
Abstract
Spontaneous intracranial hypotension (SIH) is a rare condition characterized by orthostatic headache, pulsatile tinnitus, vertigo, nausea, and fluctuating hearing loss; this latter seems to be due to the development of cochlear endolymphatic hydrops following negative cerebrospinal fluid (CSF) pressure transmitted to the perilymphatic space through a patent cochlear aqueduct. We here describe a case of bilateral progressive sensorineural hearing loss (SNHL) due to intracranial hypotension caused by an undiagnosed spontaneous CSF leak from a skull base defect in a middle-aged woman. To the best of our knowledge, this is the first report describing a SNHL in a patient affected by SIH secondary to sphenoidal CSF leak.
Introduction
Acquired sensorineural hearing loss (SNHL) can be due to multiple causes such as aging, trauma, noise exposure, infections, ototoxic drug consumption, vascular and autoimmune disorders, and endolymphatic hydrops (EH).
EH is a well-established cause of SNHL.1 -3 It is defined as an enlargement of the endolymphatic space due to increased endolymph volume 4 ; typical symptoms are fluctuating hearing loss and episodic vertigo. It can be considered a primary disorder, as occurring in Meniere disease or secondary to trauma, infections, inflammatory processes, and changes in cerebrospinal fluid (CSF) pressure.5,6
According to the available literature, spontaneous intracranial hypotension (SIH) can determine EH.2,6,8 -13 The pathogenetic mechanism is still unexplained, but it is likely related to the anatomical connections between the inner ear and the subarachnoid space through the cochlear aqueduct (CA), a small bony canal that can vary in length and size, 7 and through the vestibular aqueduct (VA).
SIH is rare and frequently misdiagnosed; it occurs in approximately 1 out of 50,000 individuals 14 with a female-to-male ratio of 3:1. 8 It was described for the first time by Schaltenbrand in 1938 and it is characterized by a CSF pressure lower than 60 mm H2O in patients without any history of lumbar puncture or surgery. 2 Three major factors can determine SIH: CSF volume depletion due to any leakage, reduced CSF production or hyper-absorption.15,16 Main symptoms include: orthostatic headache, followed by pulsatile tinnitus, vertigo, nausea, and fluctuating hearing loss; in rare cases it can also present with oculomotor nerve paralysis. 2 Diagnosis can be both clinical, based on symptoms, and radiological, based on typical magnetic resonance imaging (MRI) findings after gadolinium injection, that is, dura mater enhancement, low-lying cerebellar tonsils, reduced ventricular system width, and cortical grooves at the convexity. 17
In this article, we report the first case of bilateral progressive SNHL related to SIH caused by an undiagnosed spontaneous CSF leak from an anterior skull base defect, and we discuss and review the current literature discussing the possible relationship between SIH and EH.
Case Report
A 61-year-old female affected by progressive bilateral SNHL was referred to our outpatient clinic for intermittent serous rhinorrhea treated for few years with topical steroids in the suspicion of vasomotor rhinitis; the patient had a history of blood hypertension under treatment and obesity (body mass index = 31 kg/m2). A fiber optic nasal endoscopy did not document any anatomical alterations or signs suggestive for CSF leakage. The patient was suffering from severe bilateral SNHL, and she was on the waiting list for undergoing cochlear implant surgery. Her hearing loss was progressive over the last 10 years, during which she had referred occasional episodes of objective vertigo and diplopia (Figure 1). During many multidisciplinary examinations (by Ophthalmologist, Neurologist, Audiologist, and Otorhinolaryngologist) she had never mentioned rhinorrhea before. She underwent multiple assessments trying to discover the etiology of the hearing loss, including a muscular biopsy in the clinical suspicion of mitochondrial disease, blood examination (ie, antinuclear antibodies, erythrocyte sedimentation rate, antineutrophil cytoplasmatic antibodies) to exclude any autoimmune disease and various Gd-enhanced brain MRI scans. The last MRI (2019) was neglected by the patient for almost 2 years owing to the SARS-COV2 pandemic. When our neuroradiologists reviewed it in 2021, they observed the presence of typical signs of intracranial hypotension 17 : (1) a widespread thickening of the dura mater associated with a contrast enhancement; (2) the herniation of the cerebellar tonsils from the posterior cranial fossa toward the foramen magnum reaching the posterior arch of C1; (3) a smaller than usual size of the ventricular system, and (4) a poor visualization of the cortical grooves at the convexity (Figure 2).
