
Abstract
Background and Objective:
The aim of this study was to investigate the factors affecting extrusion time in both children and adults with ventilation tube (VT) insertion, providing useful information for clinicians for better decision-making, follow strategy, and potentially improve clinical outcomes for these patients.
Methods:
Data from patients receiving myringotomy with VT insertion from January 1, 2007, to June 30, 2012, were retrospectively collected and analyzed by the end of 2018. Various factors, including age, gender, history of VT insertion, tympanogram, size of VT used, local finding of tympanic membrane, hypertension, diabetes mellitus, hyperlipidemia, and postoperative ear infection, were included and analyzed to examine the effects of these factors on extrusion time.
Results:
A total of 447 patients were included in this study (Child group–Adult group = 237:210). The overall average extrusion time was 225.85 days. In the subgroup analysis, the average time was 221.3 days and 231.0 days for children and adults, respectively. The results showed that the VT extrusion time was significantly longer in participants without a history of VT insertion and in those where larger sized VTs were inserted in both age-groups. Male gender had an influence on extrusion time in children. In addition, a history of VT insertion and VT size were determined to be factors related to extrusion before 12 months in children.
Conclusion:
History of VT insertion and VT size were significantly related to VT extrusion time in both children and adults and defined as factors associated with extrusion before 12 months in children. The findings suggest avoiding VT with a diameter < 1 mm and considering an appropriately larger size in patients with a history of VT insertion to optimize VT retention.
Introduction
Ventilation tube (VT) insertion is a surgery that involves placement of a small tube in the tympanic membrane to ventilate the middle ear cleft. It is the most common procedure to treat middle ear effusions (MEEs) that persist after conservative management with or without medication for 2 to 3 months.1-3 Placement of a VT significantly improves hearing function, reduces symptoms of MEEs, reduces the incidence of recurrence, and provides drainage and administration of topical antibiotics for persistent MEEs, which increase the overall quality of life of patients. 4
Typically, the VT stays in place for 6 to 12 months before extrusion, followed by the spontaneous healing of the insertion site. 5 Approximately 20% of patients develop recurrences of MEEs after tube extrusion, and the longer the tympanostomy tube retention time, the lower the recurrence rate of MEE. 6 Understanding the factors affecting VT extrusion time has become a clinically important issue, as physicians would like to avoid premature VT extrusion to maximize the effectiveness of this procedure.
Factors affecting VT extrusion time have been reported previously.7-10 It is generally accepted that they are the tube shape, size, material, a history of previous VT insertion, the status of the tympanic membrane, episode of otorrhea, and infection. Although there have been various studies investigating the factors that affect extrusion time of VT with different characteristics, most of these studies exclusively examined factors in the children, and no study has screened adults with distinctive characteristics (such as comorbidities). Our study included comprehensive factors related to VT extrusion time from previous studies and examined these factors in both adults and children. By identifying the predisposing factors that might influence the effectiveness of VTs, surgeons can make a better decision in selecting the appropriate VT considering the various characteristics to prevent premature VT extrusion. The objective of this study was to evaluate the potential factors affecting VT extrusion time, with particular emphasis on subgroup analysis between children and adult patients.
Materials and Methods
Study Population
Data from patients receiving myringotomy with VT insertion from January 1, 2007, to June 30, 2012, at Taipei Medical University Wan-Fang Hospital, Taipei Medical University Hospital, and Taipei Medical University Shuang-Ho Hospital, were retrospectively collected and analyzed by the end of 2018. Criteria for VT placement was according to management guidelines in “Management of Acute Otitis Media,” 2004. Patients who are refractory to antibiotic treatment, with complications of otitis media, and immunocompromised are indicated to VT placement. 11 After excluding patients with missing data regarding VT extrusion time, congenital anomalies, and removal of VT before spontaneous extrusion, 447 myringotomies with VT insertion procedures were collected, including 219 left-eared cases and 228 right-eared cases. Patients were divided into 2 groups: children (< 18 years old) and adults (≥ 18 years old). The average age of patients in the children group was 7.2 years old, and the male–female ratio was 1.6: 1. The average age of patients in adults group was 55 years old, and the male–female ratio was 1.2: 1.
