
Abstract
Background:
Ultrasound (US) has been supported as a preferred imaging technique to evaluate neck masses suspicious for plunging ranula, but to date, there have been no reports addressing the role of adjunctive sonopalpation.
Objectives:
In this proof-of-concept technical case series, we describe the technique of sonopalpation and provide surgical and pathological correlates.
Methods:
Patients with surgically-treated plunging ranula were identified from the senior author’s case log. Three patients were included in a retrospective chart review targeting imaging results, surgical findings, and final pathology results.
Results:
US with sonopalpation identified anatomy consistent with plunging ranula in all 3 cases. These findings were confirmed surgically and pathologically.
Conclusion:
US with sonopalpation was effective in demonstrating anatomic abnormalities consistent with plunging ranula. Sonopalpation helped define relationships between the sublingual gland, ranula fluid, and the frequently-associated mylohyoid dehiscence. Sonopalpation is a useful adjunctive technique to standard US in the evaluation of plunging ranula. Additional investigation into this technique may be helpful in further evaluating its use in the diagnostic process.
Introduction
A plunging ranula is an extravasation sublingual gland pseudocyst that commonly presents as a painless cystic neck swelling. Plunging ranulas are uncommon and may be difficult to discriminate from alternative diagnoses such as lymphangioma or dermoid. 1 Computed tomography (CT) and magnetic resonance imaging (MRI) of a plunging ranula generally identifies well-defined, homogenous, non-enhancing cystic mass characteristically located in the submandibular space that may extend to the sublingual or parapharyngeal space. 2 Yun et al reported the accuracy of CT and MR correctly identifying a plunging ranula, confirmed by intraoperative or histopathological findings, to be 73% and 71%, respectively. 3
These imaging techniques may identify the “tail sign” as a smooth tract that extends from the lesion at the posterior edge of the mylohyoid muscle anteriorly into the sublingual space. 4 Although the tail sign is supportive of a diagnosis of ranula, it is not universally identified in patients with ranula. 3 The additional finding of a mylohyoid dehiscence is another acknowledged radiographic finding supporting the diagnosis of plunging ranula. 5
Ultrasound (US) has become a preferred imaging modality to evaluate for plunging ranula due to its availability, absence of radiation, appreciation of dynamic real-time anatomic visualization, and lower cost. 5 Conventional US has been reported to be effective at accurately imaging underlying the anatomy of a plunging ranula but is also acknowledged to often be limited in the visualization of the intraoral components of the lesion due to shielding from the mandible. 3
“Sonopalpation,” as reported by Patel et al to evaluate for submandibular sialolithiasis, improves US imaging of the floor of mouth by delivering floor of mouth structures into the field of view of an US probe applied to the neck. 6 The US operator places their gloved finger into the patient’s mouth and physically displaces structures inferiorly with the probe concurrently directed superiorly. Patel et al identified that the addition of sonopalpation improves sensitivity to detect both the presence and the location of sialoliths in the submandibular gland. 6
To our knowledge, there have been no reports identifying the efficacy of sonopalpation in defining the anatomy associated with a plunging ranula. This technical case series describes the use of US with sonopalpation in the evaluation of plunging ranula.
Materials and Methods
This study was approved by the University of Iowa Institutional Review Board (#202407113). Patients were eligible for inclusion if they were treated surgically for plunging ranula during the designated study period. No formal power analysis was performed due to the rarity of this condition and the proof-of-concept nature of this study. The review of the senior author’s surgical log identified 3 patients who were eligible over a 6 week period ending in June 2024. Chart review analyzed clinical findings, results of US with sonopalpation, and documentation of surgical and pathologic findings.
All imaging with sonopalpation was performed by the senior author (H.H.). The senior author has over 15 years of head and neck US experience with a focus on salivary gland imaging. Images are acquired and stored on the hospital server with subsequent inclusion in each patient’s electronic medical record. The US images are interpreted in front of the patient and again after transfer of the images into the patient chart, leading to a standard dictation template that is used to generate an US report. Salivary US was interpreted by the surgeon performing the US.
US and Sonopalpation Technique
The Toshiba Aplio 500 US unit (Canon Medical Systems, Otawara, Tochigi, Japan), employing the 14-5 MHz linear probe, was used for an US evaluation of the head and neck. The patient is seated and positioned with a tilt of the chin back and laterally, rotated slightly toward the US operator. The right-handed US operator stands to the patient’s right, facing them, holding the transducer with their right hand (Figure 1A). Standard sonopalpation technique was performed with cutaneous application of the probe directed superiorly to the submandibular space, parallel to the lower border of the mandible in a slightly-oblique transverse plane (Figure 1B). The patient is asked to open their mouth and then close gently on the inserted index finger of the examiner to permit the examiner to digitally apply pressure on the lateral floor of mouth and deliver the floor of mouth contents inferiorly into the field of view of the transducer (Figure 1C). Movement of both the finger and the transducer permits video recording of dynamic imaging of the floor of mouth anatomy. Pressure applied to the floor of mouth can be variable and allows for a subjective assessment of compression of muscular and glandular structures. This approach facilitates visualization of differences in adjacent echogenicity and determination of abnormal pathology.
