
Abstract
Secondary syphilis rarely affects the head and neck including the oropharynx and cervical lymph nodes. These patients present with throat pain, cystic/necrotic lymphadenopathy, and mucosal swelling. Sometimes this constellation of symptoms can be mistaken for head and neck cancer. We report a case of an enlarging throat and painless cystic neck mass in a transgender woman in her forties who was initially suspected to have oropharyngeal squamous cell carcinoma. A subsequent workup revealed the presence of spirochetes without cellular atypia consistent with secondary syphilis. We include the ultrasonography images as well as an endoscopic photograph of the oropharyngeal manifestation in this report.
Case presentation
A 45 year-old male-to-female transgender patient with unknown medical history presented to the emergency department with progressive throat pain and right-sided neck swelling that had been ongoing for one month. Initial symptoms included intermittent blood-streaked mucus, worsening congestion, throat tightness, and right-sided ear fullness and neck swelling. The patient denied experiencing dysphagia, hoarseness, fevers, chills, shortness of breath, or vision changes. Interestingly, she did notice a pruritic, painless rash on her trunk that had progressed to her back and extremities two weeks prior to her visit. Her social history included 30 years of heavy cigarette use, intravenous and inhaled methamphetamine use, homelessness, recent incarceration, high-risk sexual activity with multiple male partners, and limited access to healthcare.
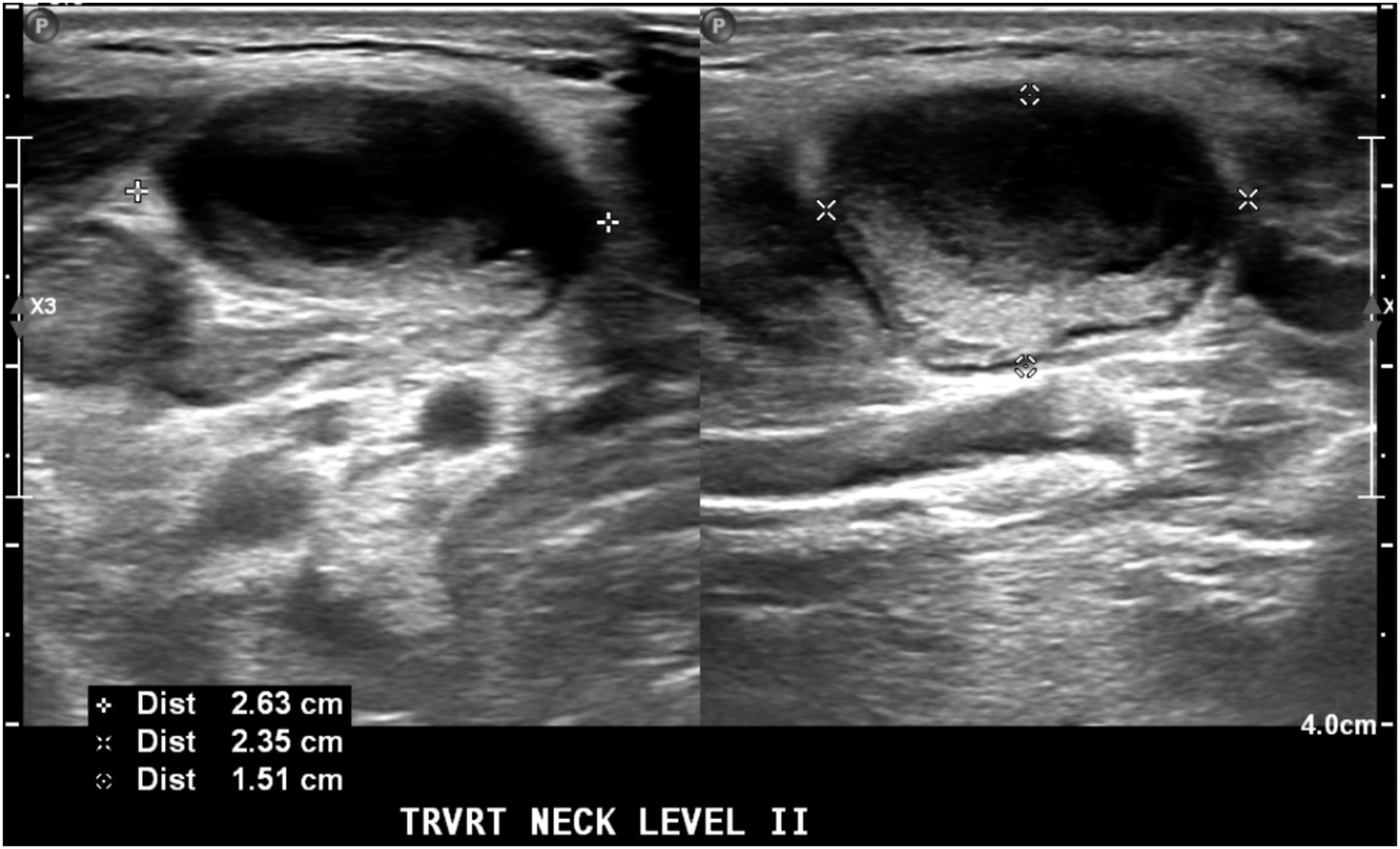
The findings from her physical exam included remarkable pharyngeal erythema and fullness in the right oropharynx and an erythematous maculopapular rash seen diffusely over her chest, abdomen, mid and lower back, and penile shaft. The neck exam showed right-sided level 2 and level 3 neck masses without overlying skin changes. Her white blood cell count was normal at 7.01 x 109/L. A computed tomography scan of the neck showed enhancement and thickening of the soft palate and uvula, fullness of the right nasopharynx and oropharynx, and a heterogeneously enhancing right level 2 lymph node measuring 1.9 cm x 2.8 cm, with internal necrotic changes. Furthermore, the scan showed an enlarged right level 3 lymph node measuring 1.9 x 0.9 cm (Figure 1(A)). The flexible laryngoscopy revealed right-sided nasopharyngeal effacement with a prominent mass extending from the right glossopharyngeal sulcus that was smooth, pale, and without erosion or ulceration (Figure 1(B)). A bedside tissue biopsy of the right oropharyngeal mass was performed and histologically examined with hematoxylin & eosin and immunoperoxidase stains, revealing reactive tonsillar tissue with prominent lymphoplasmacytic inflammatory infiltrate and numerous spirochetes (Figure 1(C)). An ultrasound showed