
Abstract
Keywords
Introduction
Tenosynovial giant cell tumor (TGCT) is a benign lesion that can affect any synovial joints. It is particularly common in large weight-bearing joints.1,2 TGCT extremely rarely occurs in the temporal bone [originating from the temporomandibular joint (TMJ)]. It is even less common than malignancies such as sarcomas or metastases. 3
Surgical resection is the key treatment for TGCT of the temporal bone at present. However, temporal TGCTs are often large and have invaded the middle skull base, and the location of the lesions is adjacent to important structures, and thus postoperative complications are sometimes unavoidable. Reported complications after surgical resection are hearing loss, tinnitus, facial paralysis, limited jaw movement, and cerebrospinal fluid (CSF) leak.3,4 Reports on postoperative recurrence rates are inconsistent. One study reports an overall TGCT recurrence rate of 7% to 32.3% after surgical excision. 5 It is therefore a challenging task to protect the important surrounding structures and perform functional reconstruction while completely resecting tumors.
In this study, we selected 5 cases of complex TGCT of temporal bone and middle skull base, and we analyzed and summarized the surgical techniques for tumor resection, functional protection of important structures, and defect reconstruction during the operation of TGCT on the basis of complete tumor resection.
Patients and Methods
Five pathologically confirmed cases of complex TGCT of temporal bone and middle skull base were treated at Eye & ENT Hospital of Fudan University from December 2020 to February 2023. According to the novel grading system for temporal TGCT proposed by Lin et al, 6 we used complex TGCT to define the tumors of grade III/IV for their character of develop extensively and invade beyond the temporal bone. All the patients’ data about clinical symptoms, imaging examinations, surgical methods, intraoperative findings, and follow-up results were collected and retrospectively analyzed. All subjects gave their informed consent for inclusion before they participated in the study. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation (Eye & ENT Hospital of Fudan University) and with the Helsinki Declaration of 1975, as revised in 2008.
For a 3-dimensional display of the range of TGCT and to guide the operation, the computed tomography (CT) and magnetic resonance imaging (MRI) images were reconstructed using 3D Slicer (version 4.11.20210226) (https://www.slicer.org/). 7 CT bone window sequences and MRI enhancement sequences were used for the reconstruction. The extension used was SlicerElastix (http://elastix.isi.uu.nl/). The detailed information about these operations can be found in the manufacturer’s instructions.
Results
Patient Characteristics and Clinical Symptoms
In this study, 5 patients were diagnosed with TGCT. The patients’ characteristics and clinical manifestations are presented in Table 1. Common clinical symptoms include hearing loss (4/5), tinnitus (4/5), and preauricular pain (3/5). Only 1 patient had facial paralysis before the operation, and