
Abstract
Introduction
In the otology clinic, most adult cholesteatomas are usually associated with a retraction pocket or a tympanic membrane (TM) perforation, often with otorrhea. Cholesteatomas behind intact tympanic membrane (ITMC) are rarely encountered in adults. 1 Di Lella et al. 1 reported ITMC without retraction pockets in 16 adults. Mills et al. 2 reported 17 adult patients with ITMC without any evidence of a retraction pocket in the attic or pars tensa. Lee et al. 3 found ITMC with tiny pars flaccida retractions in 11 adult patients. Kim et al. 4 reported that, of 1320 adult patients studied, 146 (168 ears) with unilateral or bilateral cholesteatomas exhibited tiny attic retractions but normal partes tensae.
The mechanism by which ITMC develops is not understood. Earlier studies suggested that most adult ITMC were acquired but TM perforations and retraction pockets were lacking.1–4 In patients with chronic otitis media (COM), ITMC may be associated with pars flaccida retraction caused by Eustachian tube (ET) dysfunction or squamous epithelium ingrowth from the edge of a perforation.1–4 Although sporadic cases of ITMC have been reported by a few authors,1–4 the clinical and imaging features of acquired ITMC in adults remain unclear. Acquired ITMC patients are commonly overlooked because of the absence of both a typical retraction pocket and a TM perforation. In this study, we retrospectively reviewed our experience with acquired ITMC in adults focusing on the clinical features of and the surgical outcomes.
Materials and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethics Review Board of our hospital, which is affiliated with Yiwu Central Hospital. Informed consent was obtained from all participants.
Methods
The clinical records of patients who underwent tympanomastoidectomy to treat acquired ITMC at our tertiary care referral center between January 2009 and June 2022 were retrospectively reviewed. ITMC were diagnosed via endoscopy, high resolution computed tomography (HRCT) of the temporal bone, and magnetic resonance imaging (MRI), and confirmed histopathologically. All patients had intact TM partes tensae with or without otitis media with effusion (OME), with or without tiny pars flaccida retractions, and with or without previous TM perforation and otorrhea. Patients with a history of trauma or middle-ear surgery (cholesteatoma surgery, myringoplasty, or tympanoplasty) were excluded.
To be classified as congenital, cholesteatoma must respect the criteria proposed by Derlacki and Clemis 5 and successively modified by Levenson et al 6 : an intact eardrum; no history of TM perforation, otorrhea, or previous ear surgery. Thus, ITMC was considered congenital in presence of a whitish mass behind an intact TM in a patient with no history of TM perforation, otorrhea, trauma or previous ear surgery. Otherwise, it was considered acquired.
The study population was divided into an OME group (Group A) and a previous perforation group (Group B). We analyzed clinical and operative findings and postoperative complications (recurrent or residual cholesteatoma and TM status). Postoperative evaluation employed endoscopy and HRCT was performed 24 months after operation. We gathered audiometric data, and averaged the hearing thresholds at 0.5, 1, 2, and 3 kHz preoperatively and 24 months postoperatively. The clinical features, surgical methods, audiometric data, and HRCT findings were compared between the 2 groups.
Results
A total of 13 patients (8 male and 5 female, average age of 31.6 ± 4.8 years, range 21-54 years, and 9 right ears and 4 left ears) with ITMC were included. All 13 patients were considered to have acquired cholesteatomas based on the criteria of Derlacki and Clemis.
All had been misdiagnosed at least 3 times. ITMC were diagnosed based on the HRCT findings, and endoscopic and histopathologic examinations. Of the 13 patients, OME was evident in 10 (Group A) but there were coexisting atrophic TMs in 3 (Group B) (Figure 1).
