
Abstract
Background:
Vestibular migraine is a common cause of vertigo. Intervention often includes preventive and/or rescue medications. Lifestyle modifications are often used along with medications but can be used as the sole intervention. There is lack of clarity regarding the long-term benefits of these interventions.
Aims:
The purpose of this study was to determine long-term effects of intervention types on dizziness in patients with vestibular migraine.
Methods:
Twenty-three participants were grouped based on intervention into preventive medication plus lifestyle modifications, rescue medication plus lifestyle modifications, or lifestyle modifications only. Outcomes were determined at ~372 days post intervention by comparing pre- and post-Dizziness Handicap Inventory scores. A difference of ≥18 points was considered a change and we also evaluated change in severity scale on this measure.
Results:
Using the group mean change score, only the rescue medication plus lifestyle modification group was significantly improved at 372 days of intervention. Considering all individual participants, 30% of the participants had improvement in dizziness at this point, regardless of intervention. Fifty percent of the rescue medication plus lifestyle modification group had significant reduction in dizziness, while the preventive medication plus lifestyle modification and the lifestyle modification only groups performed similarly using this criterion. Considering change in severity category, 43% of all participants improved by at least one category. The rescue medication plus lifestyle modifications and the lifestyle modifications only groups performed similarly with 50% of their respectively groups exhibiting improvement by at least one category. Notably, there was no worsening of dizziness for any participant in the lifestyle modification only group.
Conclusion:
Our findings suggest that improvement in dizziness is maintained at ~372days of intervention in patients with vestibular migraine. Intervention using rescue medications plus lifestyle modifications had the best outcomes, followed by lifestyle modifications only. There was no worsening in dizziness for the lifestyle modification only intervention. More work is needed to better understand intervention effects, but it is encouraging that effects are maintained at greater than one year.
Introduction
Vestibular migraine (VM) is one of the most common causes of episodic dizziness, 1 with a prevalence of 4.3% to 29.3% depending on diagnostic criteria and population. 2 Intervention includes medication for preventive or rescue use, with 91% of patients receiving a prescription after initial evaluation. 3 However, variability exists in medications prescribed and in treatment outcomes.4-6 Interventions also frequently include lifestyle modifications, in conjunction with medication or in isolation.1,7-9
Although most interventions report improvement for their participants, the follow-up time periods vary across and within investigations.8,10 Measuring treatment effects at similar follow-up points and for longer periods of time is important to ensure benefit is maintained. The purpose of this study was to determine long-term effects of intervention types on dizziness in patients with VM. Based on prior evidence, we hypothesized that groups receiving medication plus lifestyle modifications would demonstrate the greatest reduction in dizziness symptoms over the long-term.
Methods
Participants
Following Institutional Review Board approval (#200680), we recruited patients diagnosed with VM and who were provided lifestyle modifications as part of their treatment, either in isolation or along with medication (preventive or rescue). Chart review was completed to identify English-speaking adults 18 years and older who met inclusion criteria. Forty-one patients meeting the criteria were contacted and 23 agreed to participate. Participant information is shown in Table 1.
Demographic, Medication, and Dizziness Handicap Inventory (DHI) Results for Each Participant and Group.