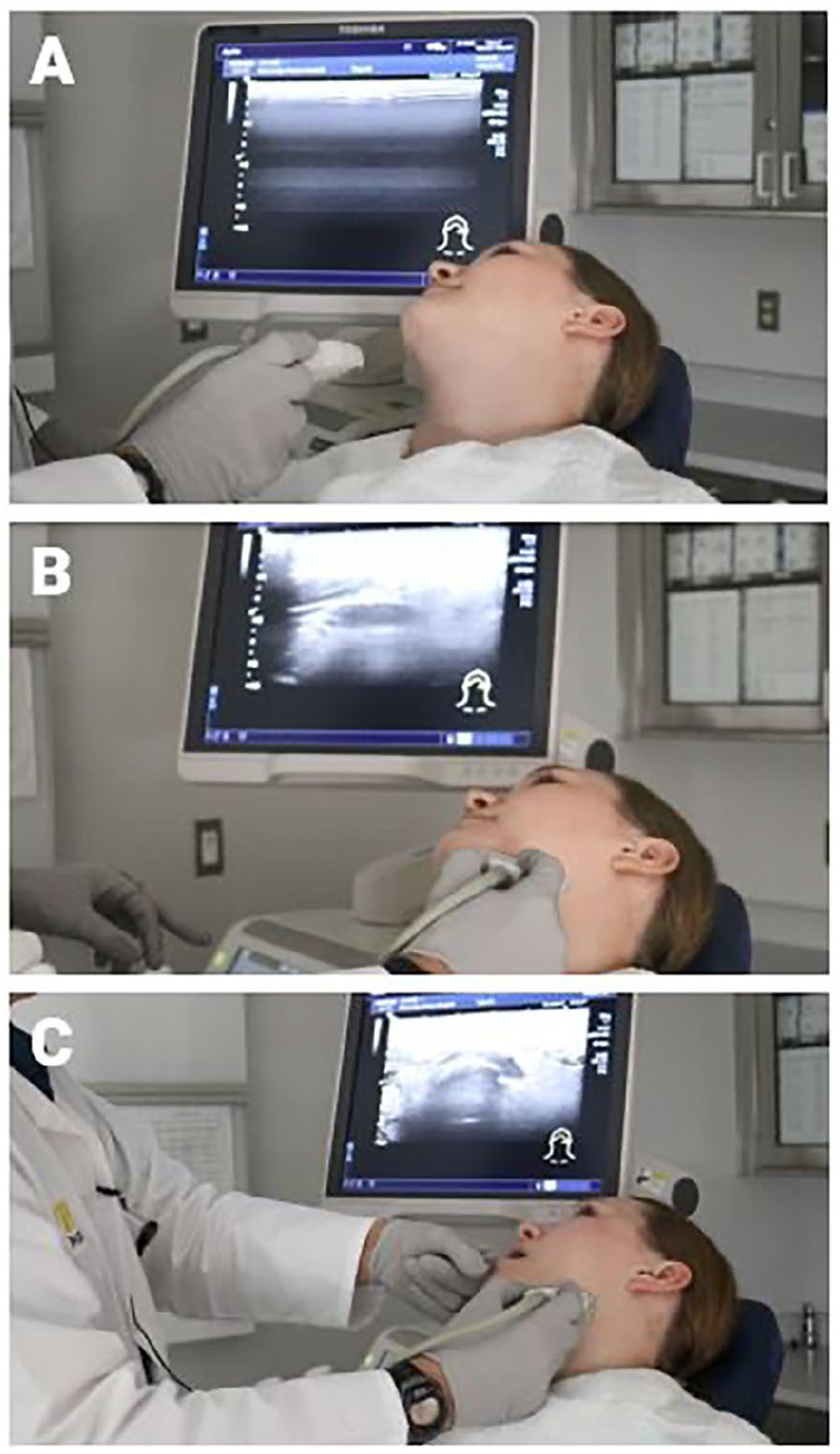
Patient and transducer positioning for sonopalpation. (A) The patient is seated in the exam chair with their head reclined slightly posterior and slightly toward the ultrasound operator. A towel is draped around the neck and chest to protect clothing from excess ultrasound gel. (B) To visualize the submandibular area, the transducer is placed parallel to the lower border of the mandible in a slightly-oblique transverse plane. (C) To perform sonopalpation, the ultrasound operator places their gloved finger into the patient’s mouth. The operator may move their finger along the submandibular space along with the transducer to allow for dynamic visualization of floor of mouth anatomy.
