
Abstract

Significance statement
Mucoceles originating in the submandibular gland, which are extravasation type, are extremely rare, and it is difficult to distinguish submandibular gland mucoceles from plunging ranulas without a tail sign through the defect of the mylohyoid muscle. Because submandibular gland mucoceles may masquerade as plunging ranula, submandibular gland mucocele should be considered preoperatively as one of differential diagnoses of submandibular cystic lesions.
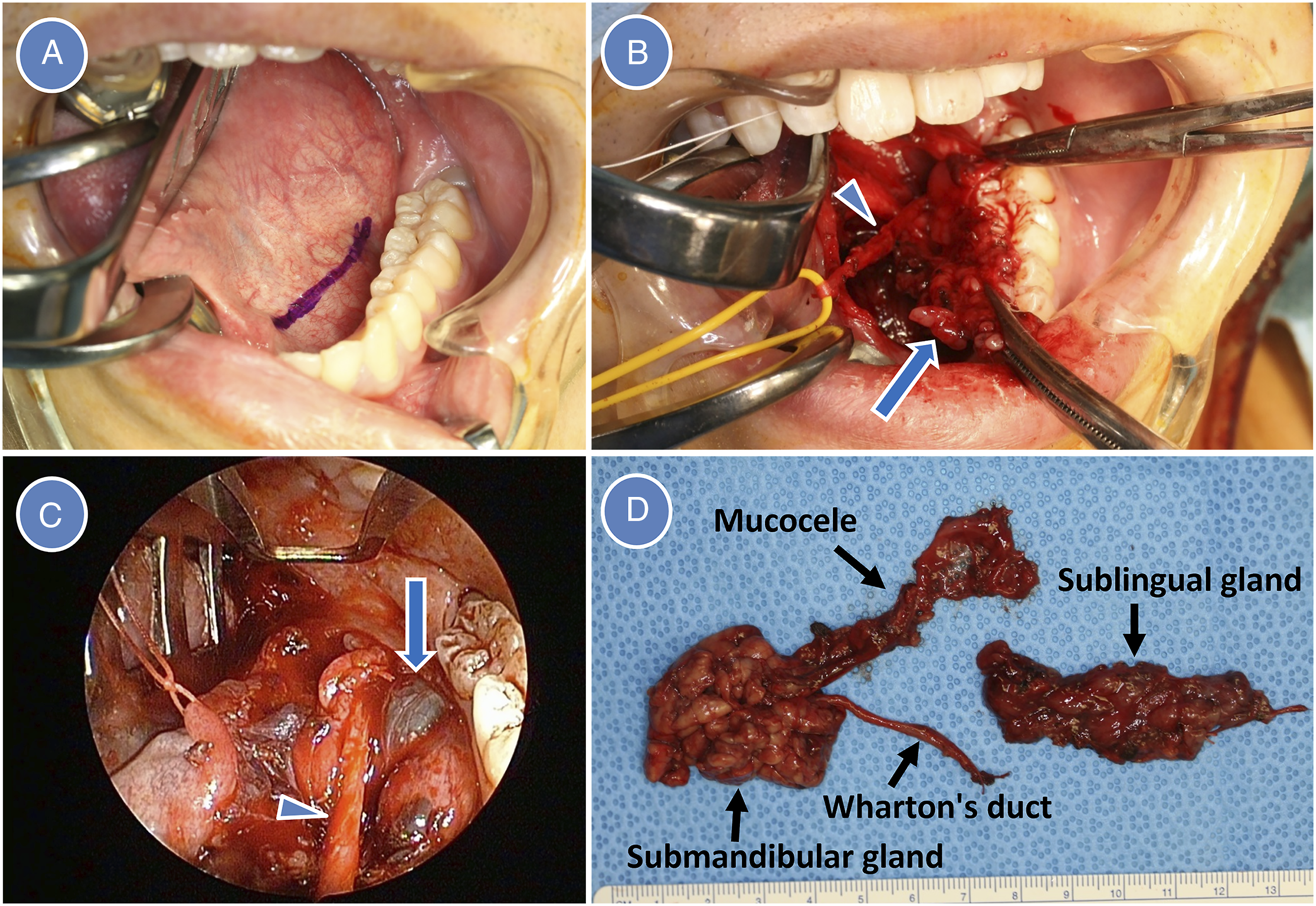
A 23-year-old male without previous history of submandibular trauma and surgery, infection, and viral illness was referred to our department with left submandibular painless swelling. The left oral floor was intact, and salivary flow from Wharton’s duct on digital submandibular pressure was normal. CT showed a well-circumscribed, homogeneous cystic lesion (44×34×22 mm) in the left submandibular region (Figure 1A and 1B). MRI showed a 36×33×22 mm well-circumscribed, cystic lesion had high signal intensity on T2-weighted and short TI inversion recovery images (Figure 1C and 1D). Although both imaging did not show the tail sign, the lesion was diagnosed as a plunging ranula through the defect of the mylohyoid muscle (MM), and the patient underwent surgery under general anesthesia. After mucosal incision of the left oral floor and identification of Wharton’s duct and lingual nerve, sublingual gland (SLG) removal was performed (Figure 2A and 2B). However, there were no MM defects and definitive continuity between the SLG and the cystic lesion. Therefore, the cystic lesion was intraoperatively considered a submandibular gland (SMG) mucocele. Following the SLG removal, endoscopically assisted intraoral removal of the SMG with mucocele was performed. After soft tissues surrounding the SMG were