Measures
We defined the date of the operation as D1, the date when the VT was last seen at the last outpatient visit as D2, and the first outpatient visit date when the tube was no longer present as D3. We then defined the extrusion time of the VT as the median of (D2−D1) and (D3−D1).
Demographic and patient factors included age, gender, history of VT insertion, tympanogram, size of VT used, local finding of the tympanic membrane (TM status), hypertension, diabetes mellitus, hyperlipidemia, and postoperative ear infection. Tube diameter included 4 different sizes: (1) inner diameter (I.D.) 0.89 mm, Fluoroplastic, Reuter Bobbin, Micromedics; (2) I.D. 1.0 mm, Fluoroplastic, Reuter Bobbin, Micromedics; (3) I.D. 1.02 mm, Fluoroplastic, Reuter Bobbin without Flange holes, Medtronic Xomed; and (4) I.D. 1.27 mm, Fluoroplastic, Collar Button, Micromedics.
Analysis
Data were analyzed using SPSS version 9.4 (IBM). Descriptive statistics were expressed as mean ± standard deviation (SD). Univariate and multiple regression analyses were done by including extrusion time (days) as a dependent variable and patient factors, including age, gender, history of VT insertion, tympanogram, size of VT used, local finding of the tympanic membrane, hypertension, diabetes mellitus, hyperlipidemia, and postoperative ear infection, as independent variables.
