be elucidated. 9 Goshuyuto showed some efficacy on both headache and dizziness in our patient.
Although the pathophysiology of VM remains largely unknown, there are several theories related to sensory hypersensitivity, altered multisensory processing, trigeminovascular, and CGRP effects in the vestibular system. CGRP, a neuropeptide involved in the efferent synapses of hair cell organs such as the cochlea, semicircular canal, and lateral line, has also been investigated in the pathogenesis of VM. 10 While many real-world reports on CGRP-targeted therapies point to the availability of various migraine symptoms, including nausea and vomiting, very few articles have focused on vertigo or dizziness. Recently, 2 studies reported the effects of anti-CGRP medications on VM.5,6 Hoskin et al 5 have reported the improvement through self-evaluation in their retrospective study, and Russo et al 6 have reported that 80% of patients with VM had at least 50% simultaneous reduction in migraine days, vertigo days, and MIDAS score by anti-CGRP monoclonal antibodies in their prospective study. However, to the best of our knowledge, no study has evaluated the effects of anti-CGRP medications on vestibular function.
Assessing what the CGRP receptor inhibitor affected in our case may help us understand VM pathology. The patient was diagnosed with VM and concomitant probable MD. However, she had never noticed hearing loss and the auditory and vestibular dysfunctions did not subside after anti-CGRP treatment. Hu et al 11 reported that the recovery of otolith dysfunction was seen in either cVEMP or oVEMP in all 5 cases with MD. We think this is because the principal clinical condition of the case was not MD, but VM, or the inner ear dysfunctions were irreversible. Although it is difficult to disclaim the effects against MD completely, it seems more natural to interpret that the anti-CGRP monoclonal antibodies ameliorated the VM symptoms in the reported case.
We hypothesized 2 pathologies that could explain why vestibular symptoms were observed in our patient by referring to previous reports: (1) blocking CGRP in the trigeminal ganglion suppressed the effect of CGRP on the vestibular nucleus, or (2) blocking CGRP revealed temporal change of the amount of blood perfusion in the inner ear. Regarding hypothesis (1) Zhang et al 12 reported the possibility of trigeminal-mediated sensitization of vestibular nucleus neurons in migraine, which may be a primary pathophysiological process underlying vestibular sensitivity in migraine patients with vestibular symptoms. They also reported that blocking CGRP in the trigeminal ganglion may relieve vestibular symptoms in migraines. In contrast, regarding hypothesis (2) the presence of CGRP in trigeminal sensory fibers innervating the inner ear and vestibular nuclei has been reported. 13 The pathophysiology of VM is proposed as follows: inner ear plasma extravasation and the release of inflammatory mediators, subsequent to neurogenic inflammation triggered by the activation of the trigeminal-vestibulocochlear reflex, cause vasodilation of the inner ear blood vessels, leading to cochlear/vestibular hypersensitivity, and then vestibular dysfunction. 10 At the same time, the hypoperfusion of the inner ear is also considered based on several studies that reported reduced or absent VEMP responses in patients with VM. Despite showing clear amelioration of dizziness, our patient did not exhibit any improvement in vestibular examinations conducted through stimulation of the peripheral vestibular organs and inner ear MRI. Based on these results, the effect of the CGRP receptor inhibitor on the vestibular nuclei through blocking CGRP in the trigeminal ganglion was more plausible in our case.
However, as this is a case report, it is not possible to conclusively determine VM pathology and reject the second hypothesis or other conditions. It is reported that the placebo effects should be considered as a distinct possibility in migraine prophylaxis, especially with the more elaborate and impressive treatment rituals. 14 Furthermore, it is well-established that VM and MD can coexist, and even EH can be present in VM. 15 Our patient was diagnosed with both probable MD and VM, although the signs of EH did not change on MRI after the treatment. Further studies are needed to investigate the effects on EH by anti-CGRP treatment. Findings from such studies with a higher number of cases, especially the pure VM cases, could improve our understanding of the etiology of VM and aid in the development of effective treatment strategies in the future.
Conclusion
This is the first literature report of vestibular examinations before and after the successful treatment of VM with CGRP receptor inhibitor. The vestibular dysfunctions shown in vestibular examinations revealed no change compared with those observed before treatment, although headache and dizziness have improved after administration of erenumab. Although further case series studies are needed, this case suggests the possibility that VM may be treated by blocking CGRP in the trigeminal ganglion, which suppresses the effects on the vestibular nucleus.
Footnotes
Data Availability Statement
The raw data of the reported case will be made available by the authors, without under reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Japan Society for the Promotion of Science Grant (JSPS KAKENHI Grant #22K09693).
Ethics Statement
This case report was exempt from review by the ethics committee of our institute.
Informed Consent
Written informed consent was obtained from the patient for publication on this case report and accompanying images.