
Abstract
Tinnitus is a common complaint in the clinical setting and can be classified into sensorineural and objective tinnitus. The sources of objective tinnitus may either come from para-auditory structures, such as myogenic or vascular structures, or the middle ear muscles. One type of objective tinnitus of muscular origin is known as forceful eyelid closure syndrome (FECS). We present an additional case of a 22-year-old woman with unilateral FECS. The auricles and external auditory canals were normal bilaterally; we examined her tympanic membrane under an endoscope, the left tympanic membrane was retracted simultaneously with the closure of her eyelids. Both tympanograms were of type A. However, small cut trace associated with tympanic membrane movement were obtained during blinking. The patient was managed by behavioral therapy and medication treatment conservatively, and the condition became well-controlled. Here, we present this rare case and review the literature.
Introduction
Tinnitus is a common complaint in the clinical setting and can be classified into sensorineural and objective tinnitus, while the latter is rare. The sources of objective tinnitus may either come from para-auditory structures, such as myogenic or vascular structures, or the middle ear muscles. 1 As a result, objective tinnitus is not just audible to the patient but also can be heard and/or recorded by an observer.
One type of objective tinnitus of muscular origin is known as forceful eyelid closure syndrome (FECS), which was reported in the Proceedings of the Second International Tinnitus Seminar in 1983,1 -9 and it has also been found to be associated with myoclonus in the middle ear (MEM). 4 The symptoms of FECS include muscular tinnitus related to forced eyelid closure. 4 There are currently less than 20 cases reported of FECS,1 -4,6 -8 and here we present an additional case of a 22-year-old woman with unilateral FECS.
Case presentation
In this case, a 22-year-old female complained of noise in her left ear for the past three months, which was only heard when she blinked forcefully. Three months ago, after working long hours on the computer, she noticed that her eyes were dry, and she blinked several times hard and heard a noise in her left ear simultaneously. The symptom was successfully replicated when she was at the clinics, but no abnormal noise with gentle eye closure. The patient described the sound as a creak of walking in the snow. Sleep and work were not affected by the symptom. The patient admitted, however, that she often repeated the same motion of eye blinking when she noticed the tinnitus and forced eye closure became a habitual behavior. Her symptoms did not include hearing loss, otalgia, otorrhea, or vertigo, nor did she experience any facial pain (trigeminal neuralgia) or headache.
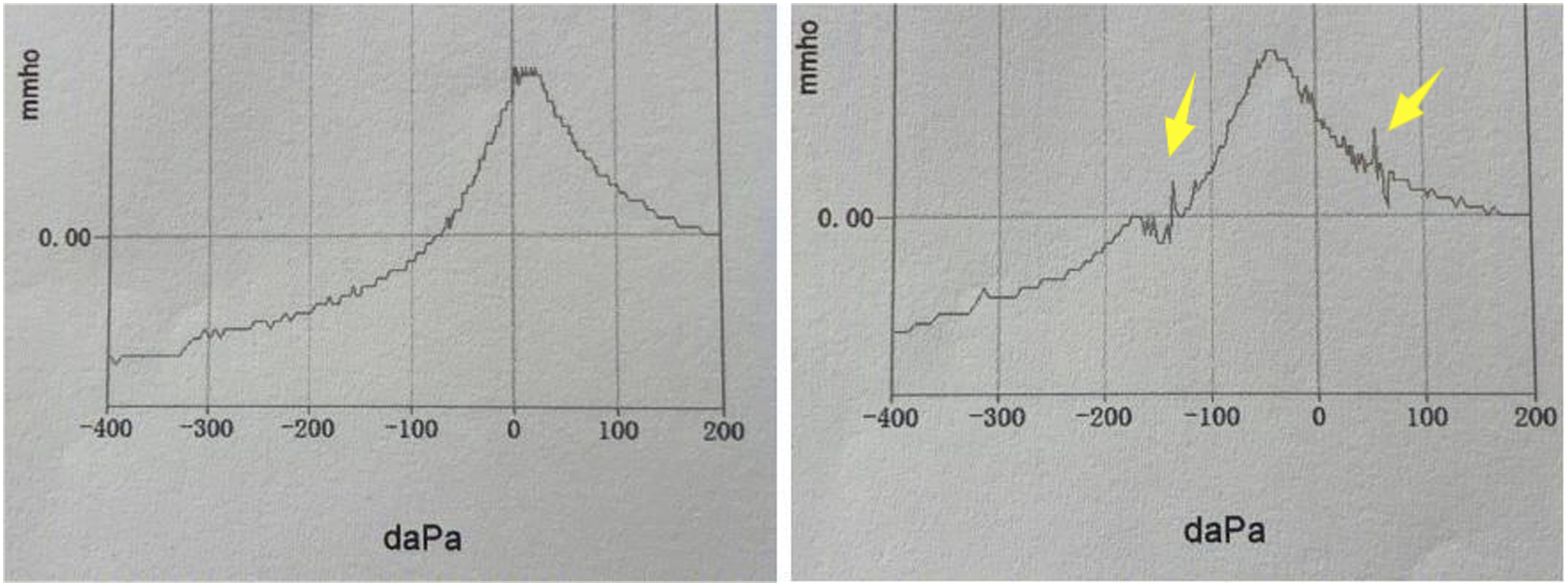