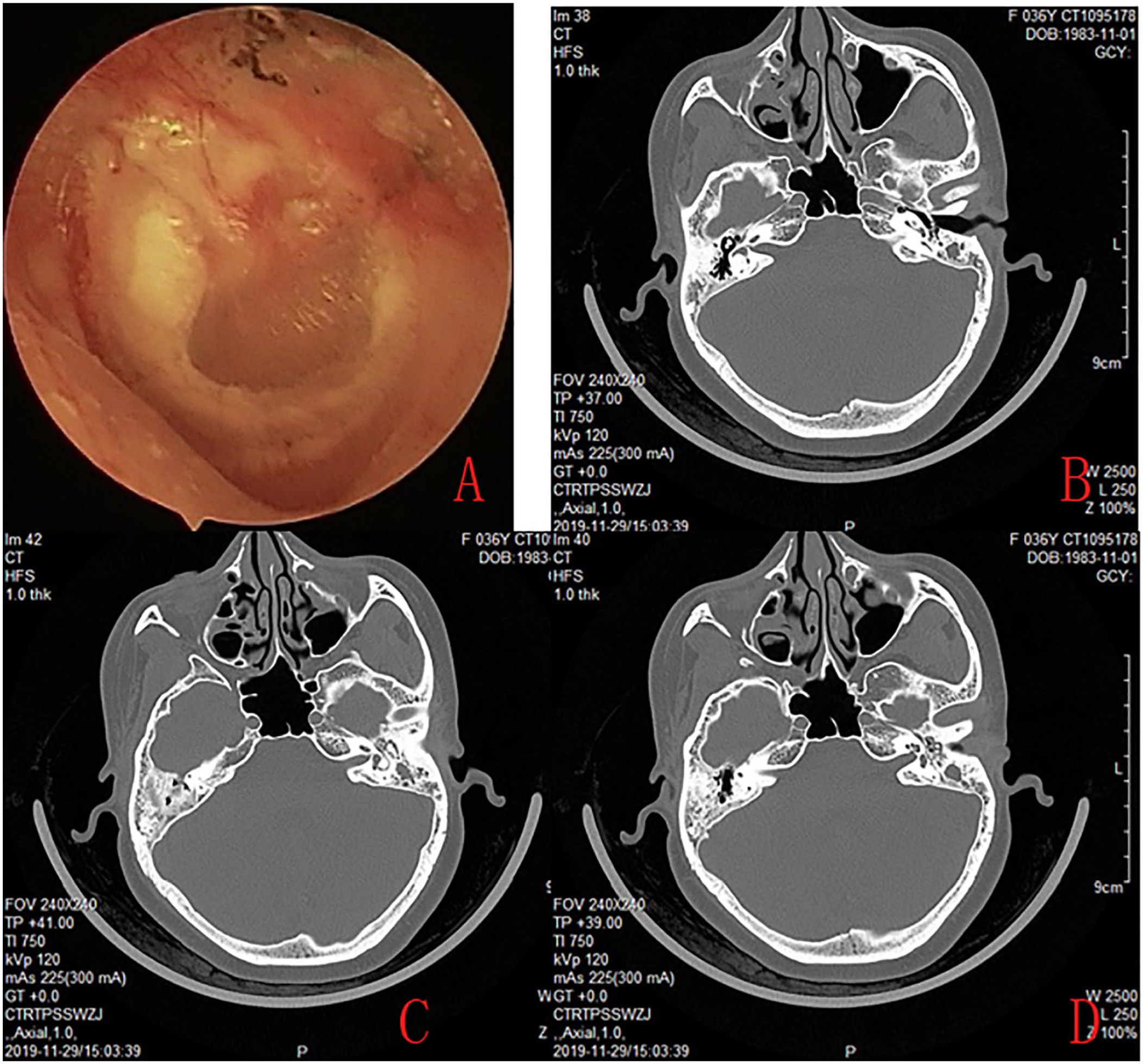
A 32-year-old female’s endoscopy revealed an intact atrophic TM with myringosclerotic plaques (A). CT revealed cystic soft tissue in the antrum and aditus ad antrum (B, C, and D).
All 10 Group A patients had histories of OME, no patient had undergone tympanostomy tube insertion but all reported histories of paracentesis. Endoscopic examinations revealed white masses behind intact TMs in the anterosuperior quadrants of 6 patients (Figure 2) and the posterior upper quadrants of 4 (Figure 3). In addition, tiny