
Abstract
Epidermoid inclusion cysts are rare in the oral cavity, accounting for less than 0.01% of cysts found there. These cysts are defined as epidermoid if they contain only epithelial lining, dermoid if skin appendages, and teratoid if they contain other tissues such as muscle, cartilage, and bone. This case report describes a case of a plunging ranula that was later diagnosed as an epidermoid inclusion cyst. The patient is a 22-year-old male who presented with swelling in the floor of the mouth and difficulty eating solid foods for the past 4 months. Upon examination, a shiny, pink-colored mass measuring 1 cm × 5 cm was observed, which displaced the tongue upward and backward. MRI scan of the brain, face, and neck revealed a well-defined, non-enhancing cystic mass measuring 6.6 cm × 4.5 cm that extended beyond the sublingual area. Histopathological examination after surgical removal of the cyst revealed that the cyst wall was lined with stratified squamous keratinized epithelium with a retained granular layer, and the cavity was filled with lamellated keratin flakes. The patient recovered well after surgery; no recurrence was observed at the 6-month follow-up.
Keywords
Introduction
Epidermoid cysts are slow-growing benign lesions that can appear anywhere on the body. Only about 7% of cases include the head and neck, while 1.6% include the oral cavity. 1 Dermoid and epidermoid cysts in the mouth make up less than 0.01% of all oral cysts. 2 They are very rare.
There are 3 types of cystic lesions: epidermoid, dermoid, and teratoid; when the lining only contains epithelium, cysts are said to be epidermoid, dermoid cysts when skin adnexa (hair follicles, sweat glands, sebaceous glands) are found and all 3 germinal layers—ectoderm (skin, hair, teeth), mesoderm (skeletal muscle, vasculature, central nervous system, peripheral nerves), and endoderm—must be present in teratoid cysts’ walls (thyroid, GI tract components, lung, liver). 3
There are many theories about what causes these cysts in the mouth. Epidermoid cysts, which are just choristomas, are said to be caused by the sequestration of surface ectoderm at bone suture lines or along the lines of embryonic closure. Another manifestation of these tumors is orbital inflammation following forceful trauma or surgical/accidental events. A third idea is that this cyst could be a type of thyroglossal duct cyst.4 -6 These cysts in the oral cavity can occasionally cause severe problems with difficulty in swallowing, chewing, and speaking. 7 This case report presents an interesting case of a sublingual epidermoid cyst, which was first presented as a plunging ranula. The case report adheres strongly to the CARE guidelines. 8
Case Presentation
A 22-year-old male from Larkana, Jacobabad, presented to Civil Hospital Karachi with a sublingual swelling that appeared 4 months ago. He experienced dysphagia for 20 days and dyspnea for 7 days. He had an unremarkable medical and surgical history and no family history of the same illness or comorbidities. The patient had normal appetite, micturition, bowel habits, and sleep with no addictions. However, his socioeconomic history was unsatisfactory, and his transfusion history was unremarkable. Figure 1 shows a preoperative photograph of the sublingual cyst occupying the oral cavity.

A preoperative photograph of the sublingual cyst occupying the oral cavity.
On examination, the patient had a sublingual cyst, pushing the tongue superiorly and posteriorly, obscuring its view. The cyst was dark pinkish in color with shiny mucosa and extended externally up to the level of the hyoid bone. Palpation revealed a single swelling on the floor of the mouth under the tongue and up to the level of the hyoid bone. The surface was smooth with well-defined margins. It was firm, nontender, and immobile, and it was nonpulsatile, non-fluctuant, and non-transilluminant. No palpable lymph nodes or other neck swelling were noted. On plain MRI scan of the brain, face, and neck, a 6.6 cm × 4.5 cm circumscribed non-enhancing cystic mass extending beyond the sublingual area was observed. Figure 2a and 2b demonstrate MRI imaging of the patient.