enlarged right level 2 and 3 lymph nodes with necrotic/cystic changes suggestive of nodal metastases of head and neck cancer (Figure 2). However, the tissue exam from the ultrasound-guided FNA revealed reactive follicular hyperplasia with clusters of spirochetes Treponema pallidum. A rapid plasma reagin test was reactive (≥1:1024 titer), and a Treponema pallidium Particle Agglutination test was reactive. Epstein Barr Virus DNA (<500) and hepatitis C antibody were detected. The patient was negative for HIV and Mycobacterium tuberculosis (tested via Quantiferon-Gold). From the FNA and serology, the patient was diagnosed with secondary syphilis. She was subsequently treated with intramuscular penicillin G benzathine. The patient was followed up after one year without any evidence of oropharyngeal or neck fullness. (A), Computed tomography with contrast showing the right oropharynx fullness (white arrow) and an enlarged right-sided cervical lymph node (black arrowhead). (B), Prominent mass extending from the right oropharynx seen on flexible laryngoscopy (black arrowhead) with normal appearing epiglottis (white arrow). (C), Immunoperoxidase stain of the right oropharyngeal mass showing numerous spirochetes (black arrow-head). Ultrasonography of of the right level 2 and 3 lymph nodes with cystic and necrotic changes.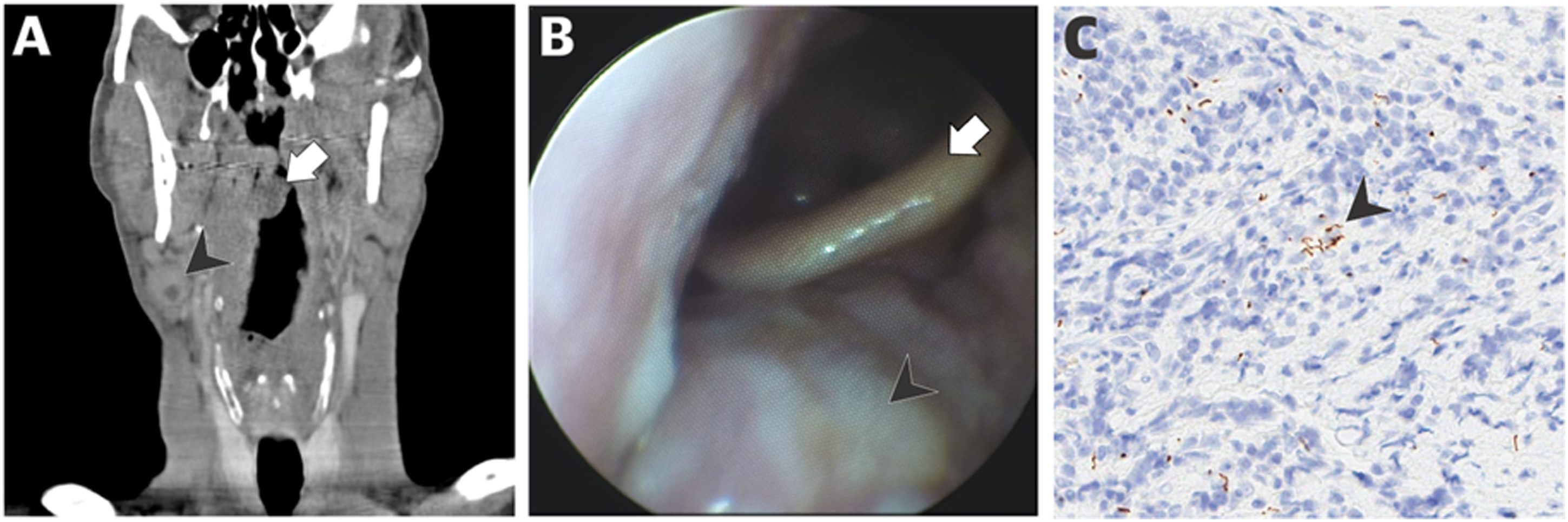
Discussion
Syphilis is a multisystem infection caused by Treponema pallidum that has re-emerged as a public health concern because of its recent resurgence in incidence. 1 A 71% increase in cases of syphilis was observed between 2014 and 2018 particularly among men who have sex with men.2-4 Historically, syphilis has been known as “the great imitator” because it can present non-specifically and mimic numerous clinical diagnoses. Although they are rare, syphilitic oral and oropharyngeal lesions and cervical lymphadenopathy have been mistaken for head and neck cancer, lymphoma, and other neoplastic conditions. 4 This confusion is due to the similar constellation of symptoms patients experience including weight loss, throat pain, and neck swelling.
The salient feature of this interesting case was the appearance of cystic lymphadenopathy on ultrasound. Necrotic, cystic-appearing lymph nodes on imaging often raise concerns for malignancy because regional metastases of p16+ oropharyngeal squamous cell carcinomas can also exhibit cystic and necrotic core of the lymph nodes. However, this case illustrates that infectious or inflammatory conditions other than syphilis such as systemic lupus erythematosus and Kikuchi-Fujimoto disease, may present with cystic lymphadenopathy.5,6 Suspicious-appearing lymph nodes warrant further workup with FNA, which has excellent sensitivity and specificity for detecting malignancy.5,7 However, when there is adequate suspicion for infectious etiology, serologic laboratory testing and antibiotic therapy should precede tissue sampling. 8