Logistic regression analysis was further used to obtain the odds ratio of the extrusion time lasting for more than 12 months in these patients. The timing of 12 months was chosen as the appropriate intubated period for healing otitis media with effusion (OME) in children as it was demonstrated to be between 12 and 18 months as reported by Osama et al. 12 Independent variables that were adjusted for logistic regression include age, gender, history of VT insertion, tympanogram, size of VT used, local finding of the tympanic membrane (TM status), hypertension, diabetes mellitus, hyperlipidemia, and postoperative ear infection. Both univariate logistic regression and multivariate logistic regression were performed. A P value < .05 was considered statistically significant.
Results
Patient Demographics and Descriptive Statistics
A total of 447 patients were included in this study (Child group–Adult group; 237: 210). Histograms for the children group and the adult group are shown in Figure 1A and B, respectively. The average age of patients in the children group was 7.2 years, and the average age of patients in the adults group was 55 years.
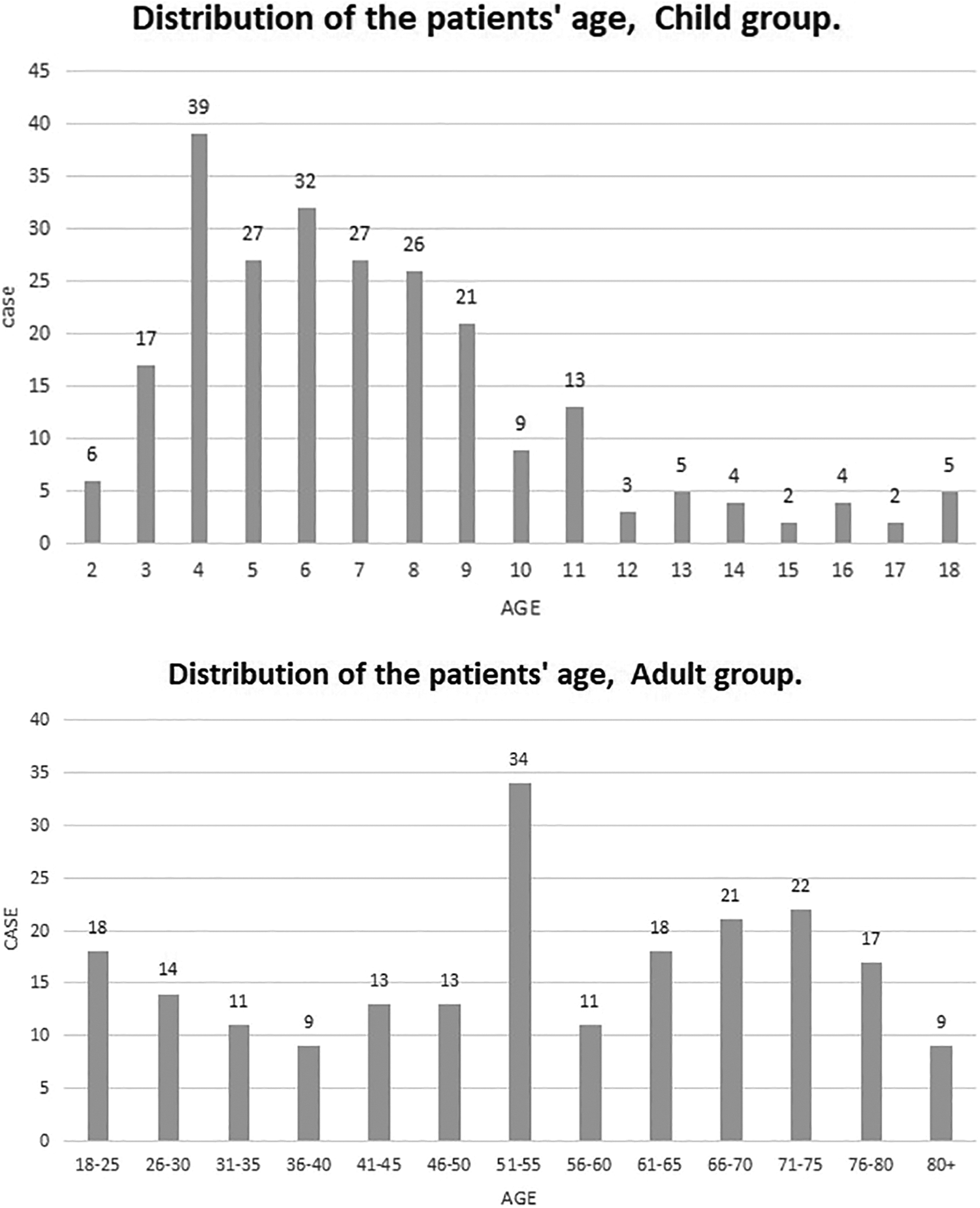
Distribution of the patients’ age, child group.