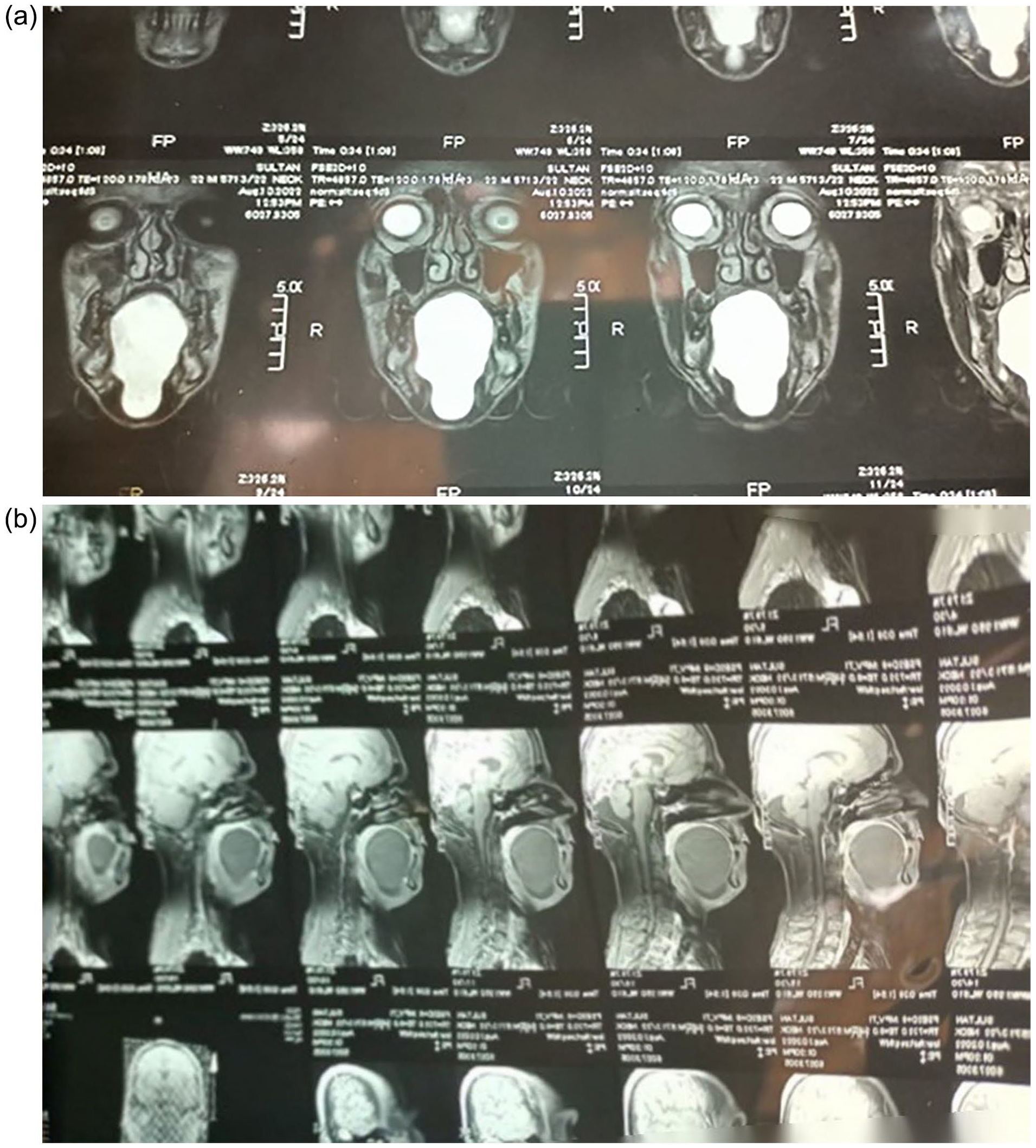
(a) and (b) demonstrate plain MRI scans of the brain, face, and neck.
The patient underwent surgical removal of the mass under general anesthesia and with nasotracheal intubation. A horizontal incision was made in the submental area, precisely 2 cm below the mandible. The cyst was then carefully separated from the adjacent tissues and excised. The intraoperative images of the transcervical and transoral approaches are depicted in Figure 3a and b, respectively. Figure 4 shows the excised epidermoid cyst.