pars flaccida retractions with crusting were found in 7 (70%) patients whereas pars tensa retractions were found in 3 (30%). Of the former 7 patients, 2 exhibited type I attic retractions and 5 type II attic retractions as defined by Tos and Poulsen. 7
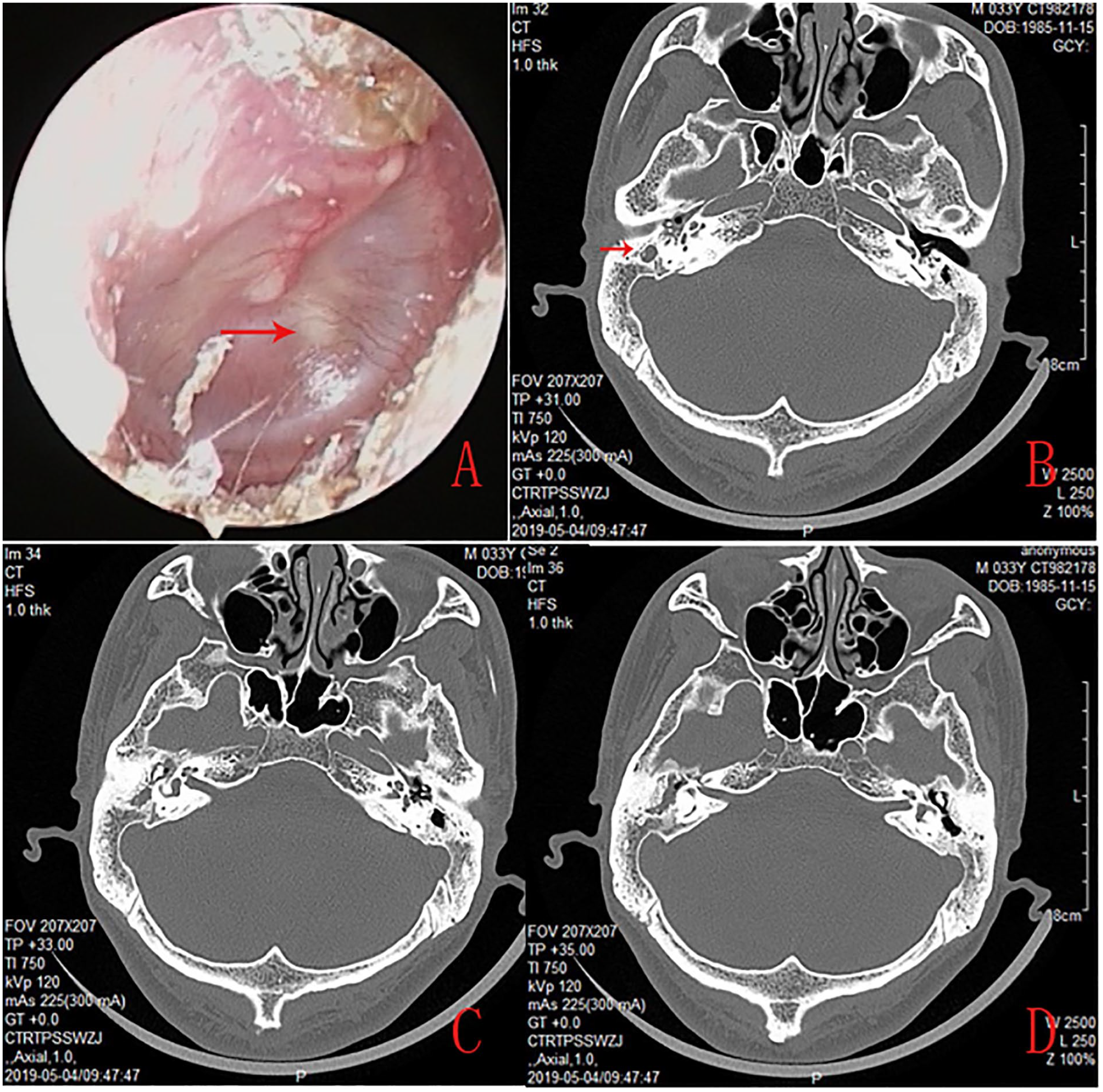
A 29-year-old male’s endoscopy revealed a white mass behind the anterosuperior quadrant of an intact TM, and effusion and crusting of the pars flaccida (A). CT revealed soft tissue in the antrum, aditus ad antrum, and tympanic cavity (B, C, and D).