Figure 2 demonstrates the general and subgroup distribution of the extrusion time after surgery. The overall average extrusion time was 225.85 days (Std = 173.46, Median = 191.50). The extrusion time was between 50 and 250 days in nearly 60% of cases and was longer than 1 year in nearly 14.7% of cases. In the subgroup analysis, the average time was 221.3 days (Std = 159.9, Median = 196.0) and 231.0 days (Std = 187.1, Median = 182.5) for children and adults, respectively.
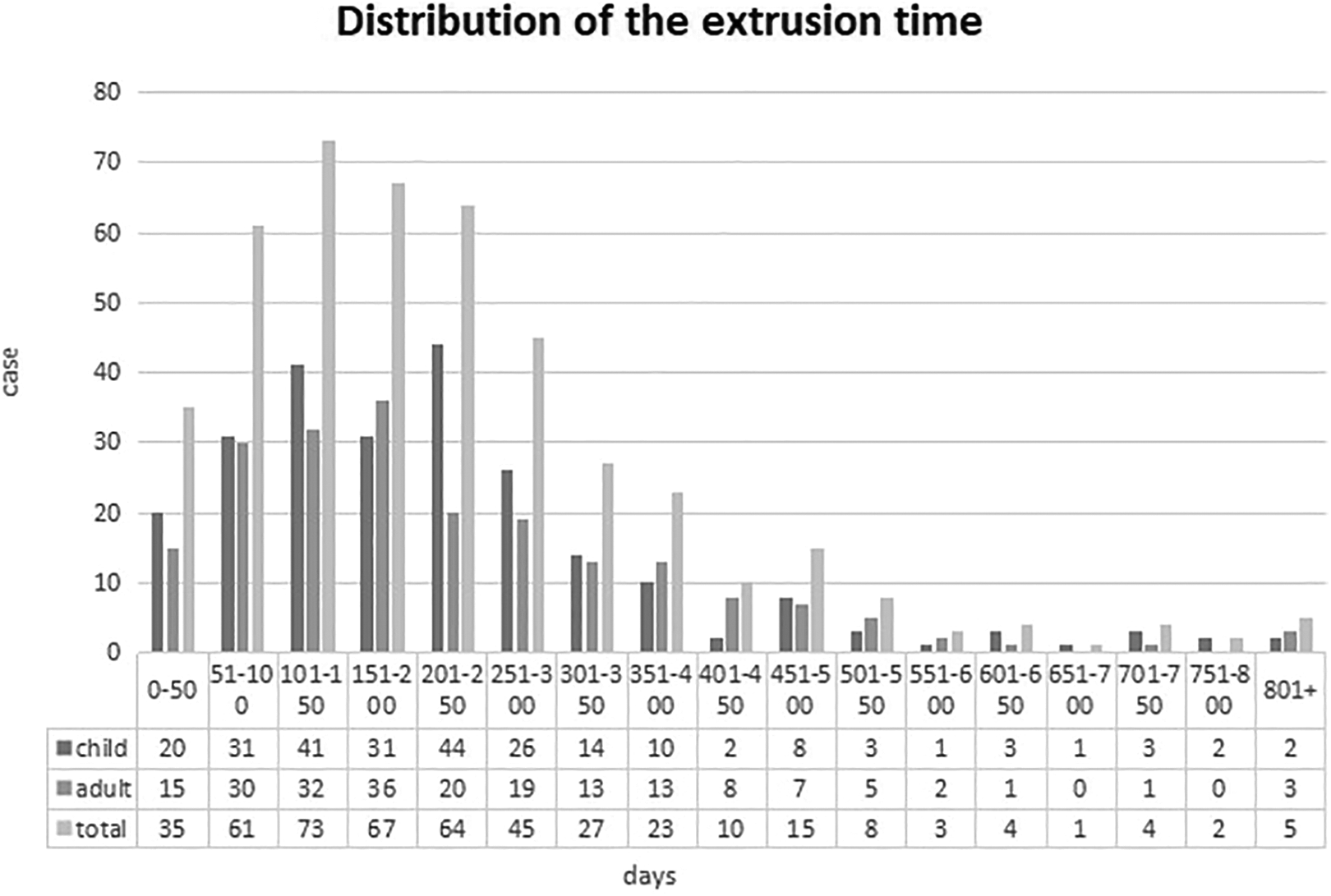
The overall average extrusion time was 225.85 days (Std = 173.46, Median = 191.50). In the subgroup analysis, the average time was 221.3 days (Std = 159.9, Median = 196.0), and 231.0 days (Std = 187.1, Median = 182.5) for children and adults, respectively.
Factors Affecting the Overall VT Extrusion Time
Upon univariate linear regression analysis, we found that gender, history of VT insertion, tympanogram, TM status, and postoperative ear infection significantly affected the extrusion time in patients overall (Table 1). Patients with predisposing factors, such as male gender, no history of VT insertion, type B tympanogram, using larger sized ventilation tube(s), presence of MEEs, presence of gluey middle ear effusion, and no post-operative ear infections, had longer extrusion times compared to those without predisposing factors. Further subgroup analysis shows that, in children, only gender, history of VT insertion, tympanogram, and tube size affected the extrusion time. However, in the adults, only VT size was found to have significantly affected extrusion time (Table 1).