no patient had obvious restricted mouth opening. The average age at diagnosis was 37 years (30-53 years). No significant gender and side differences were found. The average duration time from symptom onset to diagnosis was 9.2 months (1-36 months).
Characteristics and Clinical Symptoms of Patients.
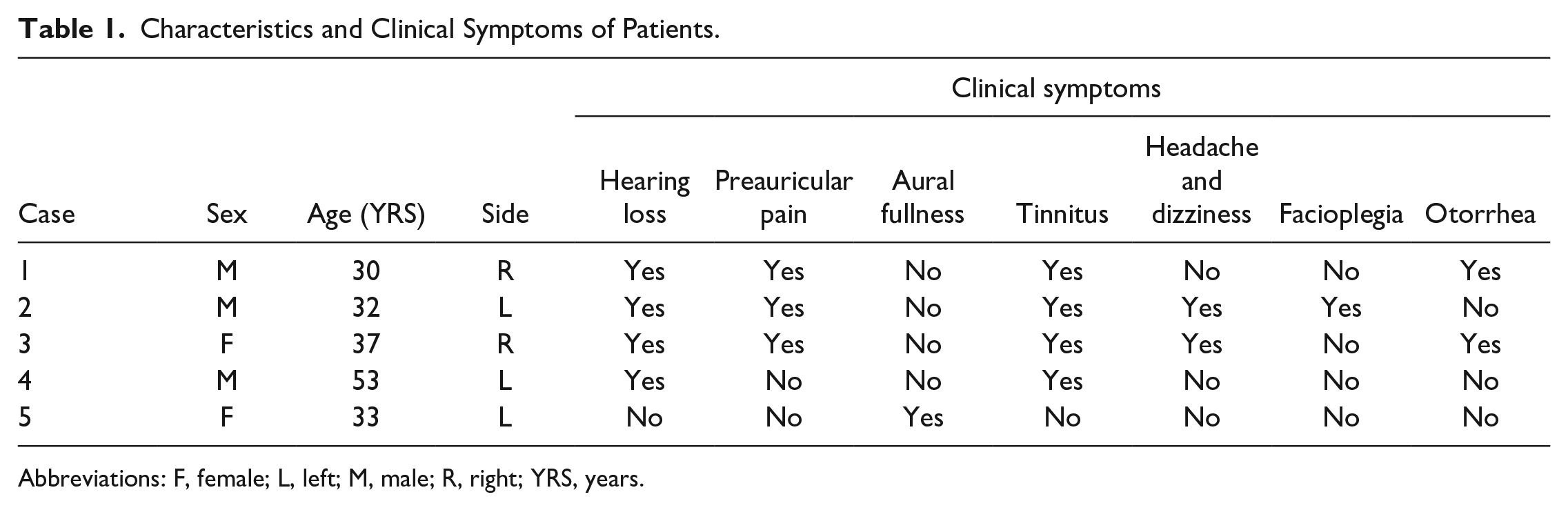
Abbreviations: F, female; L, left; M, male; R, right; YRS, years.
MRI and CT Features
CT imaging revealed no specific manifestation. Poorly defined soft tissue masses with irregular bone destruction of the squamous part of the temporal bone, middle skull base, TMJ, zygoma, and external and middle ears were found in all our patients, and CT imaging demonstrated expansive growth (Figure 1A).
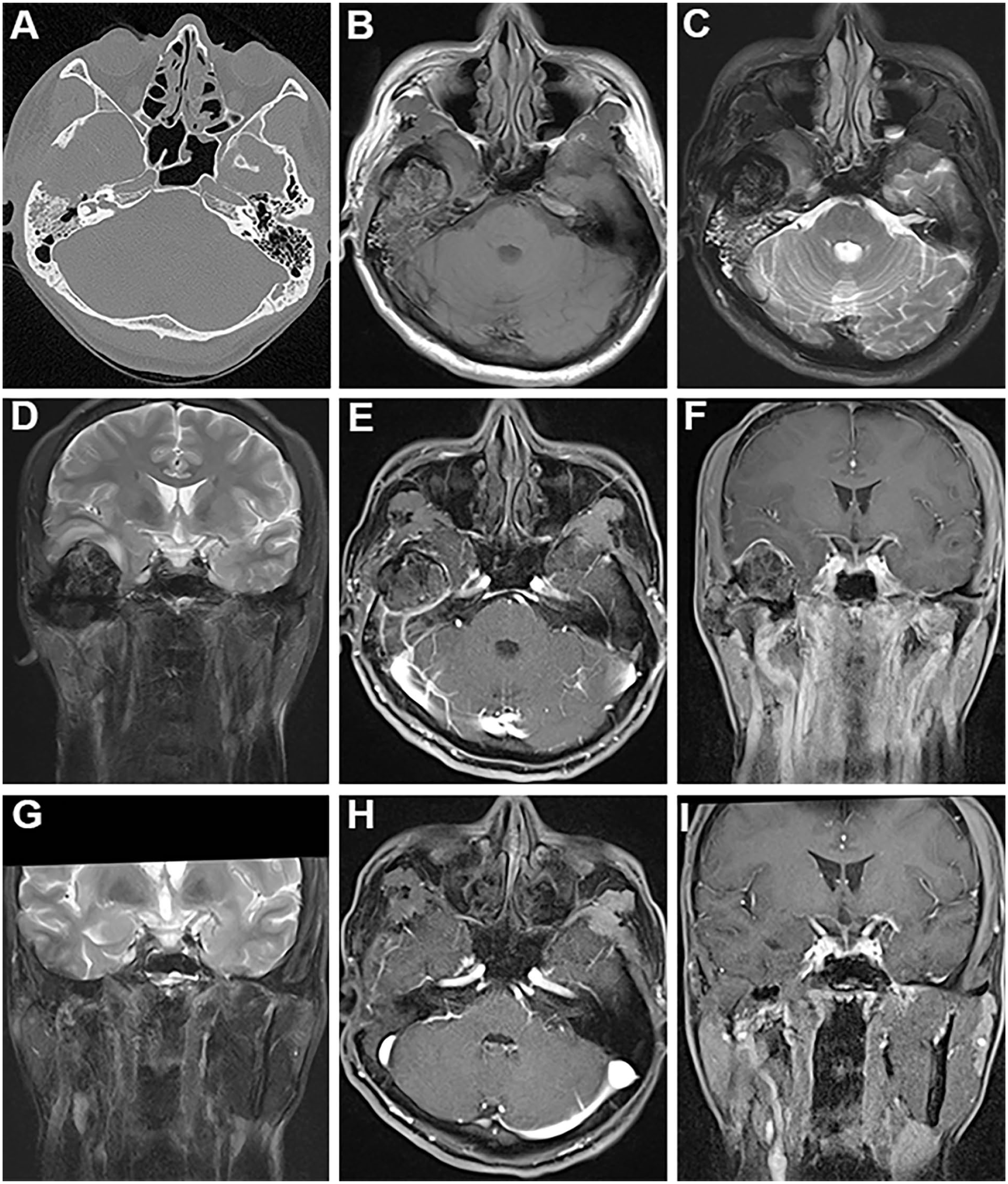
CT and MRI of case 1. (A) CT images. Soft tissue mass was seen in the middle skull base, with unclear boundaries involving the right temporal lobe, squamous and petrous parts of the temporal bone. (B) The mass was isohypointense on T1 of MRI. (C, D) was hypointense on T2, and (E, F) had heterogeneous enhancement. The mass protruded into the middle cranial fossa upward, compressing the bottom of the right temporal lobe, and causing local edema. (G) The coronal T2 of MRI scanned at 18 months after operation. The temporal lobe morphology returned to normal, edema disappeared. (H, I) The enhancement scan after operation. The temporalis muscle flap was found in the operation cavity, and no tumor recurrence was found. CT, computed tomography; MRI, magnetic resonance imaging.