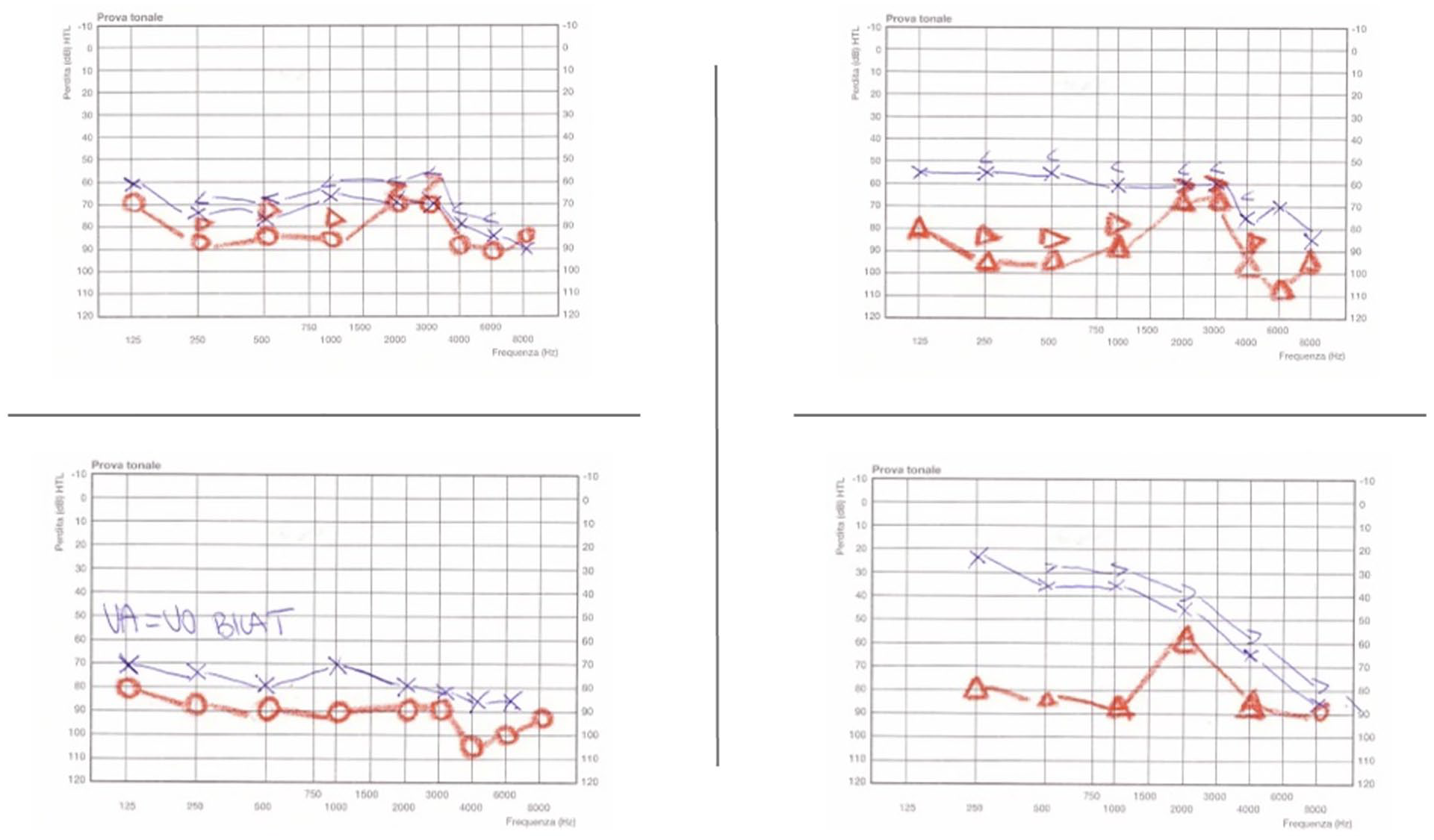
Patient’s hearing tests showing a progressive sensorineural bilateral hearing loss.