Factors Affecting VT Extrusion Time by Univariate and Multiple Regression Analysis.a
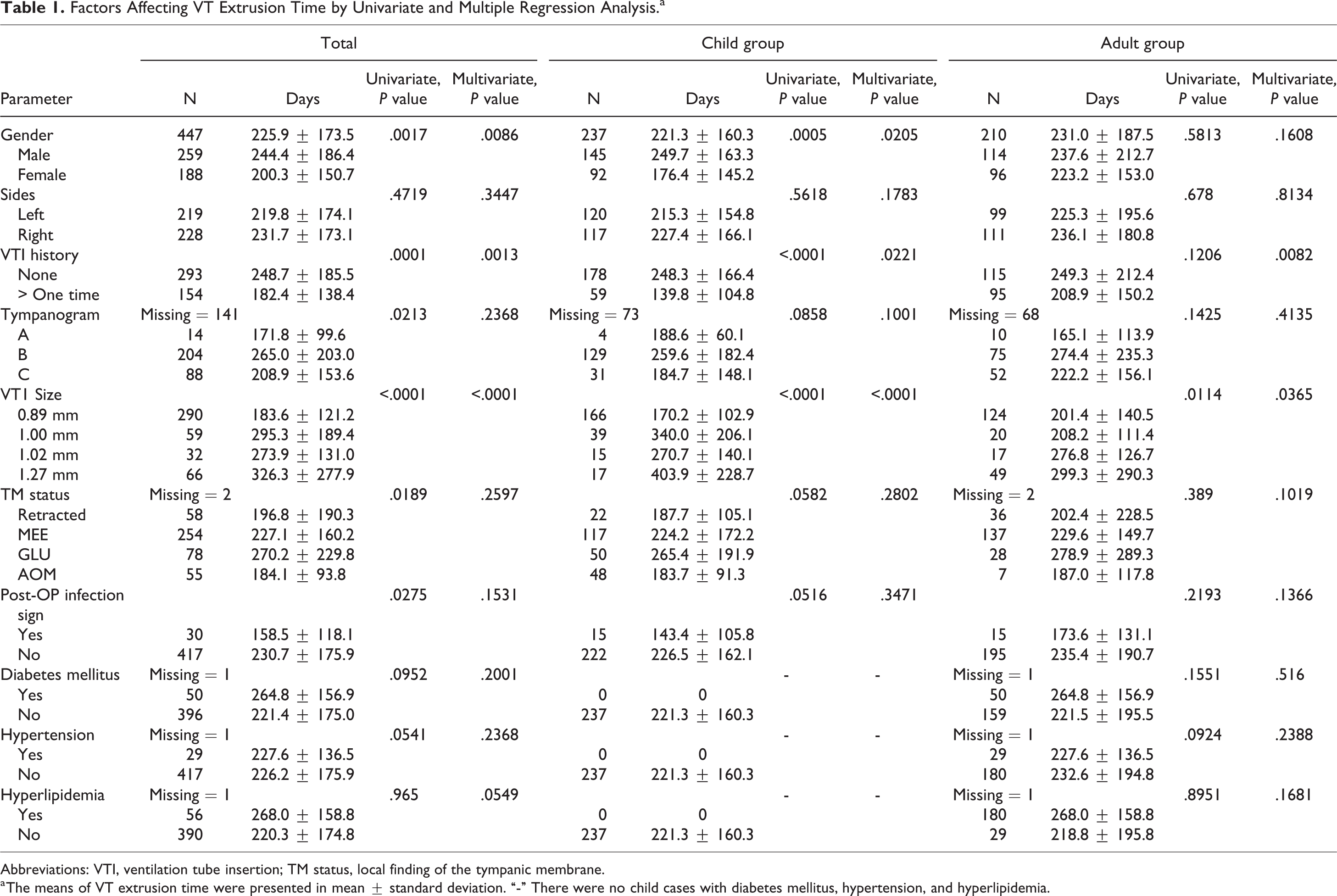
Abbreviations: VTI, ventilation tube insertion; TM status, local finding of the tympanic membrane.
a The means of VT extrusion time were presented in mean ± standard deviation. “-” There were no child cases with diabetes mellitus, hypertension, and hyperlipidemia.
For multivariate linear regression, history of VT insertion and VT size were associated with extrusion time in both groups. Gender was also a significant factor when considering all patients, and in children, but not in the adults, females were more likely to have a shorter VT extrusion time.
Factors Affecting the Chance of Sustaining the VT for More Than 12 Months
Under the settings of sustaining the VT for more than 12 months as the goal, the results from the univariate logistic regression model demonstrated that children who had no previous VT insertion history or who were inserted with a VT size larger than 0.89 mm had VT extrusion times longer than 12 months (Table 2). These factors remained statistically significant under multivariate logistic regression (Table 3).