The T1 signals of the tumors were equal or low compared with those of cerebral white matter on MRI (Figure 1B), and the T2 signals were equal, low, or even very low (Figure 1C and D). The signals presented obvious heterogeneous enhancement by gadolinium (Figure 1E and F). The boundary of the tumors was also poorly defined on MRI.
For a 3-dimensional display of the range of TGCT lesions and to guide the operation, we reconstructed the CT and MRI images. We can observe the tumors and important surrounding structures, such as the middle cranial fossa, TMJ, facial nerve, tympanum, labyrinth, internal carotid artery, and sigmoid sinus (Figures 2 and 3).
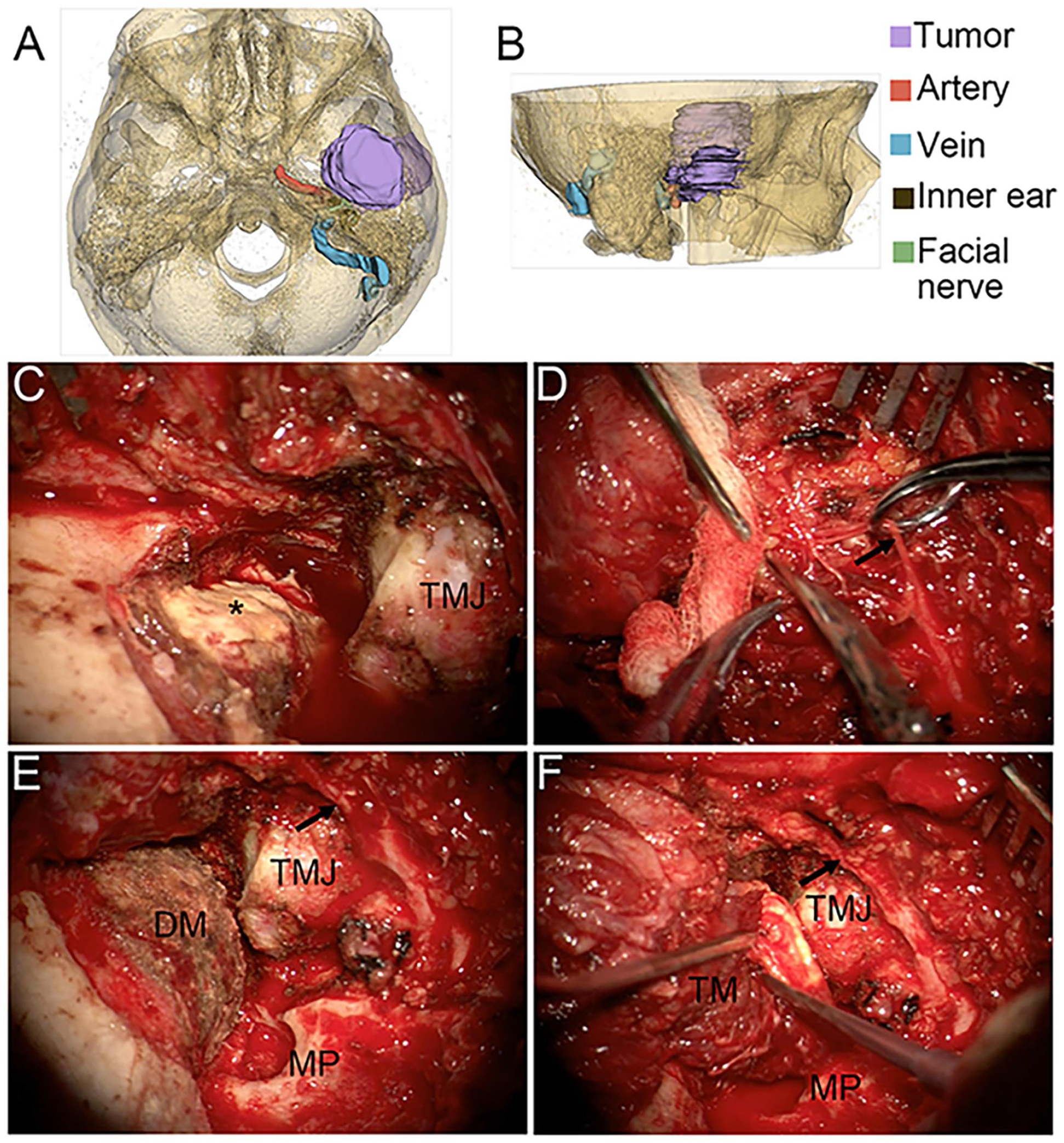
Three-dimensional display of the mass in case 1 and the intraoperative images. (A, B) Three-dimensional reconstruction of a temporal bone lesion. (C) The tumor on the surface of the dura mater of the temporal lobe (asterisk). (D) The separated temporal branch of facial nerve (black arrow). (E) The tumor was resected. (F) Skull base repair. DM, dura mater; TMJ, temporomandibular joint; MP, mastoid process; TM, temporalis muscle flap.
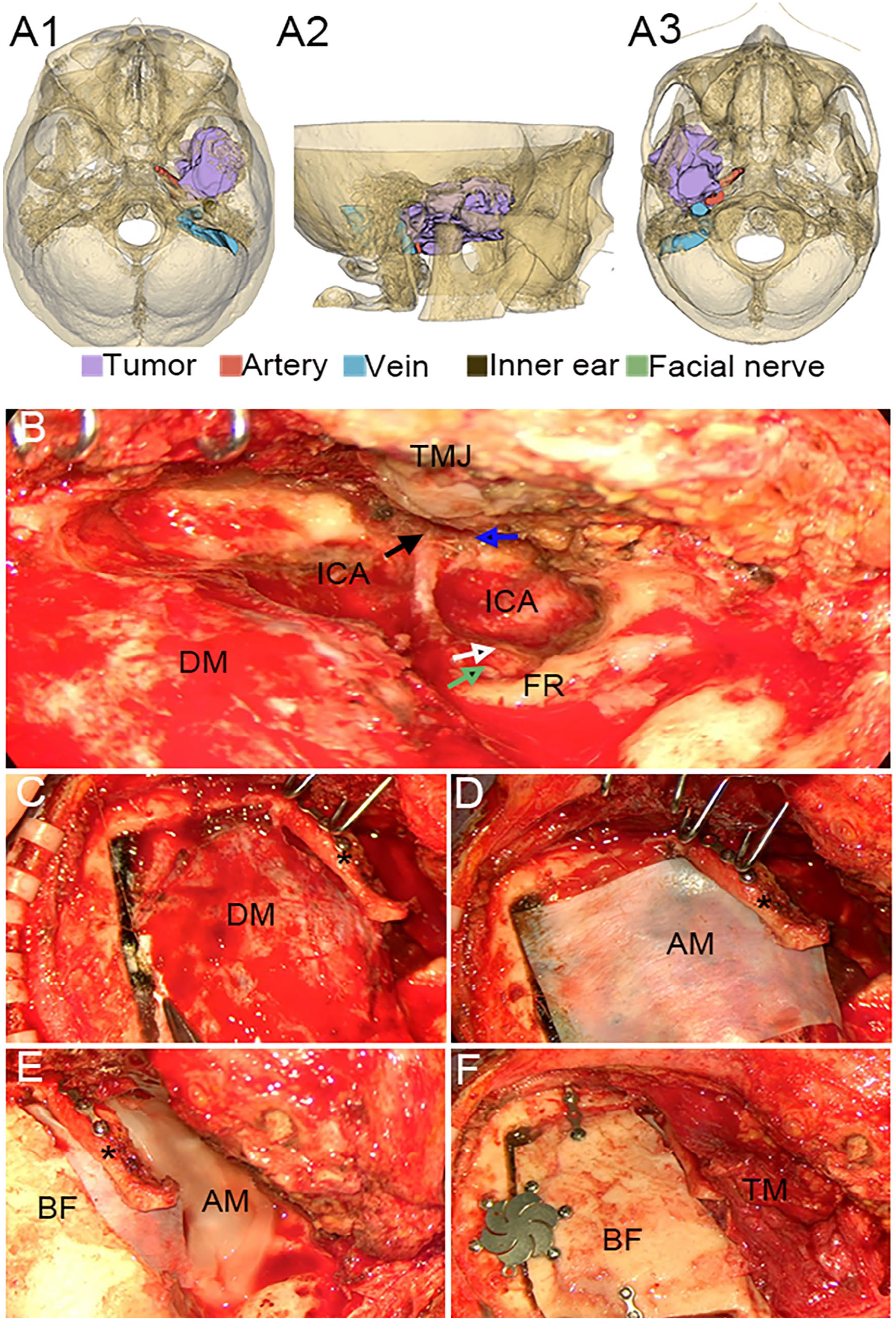
Three-dimensional display of the mass in case 3 and the intraoperative images. (A) Three-dimensional display of the mass. A1, axial view; A2, side view; and A3, antapical view. (B) The black arrow points to the tensor tympani, the blue to the sutured eustachian tube, the green to the stapes, and the white to the cochlea. (C-F) Postoperative reconstruction. The zygomatic arch was fixed (asterisk), the bone flap was reset and fixed. DM, dura mater; TMJ, temporomandibular joint; ICA, internal carotid artery; TM, temporalis muscle flap; FR, facial ridge; AM, artificial meninges; BF, bone flap.
Important Structures Involved in TGCT
The dura mater of the temporal lobe was exposed in all cases, and the temporal lobe was compressed to varying degrees. According to the degree of compression on the axial MRI, 3 levels were defined. Compared to the uninvolved side, the level is classified as severe if the local compressed temporal lobe is greater than 50%, medium if 10% to 50%, and mild if less than 10%. There were 2 patients with severe temporal lobe compression (2/5), 2 cases were medium (2/5), and 1 case was mild (1/5). None of these patients had neurologic symptoms associated with temporal lobe compression.
The facial nerve was also involved in all tumor cases. The commonly involved parts of the facial nerve in the temporal bone were the geniculate ganglion (5/5), tympanic segment (3/5), and labyrinthine segment (3/5). The temporal branch of the facial nerve was also involved in 1 of 5 patients. Although there was a very high probability of facial nerve invasion by tumor, in our study, there was only 1 case of preoperative facial paralysis.
The external auditory canal and tympanum were involved in all cases. Moreover, the auditory ossicles were invaded in 80% of the cases (4/5), mainly the malleus and incus. The labyrinthine bone wall was damaged in case 5, but the membranous labyrinth was intact, and the patient did not experience dizziness.