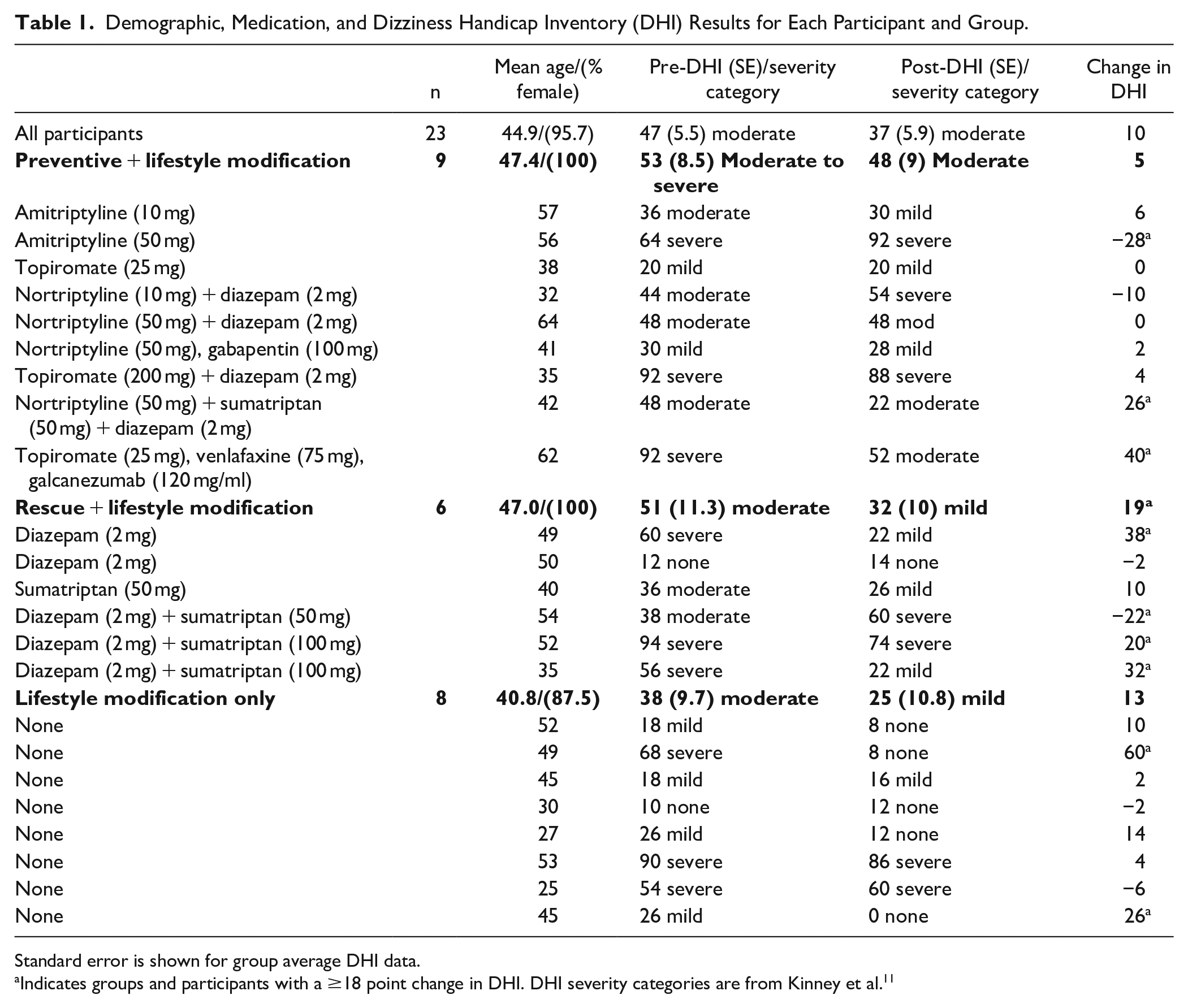
Standard error is shown for group average DHI data.
Indicates groups and participants with a ≥18 point change in DHI. DHI severity categories are from Kinney et al. 11
Participants were divided into 3 groups based on their intervention: Preventive + Lifestyle Modification (PLM), Rescue + Lifestyle Modification (RLM), and Lifestyle Modification Only (LMO). Table 1 lists medications and dosages. The PLM group took daily medication. Six participants in this group only had 1 preventive medication throughout the course of the study, whereas 2 participants used more than 1 preventive medication, discontinuing 1 prior to starting the next. Four participants in the PLM group were also prescribed diazepam or sumatriptan for rescue needs. The RLM group only used diazepam and/or sumatriptan as needed. The LMO group did not take any medication for symptoms of VM. All participants were provided the lifestyle modification intervention detailed in Roberts et al. 9
Procedures
Participants completed the Dizziness Handicap Inventory (DHI) at their initial clinic visit. 12 Post-intervention DHI was completed via REDcap online survey. Follow-up data was collected an average of 371.5 (standard deviation = 43.9; range = 321-468) days post-intervention, allowing for assessment of long-term effects of each intervention.
