
Abstract
We report a rare case of objective tinnitus induced by nasopharyngeal muscle constriction. A 49-year-old female patient presented at the clinic with unintentional sounds coming from the nasal cavity while talking or swallowing, which were similar to the lip-smacking sound. Physical examination revealed a hypertrophic posterior nasopharyngeal wall and torus tubarius at rest. With voluntary effort, the posterior pharyngeal wall protruded prominently and collided with the torus tubarius on either side, generating a sound when they were separated. Botox injection was recommended but the patient refused. The diagnosis and treatment of objective tinnitus are well established, but in some cases, it may occur under unexpected conditions. We report a novel type of objective tinnitus. A thorough physical examination for tinnitus could reveal the cause.
Introduction
Tinnitus is the perception of a sound in the absence of a corresponding acoustic source. It can be classified into sensorineural tinnitus and somatosound. Although sensorineural tinnitus is presumed to originate from the cochlea and auditory nerve, somatosound can be caused by blood vessels, muscles, the eustachian tubes, and the temporomandibular joints. Somatosound is also known as objective tinnitus since it can be perceived by both patients and examiners. Various conditions can cause objective tinnitus, and the most representative forms are vascular tinnitus, myoclonic tinnitus, temporomandibular joint clicks, and tinnitus caused by a patulous eustachian tube.1 -3 Objective tinnitus is much less common compared to sensorineural tinnitus; nevertheless, its diagnoses and treatments are well established, probably due to its high curability rate. Numerous studies have been conducted on the classification, causes, diagnostic approaches, and treatments of objective tinnitus. Thus, in the case of vascular tinnitus, which is the most common form of objective tinnitus, 92% to 100% of etiologies can be found using correct imaging modalities if the symptoms are objectively demonstrated. 4 However, some cases of objective tinnitus occur under unexpected conditions. This report describes a novel type of objective tinnitus caused by collision of nasopharyngeal structures which, to our knowledge, has not been reported previously.
Case Report