The internal carotid artery in the petrous part of the temporal bone was surrounded by the tumor in case 3. The tumor even grew backward to the jugular bulb. The trigeminal nerve, middle meningeal artery, infratemporal fossa, pterygopalatine fossa, and parapharyngeal space were also involved (Figures 3).
Treatments and Follow-Up
We mainly performed operations via modified infratemporal fossa approach B or C. The facial nerve was not displaced, and the external auditory canal was not routinely closed. In case 3, the tumor mass was large, so we also applied the expanded middle cranial fossa approach. We completely removed the tumors of all cases and repaired the temporal bone and skull base destruction using the temporalis muscle flap (Figures 1 and 2). We also protected important neurovascular structures surrounding the tumor, preserved the condyles of TMJ and the normal maxillofacial morphology in all cases.
The upper end of the tumors was wrapped by dura mater in cases 1 and 3, with unclear boundaries (Figures 1–3). We slowly and carefully removed the tumors. We then carefully separated the tumors that adhered to the dura mater. For tumors that were difficult to separate, we also utilized bipolar electrocoagulation (Figure 2). Although the facial nerve was involved in all cases, it was completely preserved during the operation (Figure 2). The internal carotid artery was invaded in case 3, we carefully removed the tumor under microscope and endoscope, and the artery remained intact (Figure 3). We also used artificial meninges and bone flap to reconstruct the middle skull base, the temporarily displaced zygomatic arch was reset and fixed with titanium plate (Figure 3). We preserved and reconstructed the external auditory canal with the temporalis muscle flap in case 4, performed tympanoplasty, and selected autologous incus for ossicular chain reconstruction. The postoperative air conductive hearing was the same as preoperative level (Figure 4). Although the skull base was damaged greatly and the temporal lobe compression was medium in case 5, we also preserved the air conductive hearing of the patient by performing tympanoplasty with ossicular chain reconstruction, just like case 4.
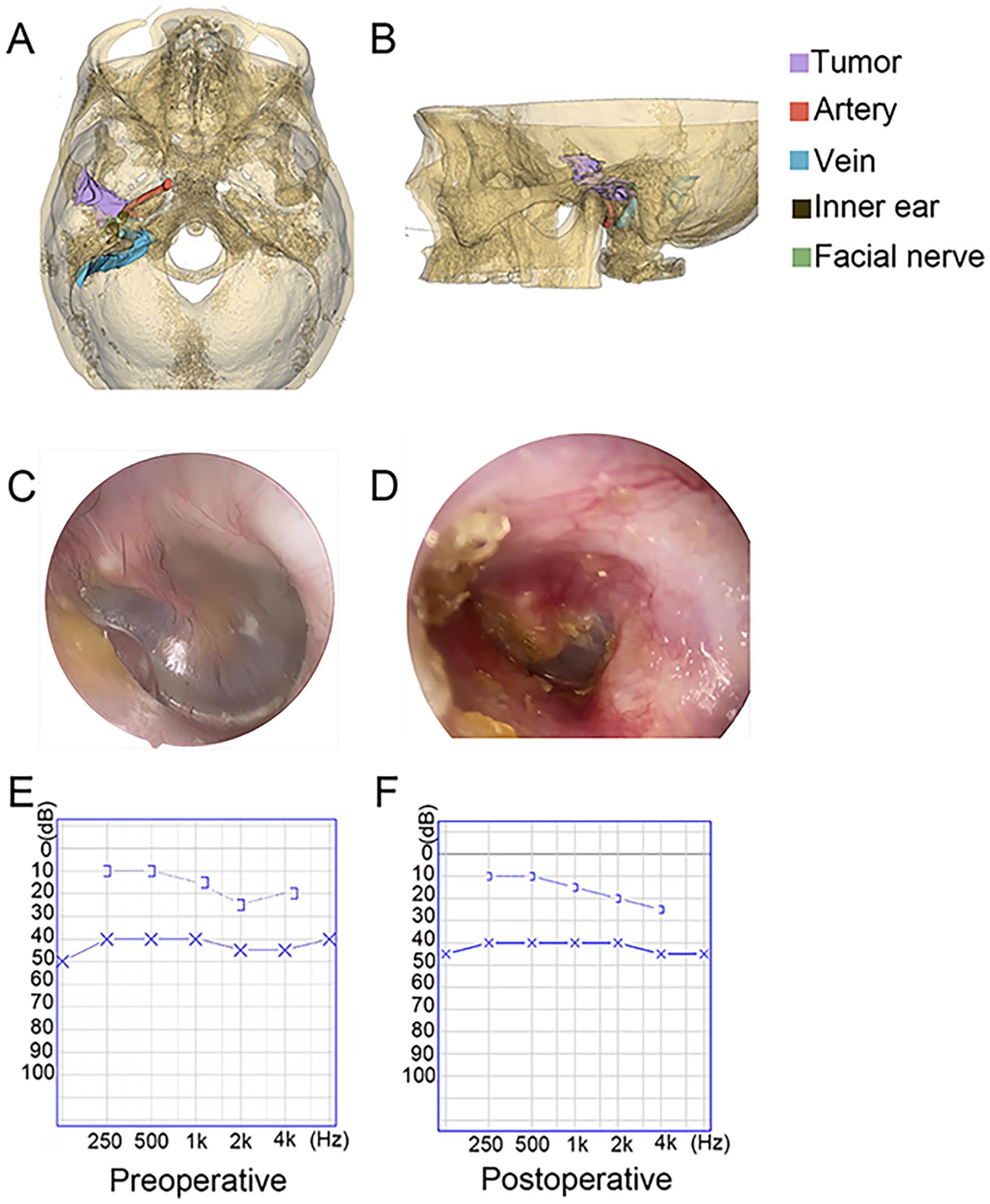
Comparison of preoperative and postoperative data of case 4. (A, B) Three-dimensional reconstruction of a temporal bone lesion. (C, D) The external auditory canal before and after operation. (E, F) Hearing test.
The recurrence rate and recurrence time of temporal bone TGCT are poorly elucidated previously.6,8 We conducted regular follow-up through postoperative CT and MRI scans. The average follow-up time was 20.4 months (12-30 months). No recurrence was found. Except for 3 patients with external auditory canal closure who experienced postoperative air conduction hearing loss, there were no other serious postoperative complications.