Results
Each patient’s presenting complaint was that of a painless upper neck mass, identified radiographically as cystic. US with sonopalpation correctly identified the relationship between the sublingual gland, extravasated fluid of the ranula, and mylohyoid dehiscence in all 3 cases (Figure 2). All plunging ranulas were surgically addressed with transoral sublingual gland resection, with the preservation of submandibular ductal drainage facilitated by sialendoscopy. The diagnosis of ranula was corroborated by intraoperative findings and/or pathology results in all 3 cases (Table 1).
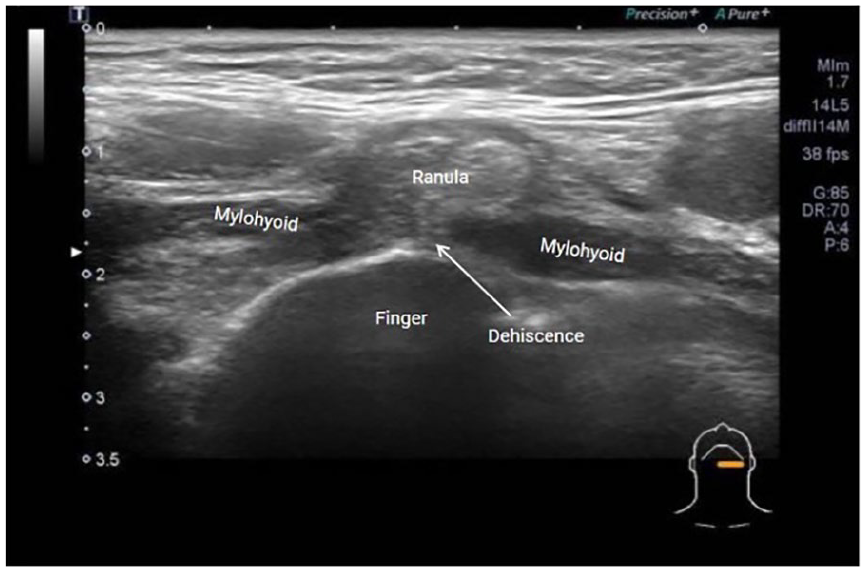
Sonopalpation identifying mylohyoid dehiscence and plunging ranula. With the US transducer placed in a transverse orientation (slightly oblique) addressing left level I, placement of the operator’s gloved finger inside of the patient’s mouth allows for manual application of pressure to bring floor of mouth tissues closer to the transducer. Sonopalpation allows for the visualization of a break in the hypoechoic mylohyoid muscle, with the more hyperechoic ranula protruding through the break. US, ultrasound.
Surgical and Pathological Correlation of Imaging Findings.
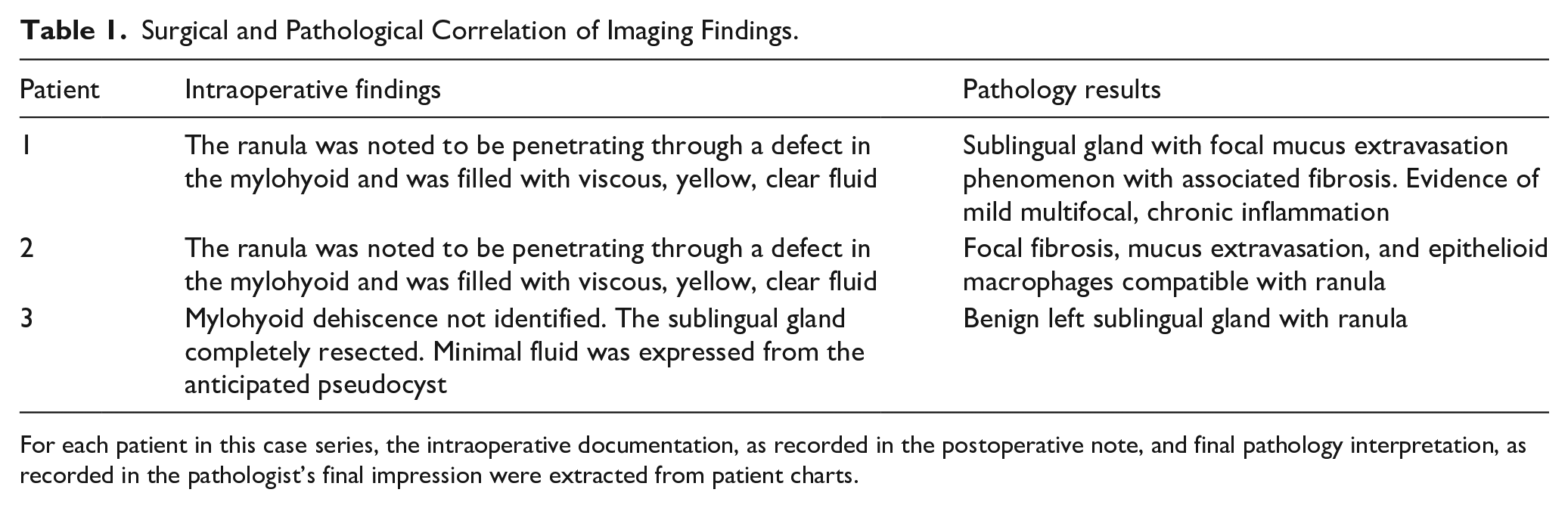
For each patient in this case series, the intraoperative documentation, as recorded in the postoperative note, and final pathology interpretation, as recorded in the pathologist’s final impression were extracted from patient charts.