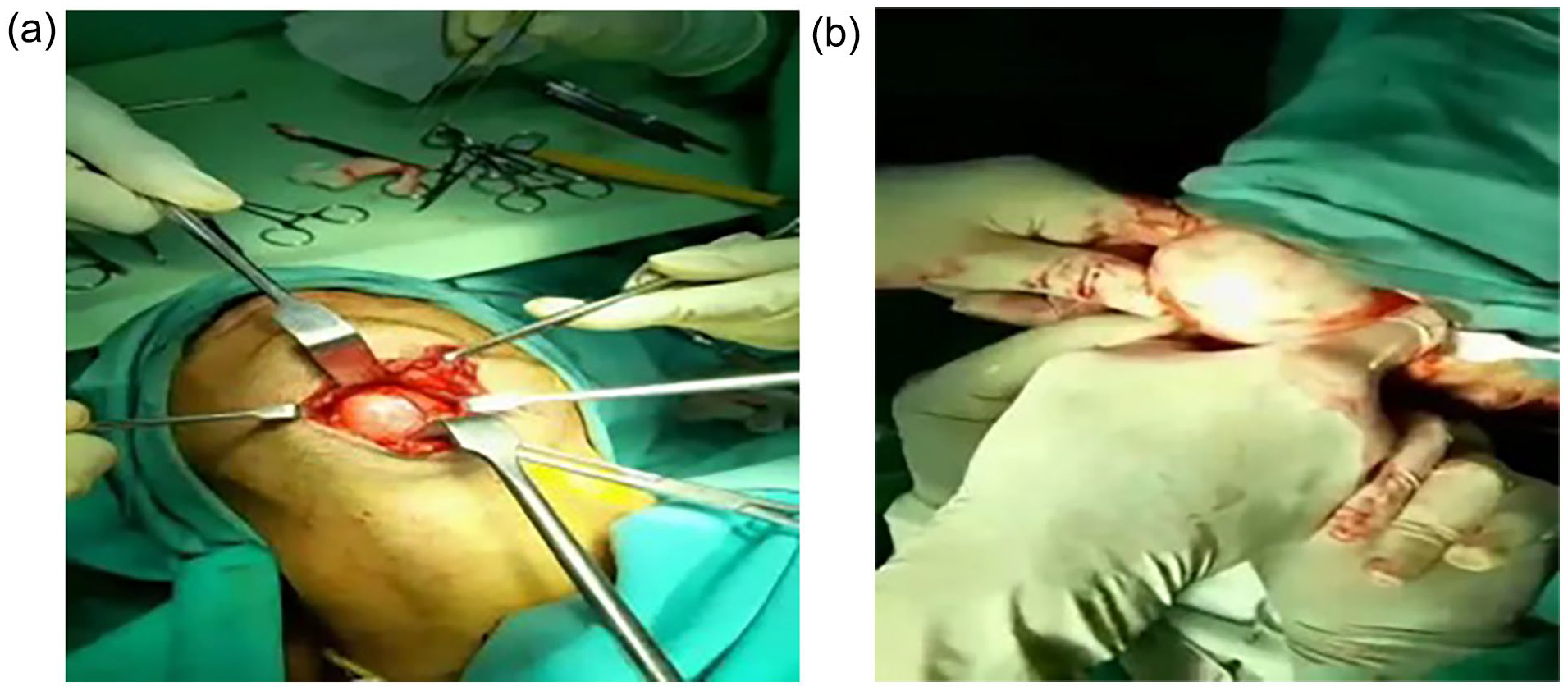
(a) Intraoperative picture showing transcervical approach and (b) intraoperative picture showing transoral approach.

The image displays the excised epidermoid cyst, which has its intact capsule, placed on a table.
Upon histopathological examination, the cyst wall was lined with stratified squamous keratinized epithelium, which retained a granular layer. Additionally, the cavity was found to be filled with lamellated keratin flakes. The patient’s postoperative period was uneventful, and there was no evidence of recurrence during the 6-month follow-up. Figure 5 shows disappearance of the swelling under the tongue of the patient on the sixth post operative day.