Discussion
The etiology of TGCT is unclear. Several genetic and chromosomal alterations have been identified in TGCT.3,9-11 Other possible etiologies involve repeated trauma, lipid metabolism disorders, and hemorrhage. 12 Microscopically, pathology results reveal that the lesion is rich in mononuclear cells, irregularly interspersed multinucleated giant cells, and lipid- or hemosiderin-laden macrophages.13-16
TGCT rarely occurs in the TMJ. Patients initially present with an indolent course of a painless preauricular swelling that may become symptomatic with preauricular pain, reduced mouth opening, trismus, opening deflection, aural fullness, and even hearing loss as tumor size increases.3,4 The main symptoms of our patients were hearing loss, tinnitus, and preauricular pain. TGCT can be misdiagnosed as a parotid neoplasm, ear disease, or other temporomandibular tumors or infections because of its nonspecific clinical symptoms.12,17
The characteristics of the disease on CT and MRI are of great significance for precise diagnoses, such as soft tissue mass surrounding the joint, widening of joint space, bone destruction, and low signals on T1- and T2-weighted images.3,4 The imaging characteristics of our patients were consistent with those reported. The formation of such double low signals could be explained by the formation of hemosiderin, which is characteristic of TGCT.14,15
Surgical resection is the key treatment for TGCT at present. The surgical approach for the disease should be individualized depending on the lesion’s location, age, severity of symptoms, extent of disease, and progression.3,5 Because the location of the lesion is adjacent to important structures, postoperative complications are sometimes unavoidable. Mastering the techniques and strategies to protect these important structures and reconstruct the defects after tumor resection is essential in reducing postoperative complications and maintaining normal maxillofacial morphology.
Temporal Meninges and Brain Tissue
Because the tumor mainly damages the squamous part of the temporal bone, temporal lobe compression is very common and is very severe in some cases. The upper boundary of the tumor is currently not clear. Despite this, we can remove the tumor from the lower part where it is visible. According to this method, we found that as the tumor shrunk, the dura mater and brain tissue gradually bulge out and are not damaged. To handle the tumors on the dura mater surface, we found that careful separation was feasible using a ring knife or micro scissor. For tumors that were difficult to separate, we found that bipolar electrocoagulation was an effective method. Diamond-tip drills can also be used to polish the dura mater surface. No recurrence was found during our follow-up. The integrity of dura mater is very important to prevent postoperative complications and intracranial spread of tumor.