Factors Affecting the VT Sustaining for More Than 12 Months by Univariate Logistic Regression in Both Child and Adult Groups.a
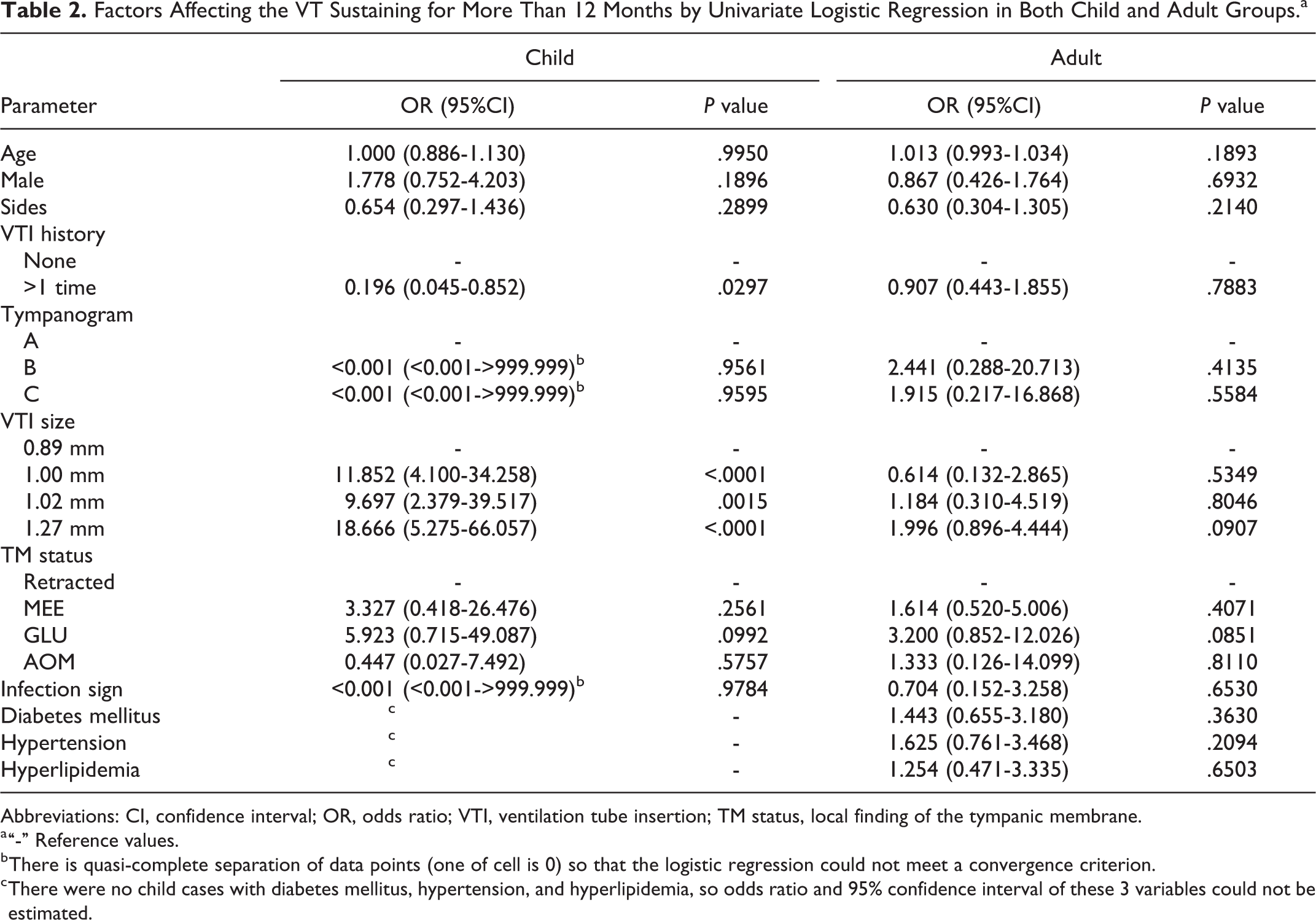
Abbreviations: CI, confidence interval; OR, odds ratio; VTI, ventilation tube insertion; TM status, local finding of the tympanic membrane.
a “-” Reference values.
b There is quasi-complete separation of data points (one of cell is 0) so that the logistic regression could not meet a convergence criterion.
c There were no child cases with diabetes mellitus, hypertension, and hyperlipidemia, so odds ratio and 95% confidence interval of these 3 variables could not be estimated.