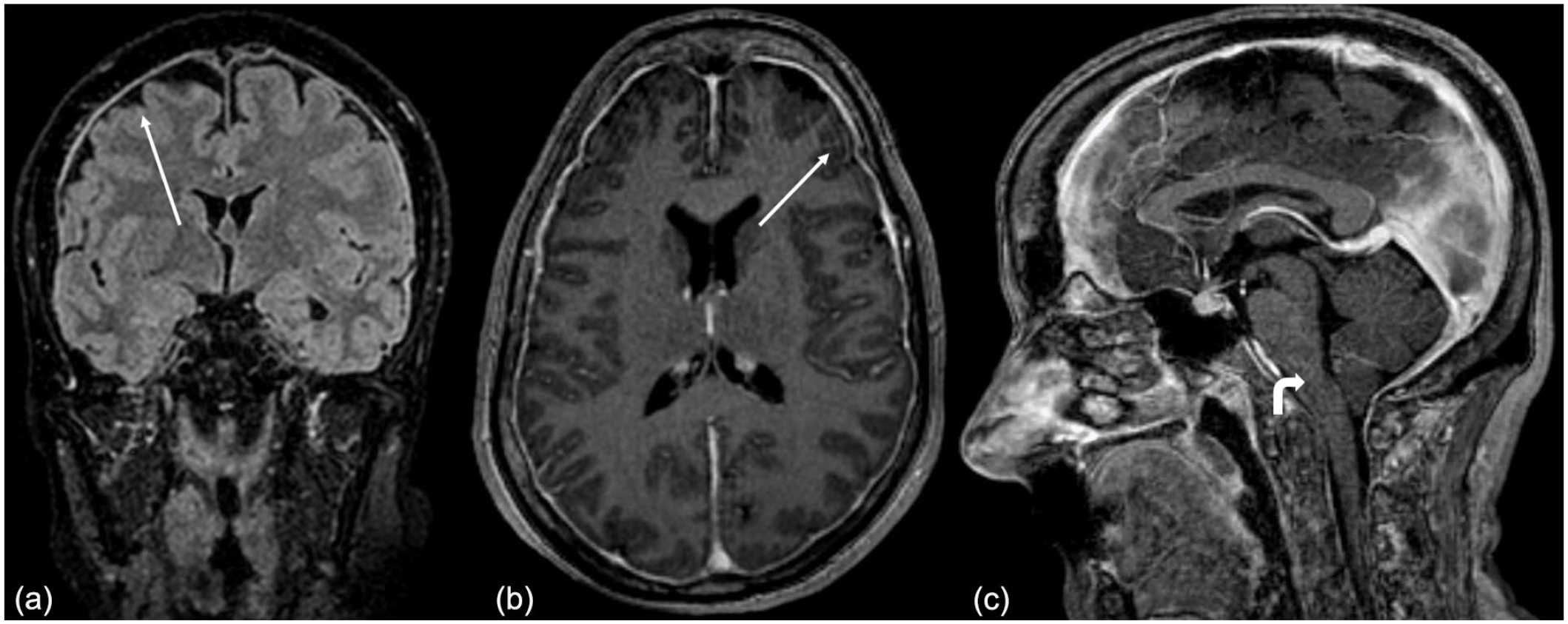
Contrast-enhanced magnetic resonance imaging showing typical radiological findings (white arrows) of intracranial hypotension: dura mater thickening (a) dura mater contrast enhancement (b) cerebellar tonsils tending to herniate toward the foramen magnum.
After having collected all these clinical data, the hypothesis of a skull base CSF leak was forwarded. A new gadolinium (Gd)-enhanced MRI and a maxillofacial CT scan were ordered as well as the search for β-2 transferrin in the nasal discharge.
The CT scan showed 2 possible points of leakage: 1 placed at the lateral wall of the right sphenoidal sinus with concomitant CSF inside the sinus and the other 1 at the posterior wall of the left sphenoidal sinus (Figure 3). The Gd-enhanced brain MRI detected a severe cochleo-vestibular hydrops in the left ear (Figure 4), without any specific sign of CSF leak. The search of β-2 transferrin in the nasal discharge resulted positive.