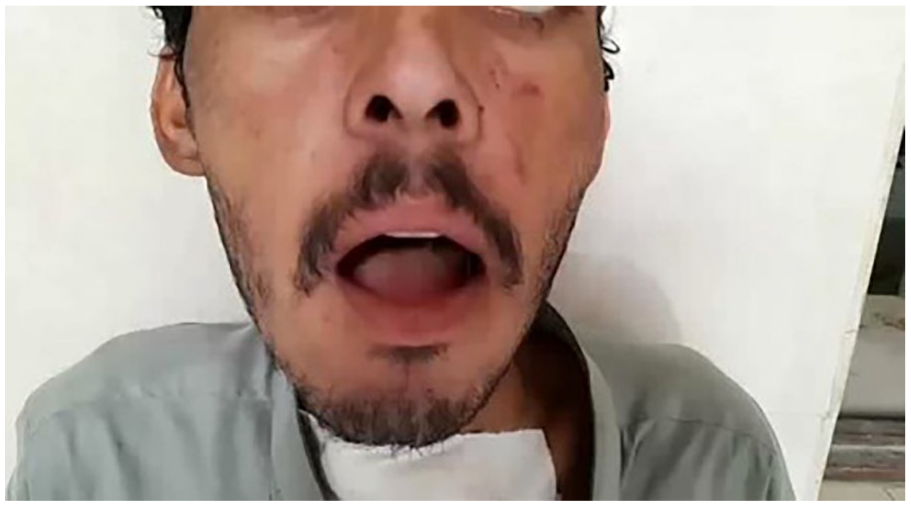
The image illustrates the disappearance of the swelling under the tongue on the sixth day after the operation.
Discussion
Epidermoid cysts are benign cysts found anywhere on the body, with prime locations being embryonic fusion sites. Based on their development, epidermoid cysts are classified into 2 types: congenital and acquired. Congenital epidermoid cysts manifest ectodermal components trapped between the first and second branchial arches during the third and fourth weeks of intrauterine life. The acquired variety—is a consequence of either traumatic or iatrogenic inclusion of ectoderm or the blockage of a sebaceous gland duct. Epidermoid and dermoid cysts account for less than 0.01% of all cysts in the oral cavity. 9
In the case reported above, subjective symptoms initially evolved in the early thirties, and no history of trauma or inflammation was inferred, labeling the cause as idiopathic. Surgical excision is heralded as the modality of choice for cysts such as these, despite the existing risk of recurrence in cases where the capsule is not correctly salvaged. However, this complication can be successfully avoided, given the accurate removal of the cyst. 10
The cysts may be categorized based on their anatomical proximity to the muscles of the floor of the mouth. They are referred to as submental (located between geniohyoid and mylohyoid muscles), sublingual (situated above mylohyoid and genioglossal muscles), and submandibular (positioned laterally to the musculature). 11
Based on the findings of our examination, the cyst was situated superior to the mylohyoid muscle, indicating its classification as a sublingual cyst. Epidermoid cysts may manifest in various regions of the oral cavity, including superior to the mylohyoid and geniohyoid muscle (A), amidst the mylohyoid and geniohyoid muscle (B), and inferior to the mylohyoid and geniohyoid muscle (C).12,13
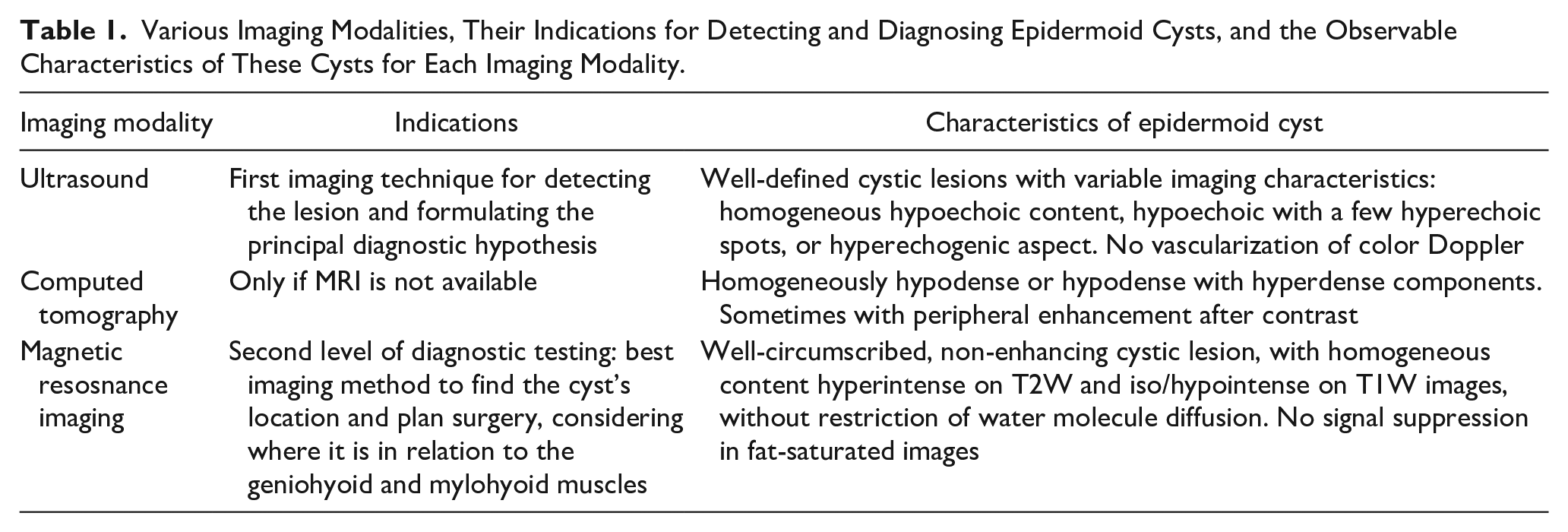