Multivariate Logistic Regression by Stepwise Selection for Children Group.a
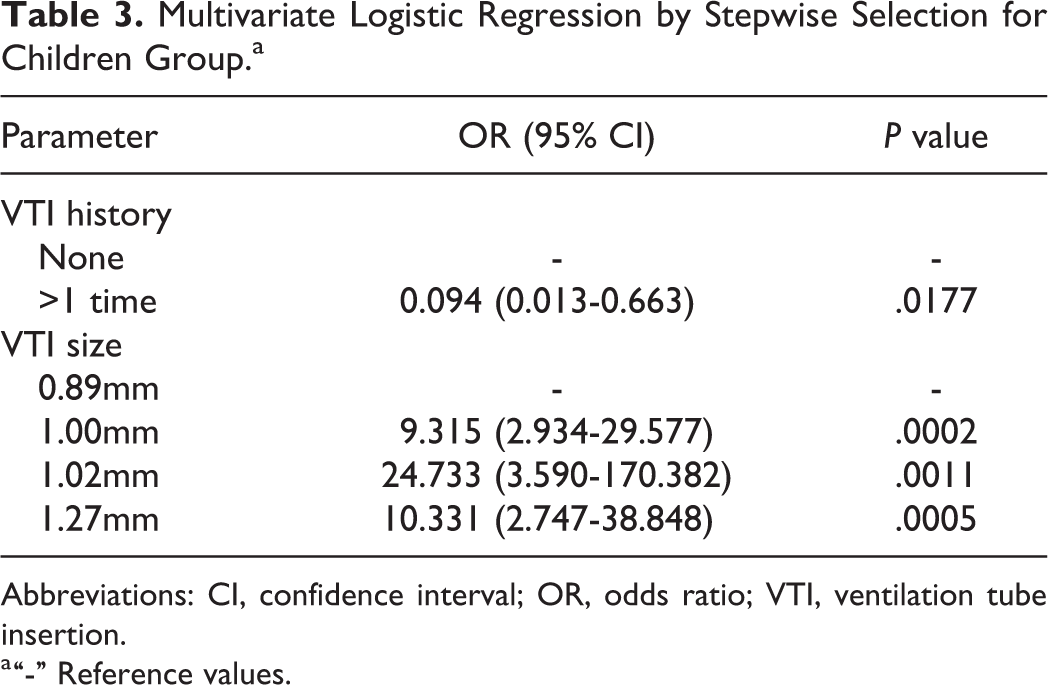
Abbreviations: CI, confidence interval; OR, odds ratio; VTI, ventilation tube insertion.
a “-” Reference values.
In the adults, no variables were identified to significantly contribute to extrusion times longer than 12 months with either univariate or multivariate logistic regression analysis.
Discussion
Through this study, we have demonstrated that the VT extrusion time was significantly longer in participants without a previous history of VT insertion and in those in who larger sized VTs were inserted in both age-groups. Male gender had an influence on extrusion time in the children. In addition, previous VT insertion and VT size were determined to be factors related to extrusion before 12 months in children.
Well known and popularized for decades, old-fashioned VT insertion still plays an important role, as newer techniques, such as laser myringotomy, appear to sustain a significantly shorter time of tympanic membrane fenestration. Zong et al reported that laser myringotomy, with an effective sustained duration of between 5 days and 5 weeks, was found to be associated with much higher recurrence rate of OME, fewer complications, and less effectiveness than myringotomy with VT insertion in keeping the middle ear ventilated and relieving MEE. 13 The most extended effective duration ever reported for the laser myringotomy was 3.5 months, as reported by D’Eredità et al and obviously much shorter than what a VT can sustain. 14
Ventilator tubes are usually extruded naturally from the tympanic membrane approximately 6 to 24 months after tube insertion. If the tubes extrude early, patients might require an additional insertion and increase the incidence rate of recurrence of otitis media due to insufficient effects of treatment. 6 Osama et al showed a significantly higher recurrence rate of MEEs when the tubes were removed before 12 months from the insertion. 12 Iwaki et al confirmed that the recurrence rate was significantly lower if the tube was inserted longer than 12 months, and MEE was less likely to recur with longer VT duration. 5 Several studies have also examined VT extrusion time and predisposing factors; however, most of these studies were focused on children only, and little has been explored in comparing the children with the adults in revealing the predisposing factors that might influence the effectiveness of VTs. The findings in our study may be of considerable clinical relevance, providing a useful guide to surgeons in the selection of the appropriately sized of VTs in cases with a high-risk of premature VT extrusion.