Temporal Bone and Skull Base Reconstruction
There is no consensus on how to repair postoperative defects. Most reported cases with skull base destruction were repaired using an artificial patch, temporal bony flap, titanium mesh, temporalis muscle flap, or autologous fat.15,16 However, there is a dearth of sufficient information concerning the comparison of different repair methods in reconstruction. In our study, we found that in the repair of large defects, the temporalis muscle flap is a reliable option. According to the defect of temporal bone and skull base, the temporal muscle can be divided by scissors or constructed into an appropriate shape. In patients with middle cranial fossa approach, artificial meninges and bone flaps can be used, as in our case 3. In addition, the sternocleidomastoid muscle flaps can be used to fill the mastoid cavity when necessary. Of course, if the local dura mater is found to be damaged during the operation, it is better to fix it using artificial meninges or temporalis fascia plus biological glue and then repair it using the temporalis muscle flap. There was no intracranial infection, CSF leakage, and meningoencephalocele postoperatively in our cases.
TMJ and Zygomatic Arch
Although TGCT of temporal bone originates from TMJ, TMJ should be preserved as much as possible when the tumor is removed. After all, TGCT is a benign tumor. When the condyle affects the exposure of the tumor, we can pull it down temporarily. When necessary, a combination of microscopy and endoscopy can be used to help with lesion resection. Preservation of TMJ is important for the quality of life of patients after surgery. In addition, the zygomatic arch should be kept as much as possible. The displaced zygomatic arch needs to be reset and fixed to maintain the postoperative maxillofacial morphology.
Facial Nerve
When the tumor damages the petrous part of the temporal bone or tympanum, the facial nerve in the temporal bone, especially the genu, is easily invaded. When the tumor grows outside the temporal bone, the temporal and zygomatic branches of the facial nerve are also easily invaded. We found that the facial nerve can be separated from the tumor by careful operation under a facial nerve monitor. In the temporal bone, the separation of the facial nerve needs to start from the normal part, assess the location of the geniculate ganglion and labyrinthine segment accurately, and the separation outside the temporal bone needs to start from the trunk of the facial nerve. In our study, there was no new postoperative facial paralysis, and one case of preoperative paralysis also completely recovered after the operation.
Hearing
When the tumor damages the external auditory canal and tympanum, a complicated problem is encountered: do we need to preserve the patient’s air conductive hearing? There is no consensus on what conditions the patient’s air conductive hearing can be retained. In the case of small lesions, we believe that we should attempt to preserve the hearing, just like in case 4. The damaged upper wall of the external auditory canal can be repaired with a trimmed temporal muscle flap. It is very important to improve the patient’s quality of life after surgery. Air conductive hearing is often sacrificed in lateral skull base surgery with large lesions. Nevertheless, large tumors are not the absolute contraindication of air conductive hearing preservation. However, we need to gather more information to effectively assess patients who are suitable for air conductive hearing preservation.
Internal Carotid Artery
The internal carotid artery may be involved in rare cases. We found that intraoperative vascular ultrasound is an excellent method to help locate the internal carotid artery. For the tumor medial to the internal carotid artery, we removed it with the help of endoscopic visualization. An endoscope provides viewing at various angles, which can help to see some deep anatomical structures. This method helps avoid excessive removal of normal structures and traction of the internal carotid artery during the operation and reduces surgical trauma at the same time. 18
Conclusion
TGCT of the temporal bone is a rare disease that lacks specific symptoms. The lesions are often large and have invaded the middle skull base and surrounding important structures, but the important structures can be separated from the tumor by careful operation. We found and summarized some surgical techniques that can help protect these structures and maintain normal maxillofacial morphology, and the techniques are effective and feasible. Our cases are relatively few, however, and we need to assess more cases and obtain more information during the follow-up.
Footnotes
Acknowledgements
No assistance in the preparation of this article is to be declared.
Authors’ Contributions
XL and YN: Conceptualization, validation, and supervision; HM and YN: Data curation; HM, CT, and HL: Formal analysis and visualization; HM: Investigation and roles/writing—original draft; YN: Funding acquisition, methodology, project administration and resources; HM, CT, HL, and XL: Writing—review and editing.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Natural Science Foundation of China (82271169).