The findings of Basla et al.’s 12 study shed light on the appropriate indications for utilizing various imaging modalities in the evaluation of the iconographic characteristics of epidermoid cysts. The MRI is a fundamental technique due to its multiplanar capabilities and superior soft tissue contrast. It offers essential insights into the content, extension, and topographic relationships of these lesions. Table 1 describes different imaging modalities, their indications for detecting and diagnosing epidermoid cysts, and the characteristics of these cysts as observed in each modality.
Various Imaging Modalities, Their Indications for Detecting and Diagnosing Epidermoid Cysts, and the Observable Characteristics of These Cysts for Each Imaging Modality.
Complete surgical excision is a relatively uncomplicated option and remains the only effective treatment. The approach is contingent on the size and location of the lesion, with the choice between extraoral or intraoral incision depending on the position of the lesion in relation to the muscles of the floor of the mouth (primarily mylohyoid and geniohyoid).12,14 The extraoral approach is generally preferred in the case very large sublingual cysts, whereas the intraoral approach is used for smaller sublingual cysts. 15
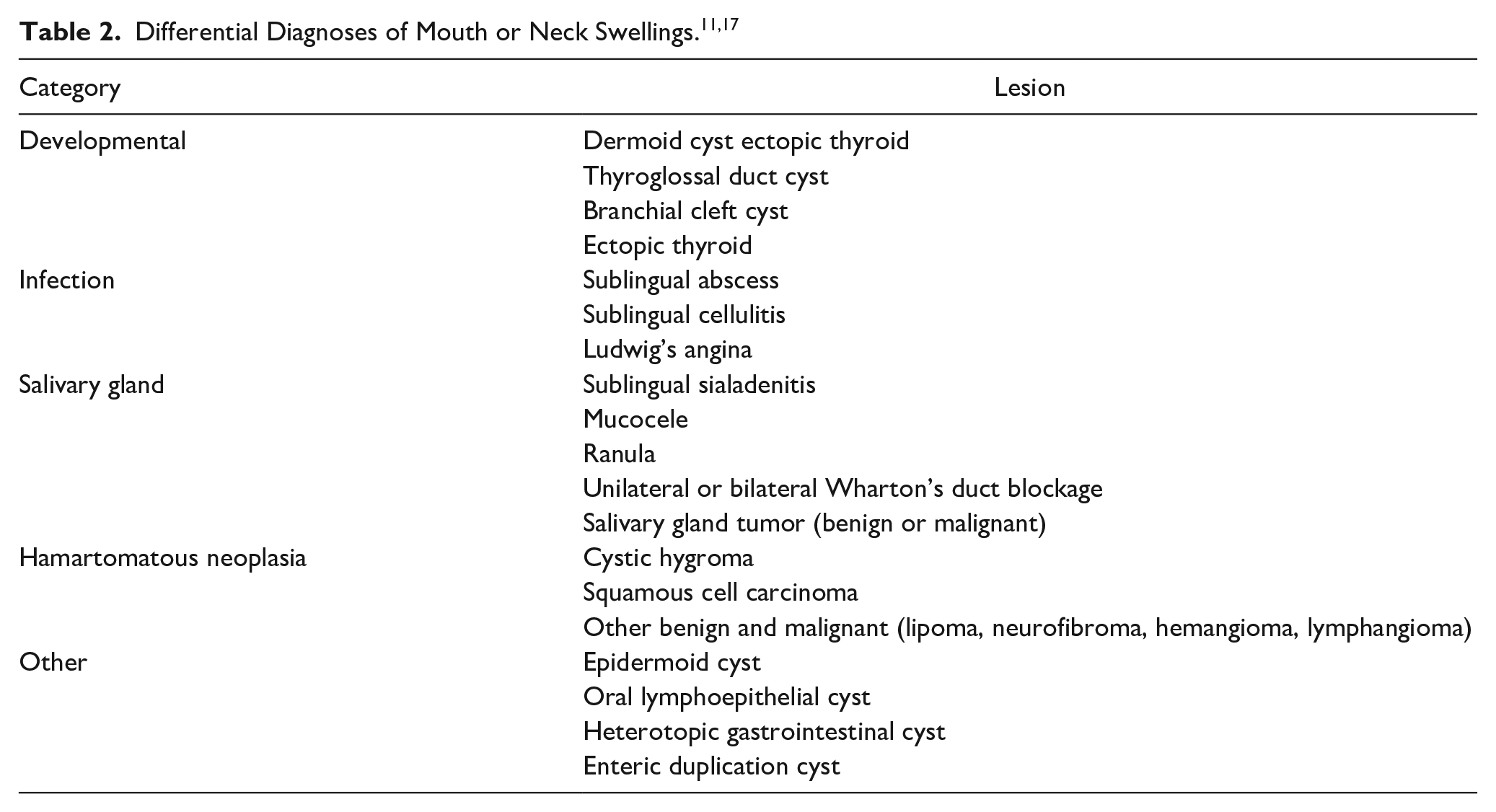
A possible differential diagnosis for sublingual lesions encompasses ranula, lymphatic malformation, dermoid cyst, epidermoid cyst, and heterotopic gastrointestinal cyst. The utilization of bimanual palpation and conventional radiography may not always provide adequate information for establishing differential diagnoses. In such instances, it is imperative to employ ultrasonography, CT scan, or MR imaging in conjunction with histopathology examination via fine-needle aspiration biopsy. Based on the CT scan, the lesion was initially diagnosed as a ranula. However, after conducting a histopathology examination, it was determined to be an epidermoid cyst. Further, all other potential sublingual lesions were eliminated as possibilities through the use of histopathology and CT scan. We opted for an intraoral approach in our patient, as the cyst was readily accessible through this route and was successfully excised. 16 Table 2 show differential diagnoses of mouth or neck swellings modified from Hikasa et al.11,17