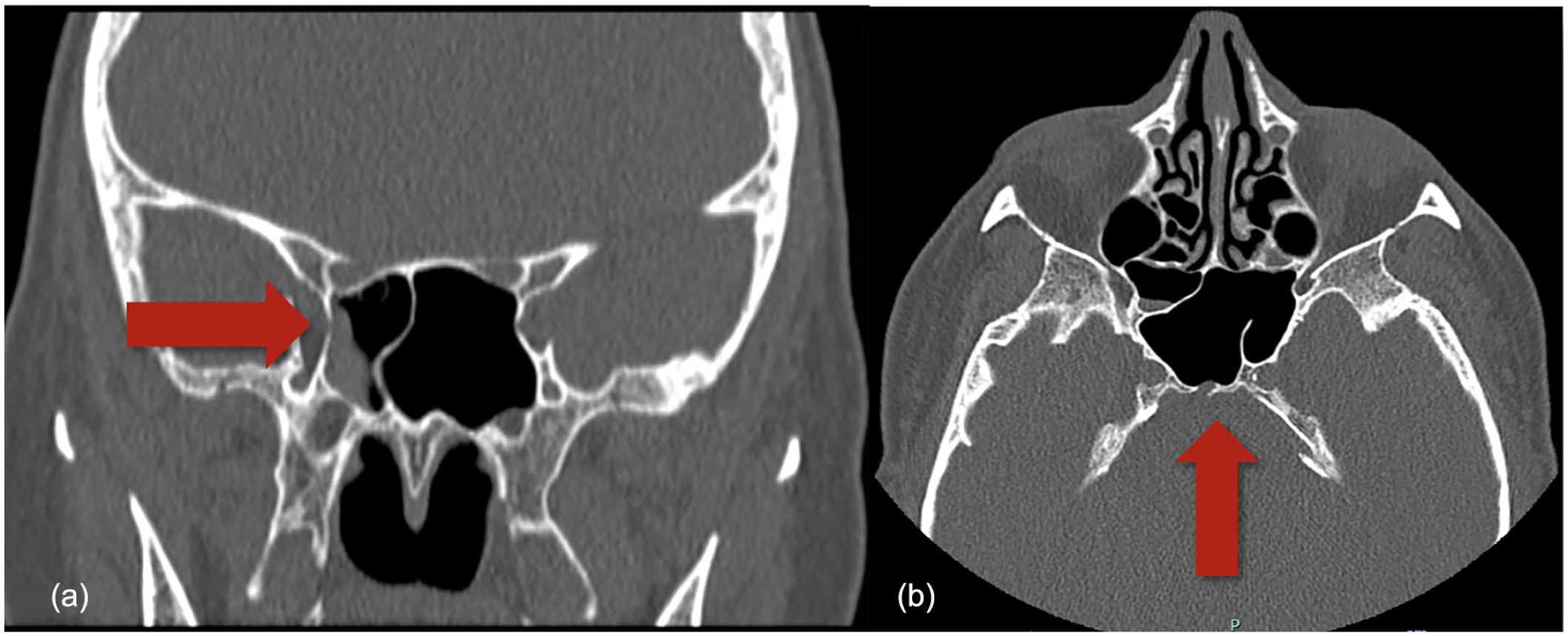
Maxillofacial CT scan showing (red arrows) 2 leakage points on the lateral wall of the right sphenoid sinus (a) and on the posterior wall of the left sphenoid sinus (b).
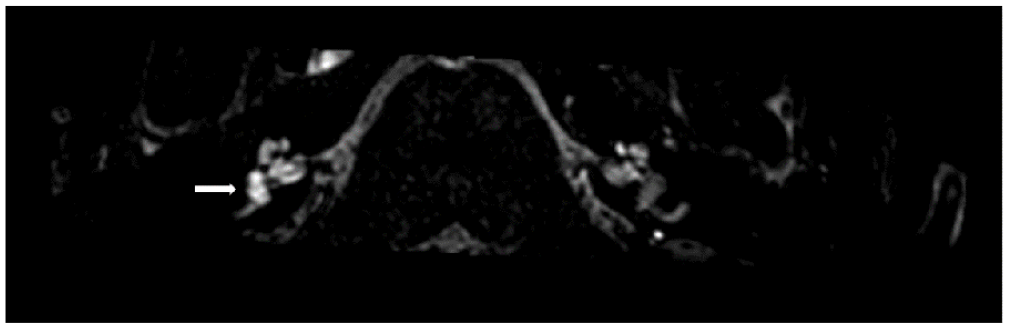
Contrast-enhanced magnetic resonance (MR) images acquired 4 hours after intravenous gadolinium perfusion, showing a severe cochlear-vestibular hydrops on the left ear in T2-3D FLAIR sequences.