dissected bluntly, the mucocele and SMG were exposed more prominently by digital pressure applied beneath the lower border of the mandible by an assistant (Figure 2C). The submandibular ganglion and Wharton’s duct were ligated and cut, and the lingual nerve was preserved. The SMG was gripped with forceps after aspiration of mucocele and pulled up through the incision by gland dissection. Because the facial artery did not penetrate the SMG, an only the glandular branch of the facial artery was ligated and cut, and the SMG with mucocele was removed completely in intraoral approach (Figure 2D). A 30°, 4-mm diameter, endoscope with tissue retractor (Karl Storz, Tuttlingen, Germany) was used for detecting residual gland and hemostasis in the submandibular space after both glands’ removal. After a suction drain was inserted through the incision site, the wound was closed. The drain was removed on the first postoperative day, and the patient was discharged on the second postoperative day. The pathological diagnosis was SMG mucocele. Although lingual nerve paresthesia occurred postoperatively, the paresthesia was resolved completely 1 week after surgery, and there was no recurrence 8.5 years after surgery. CT and MRI. (A) CT (axial image), (B) CT (coronal image), (C) MRI (axial image), and (D) MRI (coronal image). Arrow indicates a submandibular cystic lesion. Surgical view and removed specimen. (A) Intraoral view before mucosal incision of the oral floor without swelling. (B) Removal of the sublingual gland (arrow). Arrowhead indicates Wharton’s duct. (C) Mucocele (arrow) was exposed during dissection of deep soft tissues after sublingual gland removal. Arrowhead indicates Wharton’s duct. (D) Removed specimen.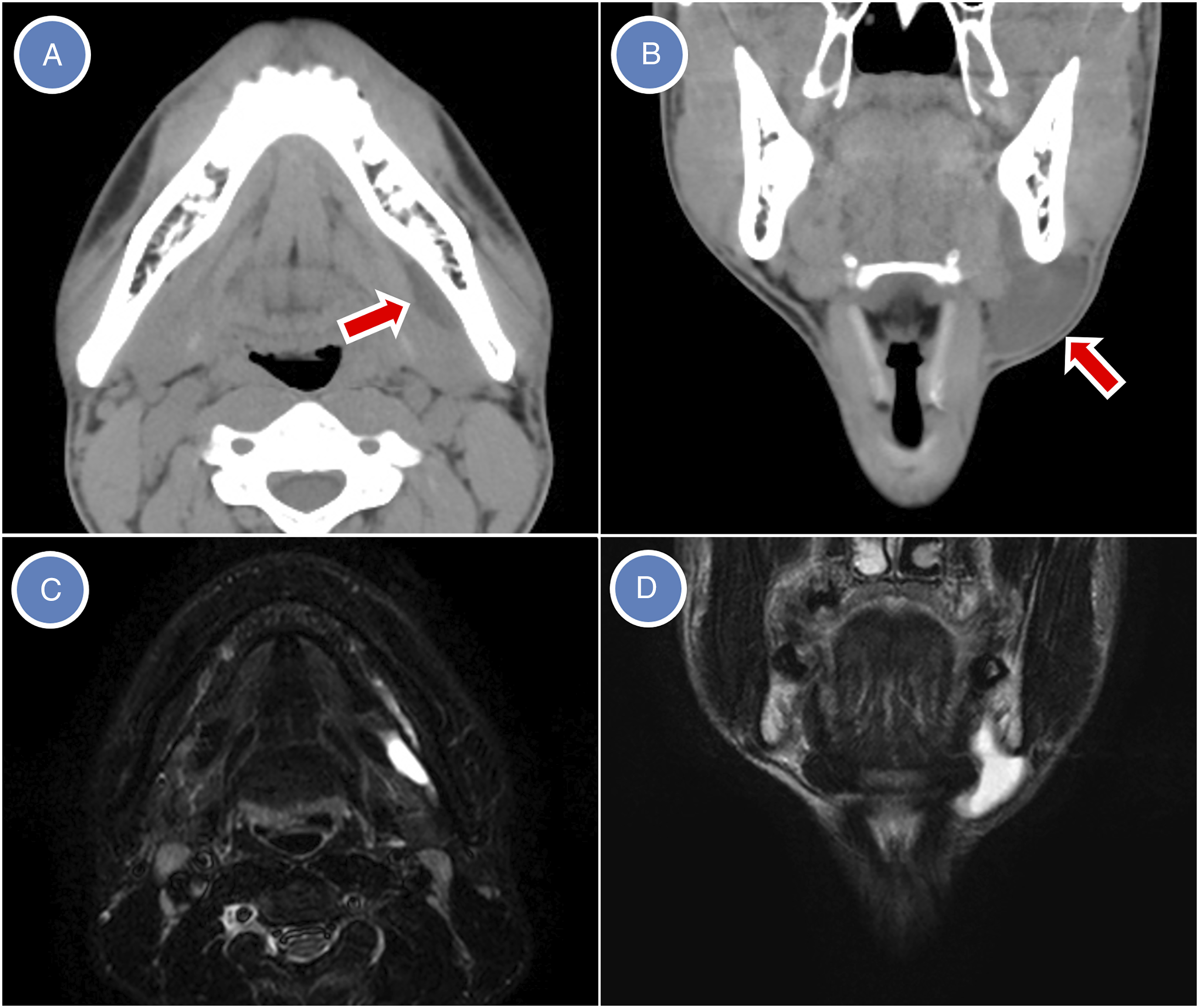