Conclusion
In this case report, a 22-year-old male presented with a swelling below the tongue that was diagnosed as a sublingual epidermoid cyst. Epidermoid cysts are rare in the oral cavity, and their etiology can be congenital or acquired. Surgical excision is the preferred treatment, although proper removal of the cyst capsule is essential to prevent recurrence. Overall, this case highlights the importance of considering epidermoid cysts as a differential diagnosis for sublingual swellings and emphasizes the effectiveness of correct imaging modalities and surgical intervention in managing such cases.
Footnotes
Acknowledgements
The authors are very appreciative to the patient for the opportunity to learn as well as thankful to the hospital for providing support for completing this report.
Authors’ Contributions
Javeria: Responsible for conceptualization, writing the original draft, granting final approval, ensuring the accuracy of the work, and overseeing the review and editing process. Hussain Haider Shah: Involved in conceptualization, writing the original draft, granting final approval, and ensuring the accuracy of the work. Muskan Seher: Responsible for writing the original draft, granting final approval, and ensuring the accuracy of the work. Khubeb Yousif Shiakh: Involved in writing the original draft, reviewing, and editing. Zeba Ahmed: In her capacity as a senior doctor, responsible for writing the original draft, reviewing, and editing. Dua Rana: Involved in writing the original draft, reviewing, and editing. Syeda Alishah Zehra: Involved in writing the original draft, reviewing, and editing. Arun Subash: Involved in reviewing and editing.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statements
Our institution does not require ethical approval for reporting individual cases or case series.
Consent Statements
Informed patient consent was obtained for publication.
Provenance and Peer Review
Not commissioned, externally peer reviewed.
Written Informed
Written informed patient consent was obtained for publication.