
Abstract
Epithelial-myoepithelial carcinoma is an extremely rare tumor of the nasal cavity. We present a case involving a 67-year-old female with symptoms of nasal obstruction and recurrent epistaxis. An investigation with endoscopy and CT was performed. The patient underwent endoscopic surgical resection. Microscopic positive margins were present after extensive resection. The patient underwent radiotherapy utilizing proton therapy and has been disease free for 6 months at follow-up.
Introduction
Epithelial-myoepithelial carcinoma (EMC) is a rare and generally low-grade carcinoma that most often arises in the salivary glands. 1 It is characterized histologically by a mass of epithelial ductal cells encompassed by myoepithelial cells. 2
This is an especially rare case of an EMC occurring in the nasal cavity; only a select few cases have been reported in the literature thus far. Furthermore, this is the first case to our knowledge in which an EMC was treated with proton therapy.
Case Report
A 67-year-old female was evaluated in the ENT clinic with a history of nasal obstruction and recurrent mild epistaxis affecting the right nasal cavity for several months. Endoscopic examination (Figure 1) revealed a friable mass involving the right middle turbinate and adjacent septum. CT imaging was performed (Figure 1) demonstrating the right nasal cavity mass. There was no obvious extent beyond what was clinically apparent. The mass appeared to be confined to the nasal cavity involving the septum and middle turbinate with no obvious bony destruction. An endoscopic biopsy was performed. The pathology was consistent with a diagnosis of EMC, intermediate grade. Because of the rare nature of this tumor the slides were sent for a second opinion to a head and neck pathologist within the same hospital system (Corewell Health) and for a third opinion at the University of Michigan’s Department of pathology. All concurred with the diagnosis of EMC of the nasal cavity. The pathology is shown in Figure 2. The patient underwent a metastatic workup that was negative. The patient was presented at Corewell Health Head and Neck Tumor Board and was staged as T2, N0, M0, with a consensus recommendation for endoscopic resection reserving radiotherapy for failure to completely resect the tumor. The patient underwent endoscopic resection of the tumor under general anesthesia. The resection included the right ethmoid cells, middle turbinate, and adjacent septum which seemed to be the epicenter of the tumor. The pathologist did not feel that a frozen section would be useful in determining margins, so clinical margins were performed with 1 cm of normal-appearing mucosa being resected around the gross tumor. Final pathology revealed a positive margin on the septum both superiorly and posteriorly despite the tissue having a normal clinical appearance. A second endoscopic resection was then performed under general anesthesia removing septal tissue up to the skull base superiorly and to the face of the sphenoid posteriorly. The final pathology for the second procedure demonstrated focal residual carcinoma at the superior extent of the resection. The patient then underwent radiotherapy using pencil beam scanning proton therapy to the nasal cavity and ethmoid sinus. The dose given was 66 cobalt grey equivalents over 33 fractions. The patient successfully completed treatment and has been followed clinically and with repeat CT imaging with no tumor recurrence in 6 months. The patient provided written consent for their information and clinical imaged to be used in a medical publication.

Left image—Endoscopic view of right nasal cavity. Tumor is apparent involving the middle turbinate. MT – middle turbinate, S – septum, LNW – lateral nasal wall. Right image—Coronal CT (Computed Tomography) scan with bone window. The tumor involving the septum and middle turbinate is circled.
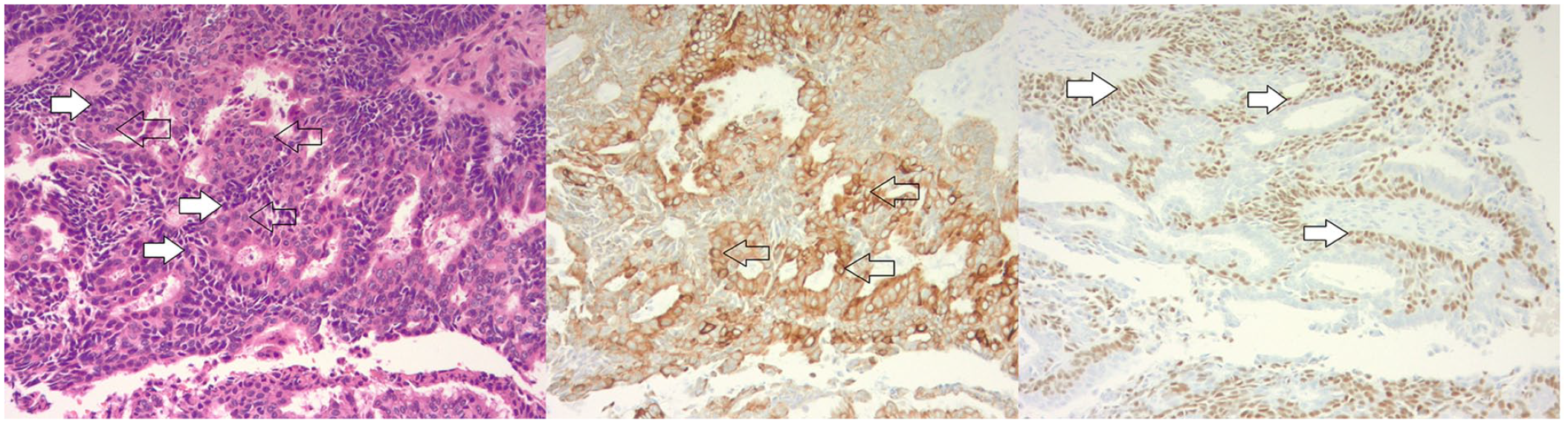
Left image—High power view (100×) demonstrating the biphasic population of tumor cells with moderate nuclear atypia. Black arrows show epithelial cells and white arrows show myoepithelial cells. Center image—Tumor immunostained with Cam5.2. Arrows show highlighted epithelial cells. Right image—Tumor immunostained with P63. Arrows show highlighted myoepithelial cells.