Plunging ranulas arise from the SLGs and extend below the mylohyoid muscle, beyond the sublingual space, and involve the submandibular space and adjacent structures. 1 Tail sign, which indicates the communication between the sublingual and submandibular space over the posterior edge of the mylohyoid muscle, is the characteristic feature of the plunging ranula. However, plunging ranulas do not always show tail sign. The MM defect was the more common route for extravasation. Therefore, absence of the tail sign does not exclude the diagnosis of a plunging ranula.
Mucoceles arising in the SMG, which are extravasation type, are extremely infrequent,1 -9 and the incidence is 0.6% of all SMG tumors and cysts. 2 Generally, SMG mucoceles are unilateral, and there is only one bilateral case. 3 It is difficult to distinguish SMG mucocele from plunging ranula without a tail sign through the MM defect. When the tail sign is absent and the mucocele is close to or within the parenchyma of the SMG, it should be assumed that the origin of the lesion is the SMG. 1
The treatments of SMG mucocele are carried out conservatively or surgically. Conservative treatments include aspiration, sclerotherapy, irradiation, marsupialization, and incision and drainage.1,9 Although surgical treatments are performed by simple cystectomy, removal of SMG with mucocele, removal of SLG and SMG with mucocele, 3 or removal of both glands with mucocele provides a good prognosis. 1 In the present case, both glands’ removal was performed in only intraoral approach without cervical scar and facial nerve injury. When plunging ranula without tail sign or SMG mucocele is considered preoperatively as the differential diagnosis of submandibular cystic lesions, surgeons should explain to the patient possibility of SMG removal as well as intraoral SLG removal.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.