Based on these new findings, after a multidisciplinary consultation, we opted not to perform a lumbar puncture because the radiological and biochemical signs were pathognomonic for the presence of a CSF leak; therefore, the patient underwent endoscopic sinus surgery preceded by intrathecal fluorescein injection (4 hours earlier). Intraoperatively, a site of leakage was detected at the posterior wall of the left sphenoid sinus, and it was repaired with an inlay autologous fat graft and a septal bone and naso-septal mucosal overlay flap (Figure 5). No other fistulas were recognized. The postoperative course was uneventful: the nasal packing was removed 48 hours after surgery, and the patient was discharged 2 days after surgery. At the 11-month follow-up assessment, no CSF leak recurrence occurred, and the sinus mucosa appeared well healed.
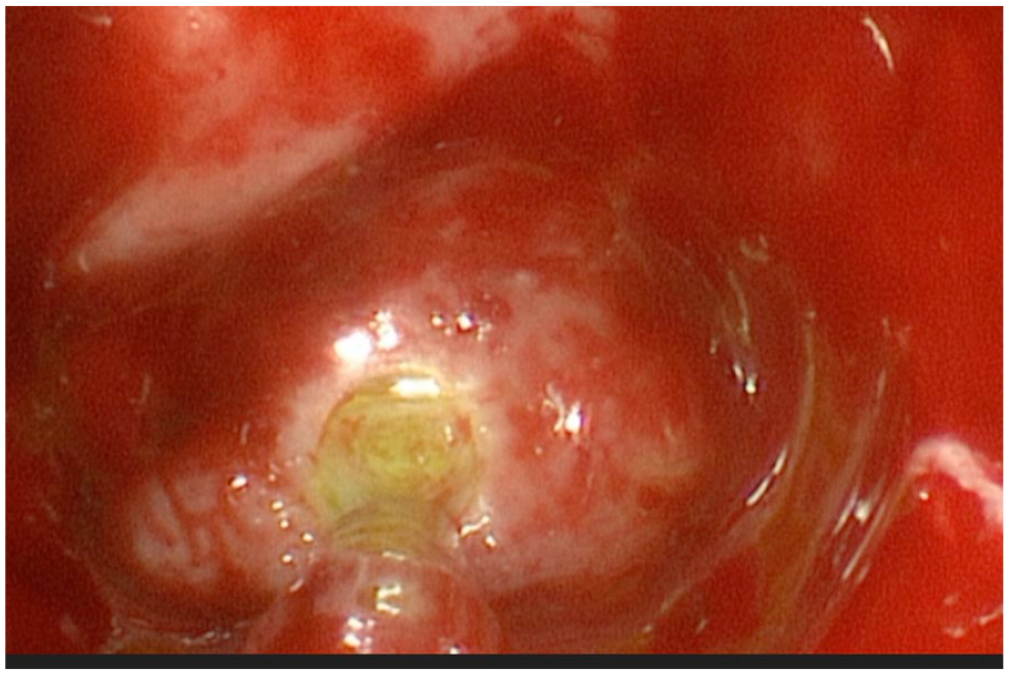
Cerebrospinal fluid leakage on the posterior wall of the left sphenoid sinus detected intraoperatively by means of intrathecal injection of fluorescein.
Postoperative hearing assessment documented that the hearing thresholds remained stable, and the patient is now waiting for cochlear implantation surgery.
