
Abstract
Diffuse-type tenosynovial giant cell tumor (D-TSGCT) is a destructive benign tumor-like proliferative disease that occurs in synovial tissue characterized by villous nodular hyperplasia of joints, tendon sheaths, and synovium. D-TSGCT invading the temporal bone originating from the temporomandibular joint (TMJ) is very rare. Here, we report 3 cases of temporal bone D-TSGCT originating from the TMJ. The tumors in the three cases were originating from the TMJ and further invading the middle ear, the carotid foramen or the temporal lobe respectively. The second patient clearly involved the carotid foramen. The third patient clearly affected the temporal lobe. Lesions were completely removed in 3 cases, and all 3 patients were followed up for 30, 20, and 7 months, and none had recurrence. There are very few reports describing such cases. Although this report is not representative of most scenarios, there is still a potential that it provides a relatively reliable surgical idea for similar cases.
Keywords
Introduction
Diffuse-type tenosynovial giant cell tumor (D-TSGCT) or pigmented villonodular synovitis (PVNS) is a benign lesion that occurs at the joint, tendon sheath, and joint capsule. Patients often present with local pain, swelling, joint stiffness, and limited movement. 1 According to the WHO classification, PVNS is a D-TSGCT. Almost 80% of D-TSGCT cases occur in the knee joints, followed by the hip, ankle, shoulder, and elbow joints. 2 D-TSGCT invading the temporal bone, which originates from the temporomandibular joint (TMJ), is very rare.2-4 In this paper, 3 cases of D-TSGCT in temporal bone were presented. They were all diagnosed in recent three years.
Case Report
Case 1
A 36-year-old woman patient had discharge from the right ear accompanied by hearing loss for one month. She had no ear pain, headache, dizziness, or other discomforts. Twelve days before going to our hospital, a neoplasm was found in the right external auditory canal during physical examination, and she was referred to our hospital for further examination. The temporal bone CT scan in the outpatient clinic showed a lesion of the mastoid process of the right middle ear. The patient had a history of an ectopic pregnancy operation 1 year ago and no other family history or medical history. No smoking or drinking history.