Discussion
US with sonopalpation consistently identified anatomic abnormalities supporting the diagnosis of plunging ranula. The tail sign has been regarded as a pathognomonic finding for plunging ranula. However, it is not always present, and its absence does not reliably rule out a plunging ranula. Jain suggested that the tail sign is less common than previously reported and that reliance on an observed tail sign for the diagnosis of plunging ranula introduces potential for misdiagnosis and delay of appropriate treatment. 4 He reported a consecutive series of patients with surgically-treated plunging ranula with only 2 out of 126 patients demonstrating fluid within the posterior sublingual space. Of these 2 patients, only 1 displayed the classically-described tail sign on US.
In an earlier publication, Jain et al assessed a cohort of 33 patients with suspected plunging ranula with 100% of the US examinations identifying mylohyoid dehiscence. These US results were correlated with intraoperative findings of mylohyoid dehiscence in 30 (90.1%) of the cases. 5 Lee et al identified through CT study that plunging ranulas pass directly through a mylohyoid defect in 88% of cases with only 12% extended along via the posterior edge of an intact mylohyoid muscle. 2 These investigators identified that among those that passed through the mylohyoid dehiscence, only 38% exhibited the tail sign.
Sonopalpation has been used to evaluate for submandibular sialolithiasis. 6 Patel et al reported the sensitivity of detecting submandibular calculi was 96.6% using sonopalpation versus 91.5% for standard US and 83% for physical examination alone. We have applied a similar technique of sonopalpation as standard in our US evaluation for potential plunging ranula. This technique identifies the relationship between the sublingual gland, extravasated fluid of the ranula, and mylohyoid dehiscence.
Previous studies have assessed the interobserver reliability of salivary gland US specifically in patients with a diagnosis of Sjogren’s syndrome. Jousse-Joulin et al demonstrated that intra-observer reliability was substantial (kappa >0.60) when assessing salivary gland echogenicity and homogeneity. 7 US techniques are generally amenable to learning, with variable learning curves for different structures. 8 The learning curve for salivary gland US has not been fully characterized, and the technique of sonopalpation has not been robustly investigated for features such as intra-observer reliability, reproducibility, or assessment of a learning curve. In our study, a single, experienced US operator (H.H.) performed all US with sonopalpation, which does not offer an opportunity to discuss reliability, reproducibility, or learning curve.
Although we found sonopalpation to enhance our US assessment, this technique is limited by the same variables that limit imaging in general. Altered anatomy and with differing echogenicity of surrounding structures may prevent adequate visualization. Previous episodes of sialadenitis or a history of floor of mouth surgery may result in the formation of echogenic bands of scar tissue, which may make both head and neck US and therefore also sonopalpation difficult. Anecdotally, subjects in this study tolerated the sonopalpation procedure well. However, as has been reported, acute infection or inflammation may cause sonopalpation to be uncomfortable. 6
Conclusion
Plunging ranula is an uncommon condition that shares imaging characteristics with other abnormalities to elude definitive diagnosis employing standard US, CT, and MRI. Sonopalpation, as an adjunct to standard US, is an effective modality to better visualize floor of mouth anatomy to assess a plunging ranula. While the results of this proof-of-concept study are promising, they are limited by its small sample size and retrospective nature. Further research may better characterize interrater reliability, reproducibility, and learning curve, especially in assessing the feasibility of including this kind of US training in the residency process.
Footnotes
Ethical Considerations
This study was approved by the University of Iowa Institutional Review Board.
Consent to Participate
The requirement for informed consent to participate was waived. Patients included in this review have been de-identified and have given their written informed consent for the use of case history and images for publication and presentation purposes.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Henry Hoffman discloses his roles as an author for UpToDate, a research consultant for MeiraGTx and Everis, and a member of the advisory board for RiboX. Other authors have no financial conflicts of interest to declare.
Data Availability Statement
No new data were created as part of this research study.