Discussion
Inner ear fluids are influenced by CSF pressure through the direct anatomical connection between the subdural space and the endolymphatic space (ie, the CA), and via the VA that ends in a duplication of the dura mater at the posterior cranial fossa (the endolymphatic sac).7,18 The volume of the cochlear fluids, which are uncompressible, is constant because the membranous organ is enclosed within a bony structure; the oval and round windows represent the only 2 openings capable of compliance. The relative volume of the inner ear compartments is always constant: in the case of fluid depletion in one of them, the body responds by implementing the other one. In the event of intracranial hypotension, the negative pressure at the subdural space is transmitted to the perilymphatic space causing perilymph volume depletion. The inner ear compensates by increasing the endolymph volume, resulting in EH.2,7,10,18 In EH the cochlea is the most affected site.4,19 EH can be detected by intratympanic or intravenous gadolin-enhanced 3T MRI. 20 In our hospital the intravenous gadolinium perfusion is preferred because it is less invasive and faster, and it allows to perform bilateral assessment. 21 EH is identifiable 4 hours after injection. 21
The tiny sensorial structures of the inner ear are compliant, within certain limits, but they are also very fragile: an upsurge of fluid determines their alteration and distortion, possibly even resulting in rupture. 1 Under these circumstances, the concomitance of EH will result in hearing loss, which can be solved by restoring the inner ear fluid balance. However, if the EH is prolonged, it could result in irreversible damage. 22 Multiple studies have been published regarding this phenomenon: in 1976, Kimura et al 23 demonstrated that a prolonged EH determines cilia fusion, disorganization of the cuticular bodies, and an apparent loss of contact between the cuticular plate of outer hair cells. In 1987, Nadol and Thornton 22 proved that prolonged hydrops could also cause a reduction in the number of afferent nerve endings of the inner and outer hair cells and a smaller number of synaptic contacts between afferent neurons and inner hair cells.
SNHL in patient affected by SIH is rare,2,6 as EH occurrence with the following SNHL seems to be related to the anatomical conformation of the CA, with EH development only in patients with patent aqueducts.2,24
In literature different cases of intracranial hypotension due to spinal CSF leakage presenting with EH have been reported,2,6,8 -13 but no one related to skull base CSF leak.
In this review, 8 articles were considered for a total of 10 patients (excluding our patient), 4 females, and 6 males; the mean age was of 43.3 (range 29-63). All these patients presented typical clinical and radiological signs of SIH, and all were affected by SNHL. Only in 5 patients (50%) a CSF leakage (located at the spine) was identified; in all the remaining cases no leakage could be detected. Among these, 6 patients were surgically treated by means of blood patch; the remaining 4 patients were treated by means of diuretics, bed rest, caffeine, and Betahistine. In 2 patients8,9 (all presenting symptoms since long time) the hearing threshold did not recovery after treatment. To our knowledge, no cases of EH with concomitant CSF leakage located at the skull base have been reported before.
Under the suspicion of CSF leakage, it is mandatory to search for it (even in the case of previous negative radiological assessment) and exactly locate it. Many diagnostic tools are available for this purpose, such as CT cisternography, contrast-enhanced MR cisternography, radionuclide cisternography (invasive), and other investigations such as or MR cisternography and high-resolution CT 25 (noninvasive). Intraoperatively, the off-label intrathecal fluorescein administration can be used for detecting the leakage.
B-2 transferrin dosage on nasal discharge samples is considered a sensitive, low-cost, and specific diagnostic tool.26,27 Once the leakage is localized, it must be promptly solved to prevent development of complications such as SIH and infections; intranasal endoscopic surgical repair with autologous graft is the treatment of choice. 28
In our case, diagnosis of progressive hearing loss due to intracranial hypotension and consequent EH was achieved by detection of typical radiological signs of intracranial hypotension and severe EH, and radiological\intra-surgical evidence of sphenoidal CSF leakage. In most cases, appropriate and precocious CSF leakage treatment (resulting in restoring physiologic CSF pressure) determines a complete clinical recovery. When the leakage (and the EH) is long lasting, such as in our patient, a permanent cochlear damage had ensued,8,9 and the hearing loss did not improve after surgical closure.
However, according to Mokri, 16 some patients can develop symptoms of intracranial hypotension (IH) after surgical leakage repair: this phenomenon can happen when the leakage is the expression of intracranial hypotension (IH) and acts as spontaneous CSF drainage. This could have been the case of our patient.
In conclusion, our article describes a case of progressive SNHL due to a spontaneous CSF leakage at the sphenoid sinus presenting with progressive sensorineural hearing loss; in this case, chronic intracranial hypotension with concomitant EH have resulted in bilateral hearing loss. A timely recognition of CSF rhinorrhea and an early treatment of the CSF leaks may prevent serious infectious consequences and, in some case, might also stop the auditory degeneration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ST: Advisor and had lectures for GSK and Sanofi srl.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Publication was supported by the Italian Ministry of Health “Ricerca Corrente 2023.”
Ethical and Consent Statement
Not applicable.
Data Availability Statement
Data available on request due to privacy.