The finding that patients with a previous history of VT differ significantly in VT extrusion time in both age-groups is consistent with other studies, where VTs remained longer in patients without previous VT insertions. 10 Although the mechanism behind VT extrusion is not fully understood, it suggests that tympanic membrane characteristics affect extrusion time. Sequelae related to previous VT insertion include scarring and atrophy resulting from the loss of the middle fibrous layer of the healed tympanic membrane. 15 This might change the elasticity of the tympanic membrane and increase the risk of early VT extrusion. Specifically, our study showed that a history of previous VT was associated with extrusion before 12 months in children, and clinicians should consider choosing an appropriate VT size to prolong tube maintenance in this population. Our results also revealed that postoperative ear infection caused earlier extrusion of VT in patients overall. A case–control study by Ma et al stated that regular biofilm exfoliation surgery after VT insertion could elongate the retention time of VT. 16 It should be noted that, in our study, we used all fluoroplastic tubes, and the impact of different materials is not addressed. The influence of the VT materials on the extrusion time has also been discussed in the past literature. The study by Dingle et al and Shone et al demonstrated that the duration for the tube to be in place and functional was longer for titanium VTs compared to Teflon VTs.17,18 However, it was also demonstrated that, as long as the middle ear cavity remained healthy, no significant difference was seen for transient dysfunction and tube extrusion rates between fluoroplastic and titanium tubes, although better biocompatibility was observed for the titanium tubes. 19 While titanium tubes might be the better choice for adult patients lacking Eustachian tube dysfunction and OME, Handler et al proposed that there were no differences in extrusion times between titanium VTs and silicone VTs and addressed the issue regarding the considerable cost differences between these 2 types of tubes. 20
The present study found that the extrusion process happened more quickly in smaller tubes than in larger ones in adults and children. Similar to our result, Michael et al recommend choosing an appropriate VT size according to short-term or long-term purposes, as tubes with a diameter of approximately 1.1 mm maintain for 1 year and 1.5 mm tubes maintain for more than 1 year. 21 In our study, a VT diameter larger than 1 mm was also found to increase the chance of maintaining the VT in place for more than 12 months in children. Therefore, a different tube size should be considered when a prolonged ventilation duration is required, and we recommend avoiding the usage of VTs with diameters less than 1 mm in children to prevent early extrusion. Interestingly, a more recent article by Kim et al demonstrated that there was a significant increase in the time to extrusion in ears where a 1.02 mm-sized thermoplastic elastomer VT was inserted compared to that in the 1.14 mm-sized silicone VT. The authors stated that although, generally, the larger inner diameter of the tube lasts longer in the eardrum, the contrasting result is thought to be due to the different material properties of both VTs. However, the authors also mentioned that thermoplastic elastomer VTs had more plugging events than silicone VTs, which is probably due to the smaller diameter. 22 Therefore, we believe all these factors, including patient condition, tube diameter, and tube materials, must be considered together for the readers to decide which VT would be best according to patients’ clinical conditions and needs.
The study has several limitations. First, because of the retrospective study, missing data in some variables can reduce the statistical power of research and produce biased estimates. The second limitation of the study is the distribution of age among participants. The patients were mostly older adults and children, so we combined all participants who were ≥18 years old in one group. Comorbidities, such as hypertension, diabetes, and hyperlipidemia, tend to occur in middle-aged and older adults and may cause bias of analysis and lack of significance in the variables of interest. Further investigations of more factors affecting the extrusion time in the older adults group are needed. Also, it should be noted that some of the extrusion time data in this study are quite extreme such as more than 500 days or less than 50 days. However, as these outliers represent only a minority of total case numbers, we believe this would have little impact on our study result.
Conclusion
Our study revealed factors that shorten VT extrusion time, including history of VT insertion, using a smaller size of VT regardless of age, and in children, female gender. Children with a history of VT insertion or inserted with a smaller size of VT were more likely to have extrusion before 12 months than its counterparts. No other comorbidity factors influenced the VT extrusion time in the adult population. We recommend that clinicians consider these factors before performing VT insertions to better control or predict the VT extrusion time.
Footnotes
Authors’ Note
Yi-Chih Lin and Yi-Ling Kao contributed equally to this study. This is an individual study, and all financial and material support was self-sponsored.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.