The DHI is a 25-item assessment that evaluates self-perceived handicap related to symptoms of dizziness. The DHI items are answered with “yes,” “sometimes,” or “no.” Total points are summed with higher scores indicating more severe dizziness handicap. Severity categories developed by Kinney et al 11 were also considered in the current study with 0 to 14 representing no handicap, 16 to 34 mild handicap, 36 to 52 moderate handicap, and greater than 54 severe handicap.
Results
Pre- and post-intervention scores for the DHI are shown for each participant and group in Table 1. Mean pre-intervention DHI scores were moderate-severe for the PLM group and moderate for the RLM group. The mean total DHI score was also in the moderate severity category for the LMO group but was borderline moderate. An 18-point change is often used as the cut-off for significant change when total score is considered. 12 Overall, the mean total score decreased 10 points from 47 to 37 points. The PLM group changed by only 5 points and the LMO group changed by 13 points. However, the RLM group changed by 18.6 points, indicating a significant improvement for this group and intervention using the DHI total score consideration.
Across all participants, 7 individuals had a ≥18 point improvement in DHI total score. Two were in the PLM group, 3 in the RLM group, and 2 in the LMO group. These results are expressed as percentages in Figure 1. Only 2 participants had ≥18 point worsening in symptoms. One was in the PLM group and 1 was in the RLM group; no participant had worse dizziness post-intervention in the LMO group. These results indicate the RLM group was the most successful using this criterion with 50% of participants improving by ≥18 points and only 1 participant experiencing worse dizziness.
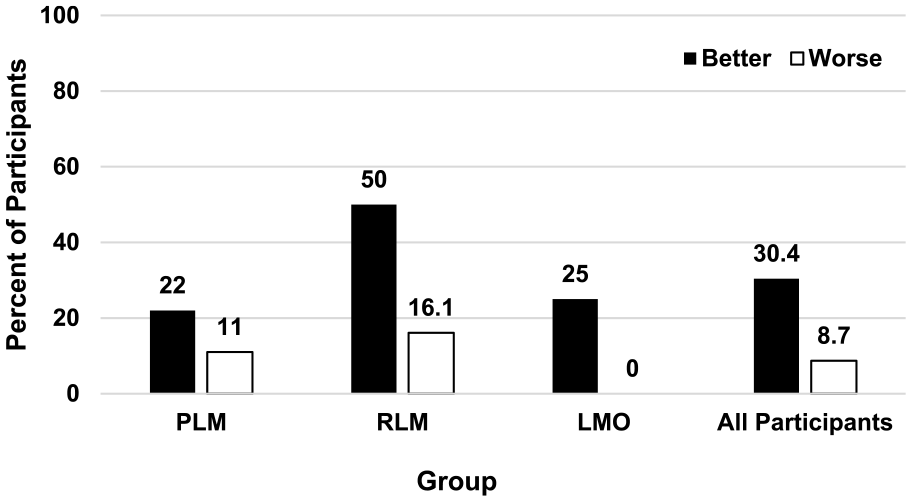
Percent of participants by group that had improved or worsened dizziness measured with the Dizziness Handicap Inventory (DHI) ≥18 point change criterion. Pre-intervention total DHI score was compared to post-intervention score obtained after ~371 days.
We also considered post-intervention change in DHI severity category, displayed in Figure 2. Across participants, 10 improved by at least 1 category post-intervention, and 2 worsened by at least 1 category. Within the PLM group and the RLM group, 3 improved and 1 worsened. For the LMO group, 4 improved and none worsened.