A 49-year-old woman visited the clinic with a 1-year history of hearing unintentional sounds coming from the nasal cavity while talking or swallowing. She could also produce the sounds voluntarily. She described the sounds as like the sound of lip smacking (Supplemental Material 1). She had no underlying diseases other than seasonal allergic rhinitis, which was asymptomatic at the time of the visit. She had no surgical history or trauma that could have caused changes to the nasopharynx or method of vocalization. She had not experienced a weight change and had not yet undergone menopause.
No abnormal findings were observed in the oral cavity or oropharynx on external examination. Examination of the nasopharynx using a flexible fiberscope revealed a hypertrophic posterior wall and torus tubarius in the resting state (Figure 1A). With voluntary effort, the patient could make the posterior wall of the nasopharynx protrude prominently and collide with the torus tubarius on both sides, generating a smacking/popping sound when they separated (Figure 1B). A neck computed tomography (CT) scan was performed and the patient was instructed to make the sound during the scan. The CT images were compared with paranal sinus CT images taken in the resting state prior to the visit (Figure 2A). CT scan revealed increased protrusion of the posterior wall and medialization of torus tubarius on effort, resulting widening of the contact area (Figure 2B). There were no other findings of note, such as signs of infection or masses.
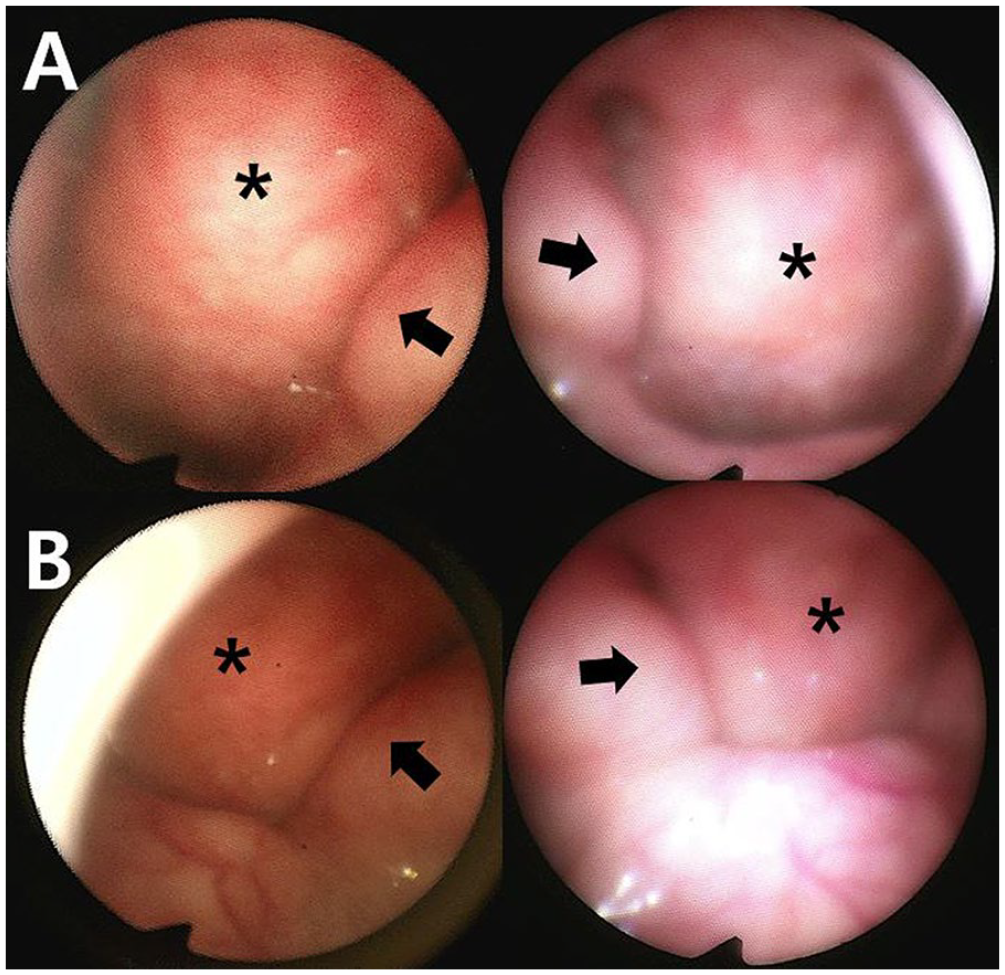
Views of the nasopharynx using a flexible fiberscope. (A) In the resting state, the posterior pharyngeal wall (asterisk) and torus tubarius (arrow) are hypertrophic. (B) Medialization of the torus tubarius and collision of the torus tubarius with the protruding posterior pharyngeal wall, obtained with voluntary effort. The panels on the left are the views of the left nasal cavity, and the panels on the right are views of the right nasal cavity.
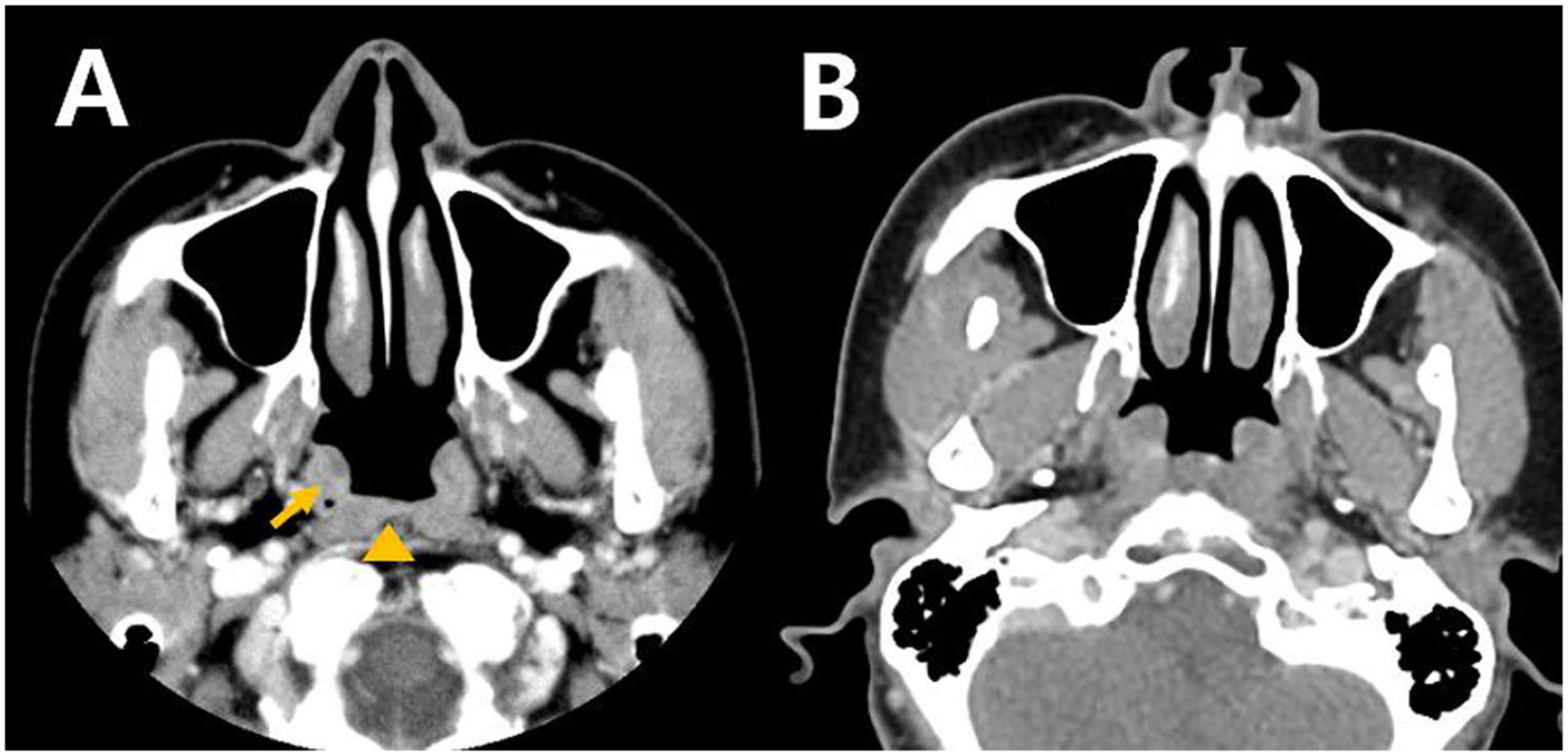
Comparison of computed tomography images of the nasopharynx in the resting state and with voluntary effort. (A) The torus tubarius (arrow) and posterior pharyngeal wall (arrowhead) are hypertrophic in the resting state. (B) Anterior protrusion of the posterior pharyngeal wall and medialization of the torus tubarius achieved with voluntary effort, causing them to collide.