Discussion
The EMC is a rare tumor type, representing approximately 1% of all salivary gland neoplasms. 2 EMCs are disproportionately present in white women older than 50 years, which is in agreement with the present case. 3 EMCs are usually low-grade adenocarcinomas with low metastatic potential, most often presenting as solitary tumors. 4 As such, patients most often present with an EMC of T1-T2 status. 3 T1 EMCs are associated with significantly longer survival relative to higher staging. 3 5-year and 10-year survival rates are 72.7 and 59.5% for EMCs overall, respectively. 2 Furthermore, survival in patients with low-grade EMCs was found to be significantly better than in high-grade tumors. 4
EMCs are most frequently native to the parotid (57.7%) and submandibular glands (9.8%). 5 Other primary sites in the head and neck region make up for <10% of documented cases.3,5 To our knowledge, there have only been 14 cases of EMCs arising in the nasal cavity documented in literature thus far. According to a literature review of the few documented cases of sinonasal EMCs, the most common sites of occurrence for these neoplasms are the maxillary sinus and inferior turbinate. 6 As previously mentioned, distant metastasis is rare, occurring in only 5% of documented cases. 2 Despite the relatively low potential for metastasis, patients with distant metastasis have a significantly worse prognosis and thus early diagnosis and treatment are essential in securing favorable outcomes.3,5
The clinical presentation of EMCs is highly variable and dependent upon the primary site and extent of tumor. 2 Due to the rarity of this tumor type, initial imaging generally does not elicit suspicion of EMCs. 2 As is true in the present case and among all previous literature, final diagnosis of EMCs is made after histological examination of a surgical specimen. In regards to EMCs that are localized to the nasal cavity, epistaxis, nasal crusting, and nasal obstruction are symptoms that are consistently reported in the literature.2,5 Less common symptoms include facial swelling, epiphora, hyposmia, headache, and unilateral vision loss. 6 Depending on the aggressiveness of the tumor, symptoms may progressively worsen prior to appropriate treatment. 2 Because of the relatively low rate of metastasis of EMCs (8.1%-25%), prognosis is generally favorable because the malignancy becomes blatantly apparent to the patient before metastasis can occur. 7 Histopathological features of EMCs are well-documented throughout previous literature. EMCs are characteristically composed of a mass primarily consisting of eosinophilic cuboidal epithelial cells that are described as ductal cells. 1 Surrounding the mass of ductal cells is a rim of myoepithelial cells. 1 The mass stains positive for cytokeratin and smooth muscle actin for the two cell types, respectively, and generally conveys low proliferation. 7 In a unique case report by Kamga et al, positron emission tomography (PET) was utilized to image a high-grade EMC of the nasal cavity. It was found that the EMC had atypically high glucose uptake which could be associated with its higher grade. 8 EMCs imaged by PET have generally been shown to have low glucose uptake which may be related to their low-grade status in most cases. 8 However, it should be noted that due to the rarity of sinonasal EMCs, it cannot be assumed as of yet that PET imaging is a particularly useful tool for predicating prognosis. The present case has a notable contrast from the classic presentation of a low-grade tumor; this EMC was determined to be an intermediate grade through histopathological examination due to moderate nuclear atypia. There have been a select few cases in previous literature reporting EMCs of high-grade histology; however, it is important to emphasize that these specific malignancies are the exception rather than the rule in regard to EMCs.
EMCs are incredibly rare, thus there is no formal consensus regarding treatment. Because of the low invasiveness of this tumor type as well as its tendency to infiltrate locally, wide surgical excision is always the main treatment approach.1,2,5,7 In cases where the mass has either not been fully resected or there is significant concern for recurrence, adjuvant radiotherapy is utilized.1,7 To our knowledge, this was the first EMC case in which proton therapy was utilized for treatment. Pencil beam proton therapy was chosen for this case specifically because of the positive margin’s close proximity to the skull base. The efficacy of chemotherapy has yet to be adequately studied as a potential treatment for EMCs, and as such, it is not a recommended neoadjuvant or adjuvant component of a treatment strategy. 7 In the rare case that an EMC metastasizes to distant tissues, chemotherapy may become a more favorable option, as was the case reported by Park et al.
Footnotes
Authors’ Note
The patient presented gave written permission for use of their medical images and information.
The article has not yet been presented at a meeting but was submitted to ARS for September 2023.
Data Availability Statement
Data availability is not applicable. The article is a case report and there is no data/research per se.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
There was no research involving humans that would necessitate IRB or other ethics board review.
Informed Consent
The patient has provided written consent regarding the use of their clinical information and images for medical publication.