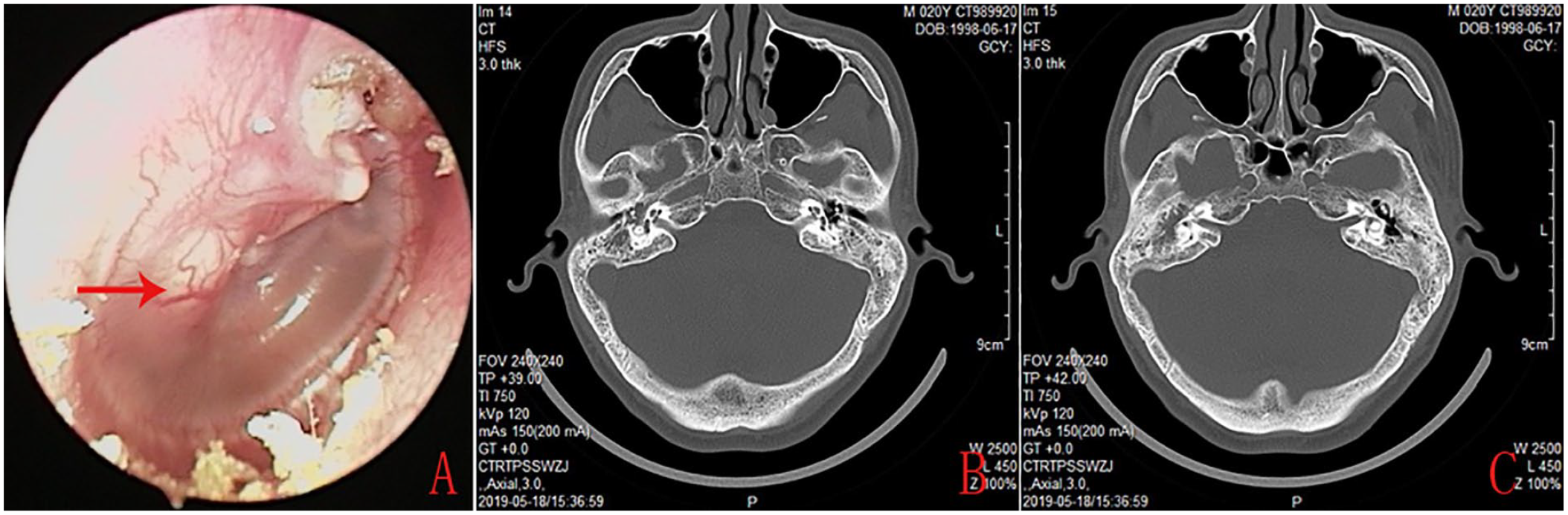
A 41-year-old male’s endoscopy revealed a white mass behind the posterior upper quadrant of an intact TM, and effusion and crusting of the pars flaccida (A). CT revealed soft tissue in the antrum, aditus ad antrum, and tympanic cavity (B and C).
All 3 Group B patients had histories of COM with otorrhea and TM perforation. The middle ears lacked white masses; endoscopy revealed only atrophic TMs and white myringosclerotic plaques.
Of the 10 patients in Group A, ear fullness was the chief complaint (9 ears; 90.0%) at the time of diagnosis, the other symptoms were hearing loss (6 ears, 60.0 %), tinnitus (4 ears, 40.0%), and otalgia (3 ears, 30.0%). All 3 Group B patients complained of hearing loss but only 1 complained of concurrent tinnitus.
In all patients, CT of the temporal bone revealed soft tissue masses in the middle ear and/or mastoid cell. No patients exhibited definite scutal erosion. In the 3 patients of Group B, the cholesteatomas were confined to the antrum and aditus ad antrum in 2 but extended to the epitympanum in 1. All 10 patients in Group A evidenced extensive cholesteatomas with intact (noneroded) malleoli, including 5 with wide extensions into the anterior epitympanum, the posterior middle ear, and the mastoid antrum; 2 with wide extensions into the anterior epitympanum, the mastoid antrum, and the mastoid cells; and 3 with extensions into the anterior epitympanum and the posterior middle ear. Eight patients exhibited cholesteatoma sacs distant from the partes flaccidae; in 5, the sacs were in contact with the partes flaccidae but were easily separated. Two patients exhibited facial canal dehiscence in the tympanic segment; these became evident after removal of the cholesteatoma sacs lying over the facial canals.
Of the 10 patients in Group A, 8 underwent canal wall up mastoidectomy (CWUM) combined with ventilation tube (VT) insertion; 1 with a low-lying dura underwent canal wall down mastoidectomy (CWDM), and 1 underwent CWUM only. Ossicular chain reconstruction was performed contemporaneously in 50% (5/10). Of the 3 patients in Group B, 2 underwent CWUM combined with cartilage myringoplasty and 1 CWUM only.
All patients were followed up for 24 months (average of 28.3 ± 3.6 months). The TM perforations closed in all patients. We encountered no residual cholesteatomas and no recurrence during follow-up. Of the 10 patients in Group A, the average air–bone gap was 35.3 ± 9.6 dB before operation and 12.8 ± 5.4 dB after operation. Postoperatively, all patients exhibited intact TMs without retraction pockets. Of the eight patients with VTs, the tubes extruded in two, 4 and 7 months after surgery; all VTs were removed at 12 months. Of the 3 patients in Group B, the average air–bone gap was 27.0 ± 2.67 dB before operation and 11.33 ± 1.68 dB after operation.