Botox injection to reduce the posterior wall muscle volume was recommended; however, the patient refused. Currently, she has been undergoing periodic follow-up for 1 year with no change in the symptoms.
Discussion
This case of objective tinnitus originated from the nasopharyngeal structures. Tinnitus was generated as the nasopharyngeal posterior wall and torus tubarius made contact and were separated. The causative lesions could be detected with the help of a flexible fiberscope, which could observe the dynamic changes of the structures in real time. Imaging examinations, while the symptoms were elicited, were also useful diagnostically. To our knowledge, this is a new clinical type of objective tinnitus that has not been reported previously.
It is natural that sound can be generated by the collision and separation of structures, but it is unusual for this phenomenon to suddenly occur without any obvious cause. We hypothesize 3 possible pathogenic mechanisms: First, decreased secretion of sex hormones with age may have resulted in pharyngeal muscle hypertrophy. Estrogen and progesterone play an important role in the regulation of body fluids and sodium levels. 5 A previous study revealed that the secretion of sex hormones decreases during the perimenopausal period, which can cause changes in the osmotic arginine vasopressin (AVP) threshold and AVP synthesis. A change in AVP homeostasis results in water and sodium retention and decreased urine output, leading to systemic edema 5 . Decreased secretion of hormones in the perimenopausal period can cause water retention, resulting in muscle hypertrophy. Although the patient had not yet undergone menopause, considering that the average age at menopause in Korea is 49.2 years, 6 it is highly likely that menopausal transition is in progress. The onset of the symptoms 1 year previously may have been related to hormonal changes during perimenopause. Additional studies, including blood sampling, could provide more clues. Second, the possibility of diseases that cause muscle hypertrophy, such as myositis, should be considered.7,8 Although the patient had no symptoms of myositis such as muscle weakness or dysphagia and no history of autoimmune disease, biopsy could reveal myositis. Third, the patient’s method of vocalization may have changed the nasopharyngeal structures. Changes in the method of vocalization can result in hypertrophy of the laryngeal muscle, 9 and use of the laryngeal muscle can affect the pharyngeal structures. 10
In this case, posterior wall muscle hypertrophy was suspected to be the main cause of the unintentional sound. Botox injection was recommended as the first-line treatment to reduce the muscle volume. Botox binds to the presynaptic cholinergic nerve terminals and inhibits the release of acetylcholine, causing paralysis and subsequent functional denervated muscle atrophy. Although the degree of muscle atrophy varies from study to study, Botox generally brings about a 30% to 40% reduction in the muscle volume. 11 Botox has the advantage of being noninvasive as it can be applied via the nasal cavity or oral cavity without additional incisions, and even if an unintended effect occurs, it can be applied relatively safely because it washes out after several months. Although the patient refused further treatment, using Botox is still a safe option that can be tried if the symptoms persist.
Physicians should be aware that objective tinnitus has various causes. A thorough physical examination for tinnitus could reveal the cause.
Footnotes
Data Availability Statement
The data used to support the findings of the study are included whtinin the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Research Foundation of Korea funded by the Korean Government (MSIT) (No. 2022R1F1A1071824) to J.M.L.
Ethical Statement
This study was approved by the Institutional Review Board of the authors’ institute (IRB number: ISPAIK 2023-04-021), and the requirement for informed consent from the patient was waived. The patient’s anonymity is preserved in the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.