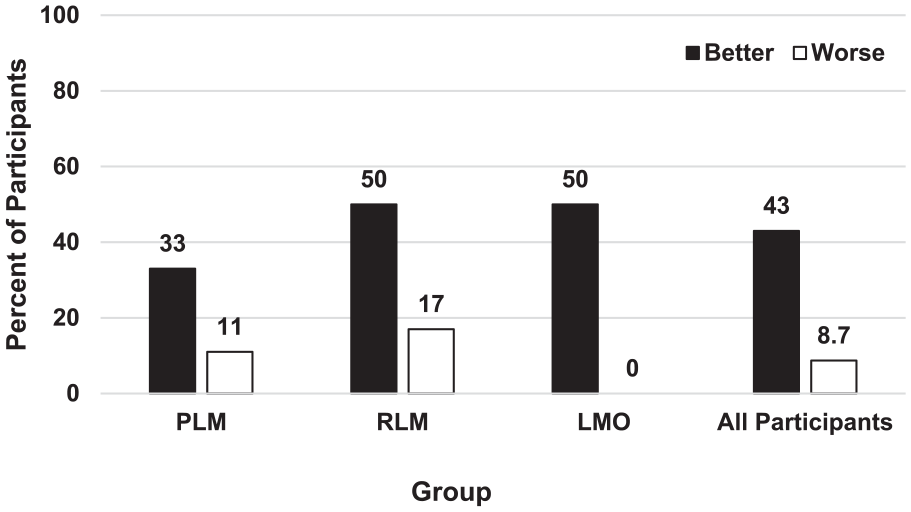
Percent of participants by group that had improved or worsened dizziness determined by a change in Dizziness Handicap Inventory (DHI) severity category. Pre-intervention DHI severity category was compared to post-intervention severity category obtained after ~371 days.
Discussion
The purpose of this investigation was to determine the long-term (~372 days) effects of interventions including medications and lifestyle modification on dizziness handicap for participants with VM. We considered both change in DHI total score with a criterion of ≥18 points as well as change in severity category to evaluate intervention effects. Using this approach, 30.4% to 43% of participants reported improvement in dizziness long-term. The RLM intervention group performed the best with 50% of participants reporting improvement and only—approximately 17% reporting worsened dizziness. The LMO group performed next best with 25% to 50% of participants reporting improvement and no worsening in dizziness. The PLM group still had participants with improvement, but this ranged from 22% to 33% with 11% reporting worsened dizziness.
Follow-up periods of about 90 to 120 days after intervention are common.4,5 While Celik et al 10 did follow patients for 180 to 960 days post-intervention, the follow-up period varied for each participant. Reploeg and Goebel 8 had a follow-up period more like the current report with a mean ~382 days. However, their range was large and included times as short as ~28 days. Comparison with other long-term data is challenging given these issues.
This is a preliminary investigation and there is an obvious limitation of number of participants per group. Still, the results are encouraging and support moving forward with an investigation of larger scale. In addition to disease-specific measures like DHI, future work should also include a generic measure of health state like the EQ-5D. 13 Generic measures not only allow for comparison among different diseases but a tool like the EQ-5D provides additional information on multiple dimensions including mobility, self-care, activities, pain/discomfort, and anxiety/depression. This information could prove valuable in helping to identify which individuals would be expected to perform optimally with varied interventions.
Conclusions
Positive treatment outcomes for VM-related dizziness can be measured at periods exceeding 1 year using validated tools (DHI), suggesting long-term effectiveness of the interventions. In the current report, rescue medications plus lifestyle modification produced the best results, followed by lifestyle modifications only. Preventive medication plus lifestyle modification had the third best results but it is possible these participants were more complex, given the need to trial various medications during intervention. The positive outcomes observed at such a long follow-up period coupled with the low risk of worsening symptoms is encouraging. Based on these initial data, we hypothesize that lifestyle medications are an effective solution for long-term reductions in DHI for about half of people with VM, especially when combined with rescue medication. Additional work is needed to better understand which intervention method should be used for specific patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
Portions of this work were completed by Courtney Kolberg as a part of her capstone project at Vanderbilt University School of Medicine. Portions of this work were presented at the 2022 meeting of the American Balance Society in Scottsdale, AZ, and at the 2022 meeting of the American Academy of Audiology in St. Louis, MO.