The auricles and external auditory canals were found to be normal bilaterally on examination, and the movement of the palate and pharynx was found normal. As we examined her tympanic membrane under an endoscope, the left tympanic membrane was retracted simultaneously with the closure of her eyelids (Supplement Video 1), although both tympanic membranes were normal. Computed tomography (CT) and magnetic resonance imaging (MRI) of the middle and inner ear were unremarkable (Figure 1), and pure tone audiometry showed that the hearing threshold was normal. Both tympanograms were of type A. However, small cut trace associated with tympanic membrane movement were obtained during blinking (Figure 2), but the auditory brainstem response was normal. Impedance audiometry of the left ear showed a slight change in compliance, simultaneously with eye blinking. Her previous otologic history was unremarkable and did not include facial paresis. In addition, she was stressed from her work. As a result of the fact above, she was diagnosed with objective tinnitus due to FECS, with the muscles of the middle ear as a plausible cause. Computed tomography (CT) and magnetic resonance imaging (MRI) of the middle and inner ear were unremarkable. Small cut trace associated with tympanic membrane movement were obtained during blinking.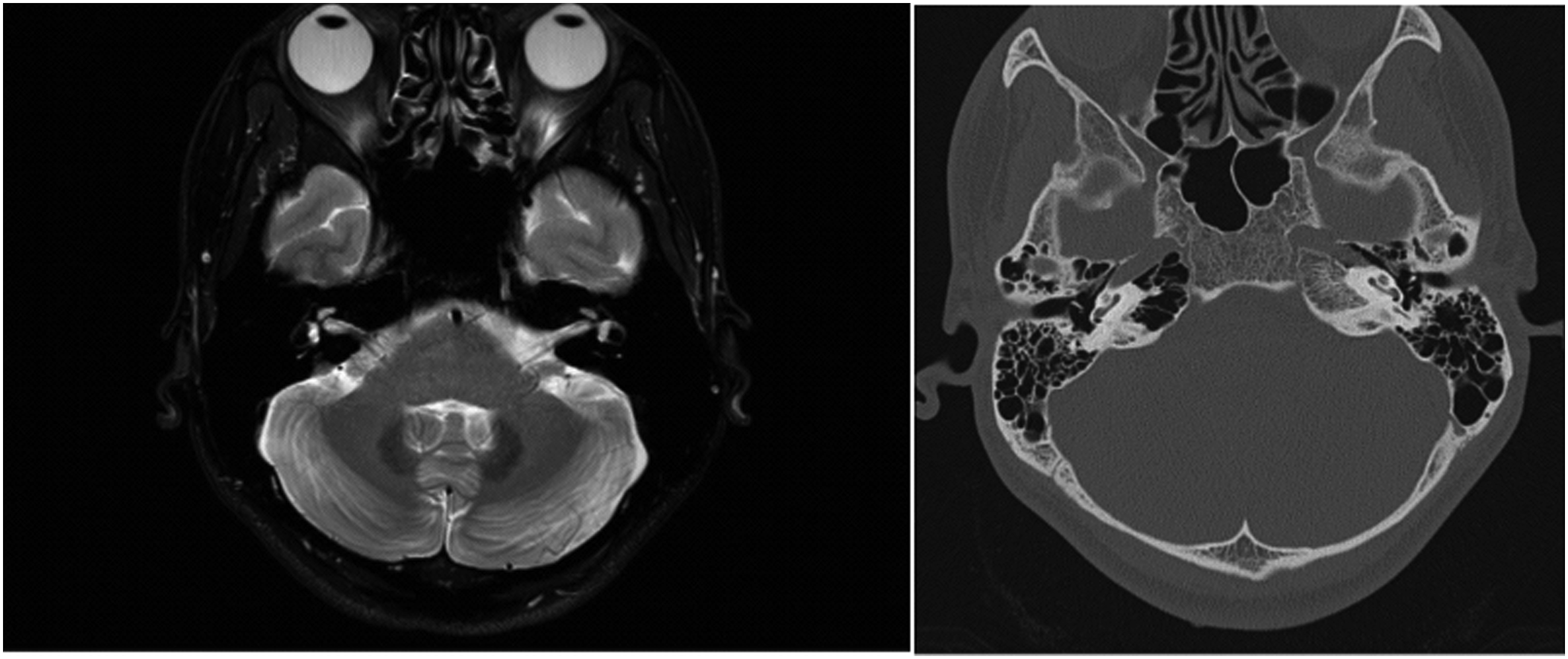
After explaining the disease to her, two treatment plans were given. The patient can take carbamazepine 100mg BID orally if the tinnitus bothers her. Otherwise, she could relax and reduce focus on tinnitus. She chose the medication plan, and she would attempt to avoid habitual blinking. After four weeks, the patient revisited and reported that carbamazepine helped reduce her tinnitus, but she quit taking it after two weeks as the medication induced drowsiness. She stayed home for the next two weeks, did things such as yoga and reading, and reminded herself not to blink forcefully. As a result, her tinnitus was relieved, although it was still present.
Discussion
FECS is one type of muscular-origin objective tinnitus and mainly affects patients under 20 years,4,9 with more than 60% being female. 9 It is often observed as one of the sequelae of facial nerve palsy. 10 It should be noted that several cases have been reported without any history of facial paralysis, such as this case. The precise mechanism of FECS is poorly understood. Occasionally, a causative lesion can be identified in the brainstem or cerebellum via magnetic resonance imaging. However, most cases are idiopathic. 7
FECS is a rare disorder assumed to be caused by the contraction of muscles in the middle ear, that is, the stapedial muscle and the tensor tympani muscle. 5 The tensor tympani muscle is innervated by the mandibular branch of the trigeminal nerve—CN V, and the orbicularis oculi and stapedius muscle by the facial nerve—CN Ⅶ. Most people speculated that abnormal communication occurred between the fifth and the seventh pairs of brain nerves. FECS has been hypothesized to be due to abnormal communication between the facial nerve and trigeminal nerve.2,4,9