While the correct diagnosis of syphilis was initially established in the case described above because of positive biopsy and FNA results, these tools may not universally yield the correct diagnosis for syphilitic neck masses. In a case series of oropharyngeal syphilis presented by Jategaonkar et al., three of five biopsies performed on oropharyngeal syphilitic masses did not reveal spirochetes and instead show non-specific inflammation. 9 One reason for the inability to detect syphilis adequately via biopsy and FNA may be sampling errors from necrotic and inflammatory cores; thus, the use of FNA must be considered along with history and serology. 10 In the case of a syphilitic mass, FNA with darkfield microscopy can be used in conjunction with immunofluorescence staining with treponemal antibodies and conventional silver stain. 11 The traditional method of syphilis diagnosis utilizes anti-treponemal serologic studies such as the fluorescent treponemal antibody absorption test. 12 These serologic tests are not commonly part of the diagnostic pathway for malignancy, and thus require a considerable degree of clinical suspicion to initiate workup. In these cases, a thorough social history is key to identifying patients at increased risk of syphilis infection.
Approximately 8% to 40% of infected individuals who do not receive treatment will develop serious tertiary disease including cardiovascular syphilis, neurosyphilis, and gummatous syphilis.13,14 First-line treatment of syphilis is with parenteral penicillin G or doxycycline for patients with severe penicillin allergy. 15 Additionally, syphilis predisposes patients to a higher risk for HIV transmission and acquisition due to genital inflammation; therefore, all patients with a new syphilis diagnosis should also be screened for HIV and other related sexually transmitted diseases.14,16 Given the many head and neck presentations of syphilis, otolaryngologists have a unique opportunity to recognize these symptoms and intervene before the development of serious sequelae.
Conclusion
Syphilis is a multisystem infection caused by a Treponema pallidum infection. In the head and neck, its manifestation can mimic the presentation of head and neck cancer. Here, we present the endoscopic photography of secondary syphilis and cystic/necrotic lymphadenopathy on ultrasound. The lesion was smooth and somewhat pale without signs of ulceration or friability. A thorough history and physical and a review of systems, such as high-risk social history and recent dermatologic signs, can often provide clues to the correct diagnosis of syphilis. Given the increasing incidence of syphilis, physicians should consider secondary syphilis in differential diagnosis of a middle-aged adult presenting with mucosal lesions and a neck mass.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.