Discussion
The mechanism of ITMC development remains unclear. Most scholars consider that childhood ITMC may originate from residual epidermoid cells incorporated into the middle ear during embryonic development.8,9 The 2 theories of adult (acquired) ITMC development are the inclusion theory of Tos 10 and the middle-ear mucosal metaplasia theory of Sadé. 11 The acquired inclusion theory postulates that viable, keratinized epithelial cells of a retracted TM attach to the malleus and remain in the tympanic cavity; the retracted TM then heals. 12 It has also been speculated that keratinized squamous epithelium may become implanted in the tympanic cavity via the perforation edges, followed by TM healing.2,13 However, few studies have evaluated ITMC patients with OME, with the exception of 2 patients examined by Matsuzawa et al. 12 In the present study, 10 patients with ITMC had histories of persistent OME and 3 had histories of TM perforation and otorrhea. The cholesteatomas were located in the anterosuperior quadrants in 6 of the 10 patients with OME and the posterior upper quadrants in 3. The cholesteatomas lay in the antrum and aditus ad antrum in all 3 patients with atrophic TMs. We speculate that cholesteatomas in the anterosuperior quadrant may have arisen after ectopic implantation of squamous epithelium introduced into the tympanic cavity by a puncture needle. However, cholesteatoma formation may reflect inadequate ventilation of the middle ear. ET dysfunction disturbs middle-ear ventilation, triggering mucosal edema and/or the proliferation of granulation tissue in the tympanic cavity, further compromising ventilation and drainage of the ET, middle ear, and mastoid cells, thereby inducing cholesteatoma. Another possible mechanism is middle ear, mucosal squamous metaplasia attributable to COM. 14
OME with an intact TM usually results in misdiagnosis of ITMC. All patients of the present study had been misdiagnosed. Although audiometry revealed conductive hearing loss in all 13 patients, ear fullness was the chief complaint in the 10 patients with OME but hearing loss was the principal complaint in the 3 patients with atrophic TMs. Endoscopy revealed white masses behind the TMs and intractable OME in 10 patients, but minimal pars flaccida retractions; 7 exhibited partes flaccidae of type I or II; and 3 pars tensa retractions with pars flaccida crusting. Matsuzawa et al. 12 reported closure of pars flaccida retraction pockets in 3 patients with ITMC. Lee et al. 3 and Kim et al. 4 reported ITMC patients with tiny retractions of the partes flaccidae.
Thus, ITMC should be suspected if the hearing loss is greater than expected, given the preexisting disease, or a new symptom develops. Although the TM is intact with or without pars flaccida retraction in patients with OME or histories of perforation, CT/MRI should be performed. Jaisinghani 15 suggested that TM and middle-ear pathologies are significantly correlated. Evident TM pathology, alone or in combination with another pathology, may be a strong indicator of underlying middle-ear pathology. However, a normal TM does not exclude the possibility of middle-ear pathology.
Most scholars believe that ITMC should be treated via CWUM. Di Lella 1 reported on 27 ITMC patients treated via CWU (44.4%), tympanoplasty (44.4%), and CWDM (11.2%). In Lee et al., 3 only 2 ITMC patients with low-lying durae underwent CWDM and 9 underwent CWUM. Kim et al. 4 treated 3 ITMC patients via CWUM. Of our 3 patients with atrophic TMs, 2 underwent full-thickness cartilage myringoplasty and CWUM and 1 CWUM alone. Full-thickness cartilage grafting may prevent TM reperforation and atrophy. Of the 10 patients with OME 1 underwent CWDM because of a low-lying dura, 1 CWUM alone because the postoperative ET function was good, and 8 CWUM combined with VT insertion. An ITMC with OME is similar to a cholesterol granuloma (CG). Mastoidectomy alone may be inadequate because ET dysfunction is difficult to treat. CWUM combined with VT insertion may avoid postoperative negative pressure in the middle ear and thus prevent cholesteatoma recurrence. VT insertion effectively compensates for ETD. 16 No remnant or recurrent cholesteatoma was found during follow-up. Ou et al. 17 divided 49 patients with CGs into CWUM, CWUM/VT insertion, and CWUM/balloon dilation Eustachian tuboplasty groups, and the treatment effectiveness rates were 37.5%, 73.68%, and 90.91%, respectively, over 2 years of follow-up. Maeta et al. 16 believed that VT insertion and thorough mastoidectomy were essential to treat CGs and TM retractions, CWUM alone inadequately controls CGs, and that both CWUM and VT insertion are needed. The limitations of this study included the small sample and the fact that the times of initial onset were not known.
Conclusions
ITMC should be suspected if symptoms worsen or new symptoms develop in adults with OME or a history of perforation, although the TM is intact and lacks pars flaccida retraction. HRCT/MRI should be performed. CWUM combined with VT insertion effectively treats ITMC with OME.
Footnotes
Author’s Note
Author Contributions
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Health Commission of Zhejiang province, China (Grants#2021KY1186) and the Science and Technology Agency of Yiwu city, China (Grants#2018-3-76).
Availability of Data and Material
All data generated or analyzed during this study are included in the published article.