A buzzing sound is considered to be associated with the Stapedius muscle contraction,11,12 and a clicking sensation is related to the Tensor Tympani muscle contraction. 13 Previously, Masafumi Ohki 1 and Keishi Fujiwara 14 reported cases of objective tinnitus concomitant with eye closure, and they believed that the tinnitus was attributed to stapedial muscle contraction. However, Seokhwan Lee presented the first report of an MEM concomitant with eye blinking treated by resection of the tensor tympani tendon. Lee et al. identified the retraction of the only tensor tympani tendon with eye blinking, and the tensor tympani tendon was resected and the tinnitus was completely resolved immediately. 15 Currently, the tympanic tension muscle contraction is not objectively distinguishable from the stapes muscle contraction, which must be explored directly with the microscope or endoscope after tympanotomy. 16
Most of the patients had triggering factors for FECS, 4 such as stress events, nervousness, and anxiety. Similarly, work-related stressors were also presented. These factors may affect neurological function, and forceful eyelid closure was suggested to induce abnormal crosstalk between the facial and trigeminal nerves. 4 In a study by Rock et al. that examined a total of 432 ears, the patients were asked to close both eyelids forcefully, and 25% (108 ears) were found to be positive on retraction of the TM after otomicroscopy. However, FECS are rarely reported in the literature. One hypothesis made by Rock was that the sound could be subtle and ignored by most people, so the awareness of the sound could largely depend on one’s own sensitivities. 2 In one case, a patient was found that both of her tympanic membranes moved upon blinking, but she just complained of one side tinnitus. 7 This type of tinnitus is fatigable, 2 and the tinnitus would be gradually weakened if she closed her eyes forcefully for several successive times. Smith, Rock, and Ohki M found that the patients may suffer hearing loss during forced eye closure, but no hearing loss during a resting period.1,2,17
In all the cases reported, scholars found there was significant perturbation synchronous with eye closure in the impedance audiogram. 4 Therefore, acoustic reflex decay with or without static compliance during eye closure might be a promising audiologic test tool for the diagnosis of FECS. However, with the development of otoendoscope, observation and recording of movement in the TM might be more practically useful as it provides more direct and straightforward diagnosis. Thus, the movement of the TM synchronous with forced eye closure on endoscopic examination is the current most reliable diagnosis of FECS.
Several options exist for the management of FECS in the previous literature. Considering patients with FECS generally involve triggering factors, and the level of distress is often related to the patient's own sensitivity, the initial treatment should include feature reassurance, conservative therapy, and behavioral therapy. Tinnitus masking devices described by East and Hazell 18 and zygomatic pressure maneuvers developed by Chan and Palaniappan 19 may also be practiced. Medical management with anticonvulsants 3 or sedatives is ineffective for tinnitus associated with FECS, such as carbamazepine. 20 Doctors should pay attention to its potential side effects, such as bone marrow suppression, and development of liver and/or kidney abnormalities. When conservative management is ineffective, botulinum toxin injections may be practiced.21,22 Thomas M reported a 52-year-old woman with bilateral FECS, exhibiting features of cranial nerve (CN) V3, CN VII, and possibly CN X involvement. The patient was successfully treated with a trial injection of botulinum toxin to the soft palate. 9 In 2018, Jennifer Dang presented a unique pediatric case of FECS that was successfully managed by trans-palatal injection to the aponeurosis of the tensor veli palatini. 23 Middle ear tendon resection is preferable as the ultimate treatment option for patients who do not respond to conservative treatments as described above.1,4 Considering various treatment options for FECS, we chose behavioral therapy and medication treatment for this case. However, due to the side effects of carbamazepine, the patient only adhered to behavioral therapy, but the treatment plan was effective in mitigating the tinnitus.
In this reported case, it is important to follow the patient for a longer period of time to observe how the tinnitus progresses, monitor whether there are other related symptoms, and perform regular head imaging examinations for early detection of any potential system lesions. In the future, we aim to collect more similar cases, analyze them comprehensively, and determine more accurate and reasonable pathogenesis.
Conclusion
FECS is a very rare disease with only a few reported cases, which makes it unknown to many otolaryngologists. 8 It is also possible that some patients are missed for diagnosis. Thus, diagnosis and treatment of this disease have been challenging until now. Otologists should be aware of this rare but treatable entity of muscle-origin tinnitus and select appropriate treatment individually.
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Shenzhen Second People’s Hospital Clinical Research Fund of Guangdong Province High-level Hospital Construction Project (Grant No.20203357009).
Informed consent
Informed consent has been obtained from the patient and her family.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.