CT scan: Subtle erosions of the right temporal bone and sphenoid bone were observed that affected the anterior wall of the external auditory canal, the tympanum, and part of the mastoid. (Figure 1, A1) Representative CT and MRI images of the 3 cases. Axial CT images of the 3 cases showed soft mass-like density shadow around the TMJ, with bone destruction of the front external ear canal, temporal bone, and the sphenoid bone; MRI images of the 3 cases showed characteristic low signal mass of both T1 and T2 imaging, and no enhancement after contrast-enhanced agent injection. The red star indicates the tumor.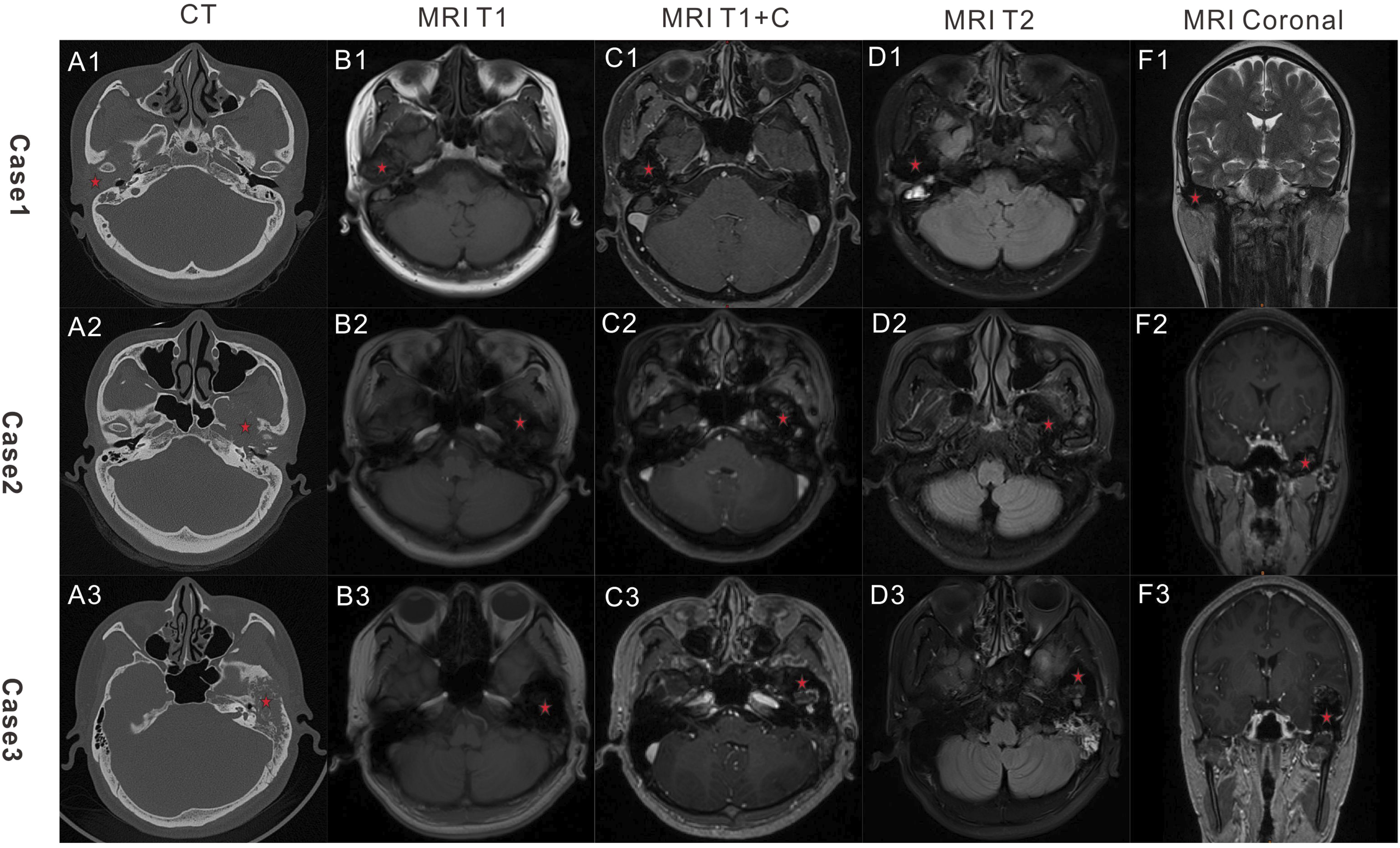
MRI: Low signal mass (3.2×2.9×2.0 cm) around the right TMJ was observed both in T1-weighted images and T2-weighted images; no enhancement was seen after contrast agent injection. (Figure 1, B1-F1)
The right preauricular longitudinal incision was performed. We performed a complete resection of the tumor in the external ear canal, middle ear, and around the TMJ together with the synovium of the TMJ. Pathological examination showed diffuse-type tenosynovial giant cell tumor.
Case 2
A 40-year-old woman was found to have a lesion in the left temporal bone for half a month, accompanied by dizziness without other symptoms. Magnetic resonance imaging (MRI) and computerized tomography (CT) examination showed a temporal bone tumor-like lesion. Then she was admitted to the hospital with a temporal bone lesion. There was no relevant medical history or family history and the patient was otherwise in good health. No smoking or drinking history.
CT scan: Extensive bone destruction was observed in the left petrosal bone, tympanic bone, greater and lesser wing of the sphenoid bone, with the involvement of the left otosteon, and carotid foramen. Soft mass lesions were found around the TMJ, in the external ear canal and middle ear (Figure 1, A2)
MRI scan: Bone destructions were observed in the left temporal bone, the TMJ, and the wing of the sphinoid bone. The bone destruction area was characterized by a low signal of T1 and T2 images (4.0×3.5×2 cm) with uneven enhancement after injection of contrast agent. (Figure 1,B2-F2)
A C-shaped incision was made that stretched backward behind the ear. We give a complete resection of the tumor in the right external ear canal and the TMJ area together with the affected synovium. Pathological examination showed diffuse-type giant cell tumor of the tendon sheath (pigmented villonodular synovitis) with focal chondrogenesis. Immunohistochemistry showed tumor cells: CD68 (+), CD163 (+), Desmin (individual +), SMA (partially weak +), S100 (-), CD34 (-), DOG1 (-), SATB2 (focal +), H3G34W (-), P53 (-), and Ki67 (LI: 5%). (Figure 2) H&E and IHC images of the tumor from Case 2. A: H&E 200X; B: H&E 400X; C:CD163 200X; D: Desmin 200X. IHC: immunohistochemical.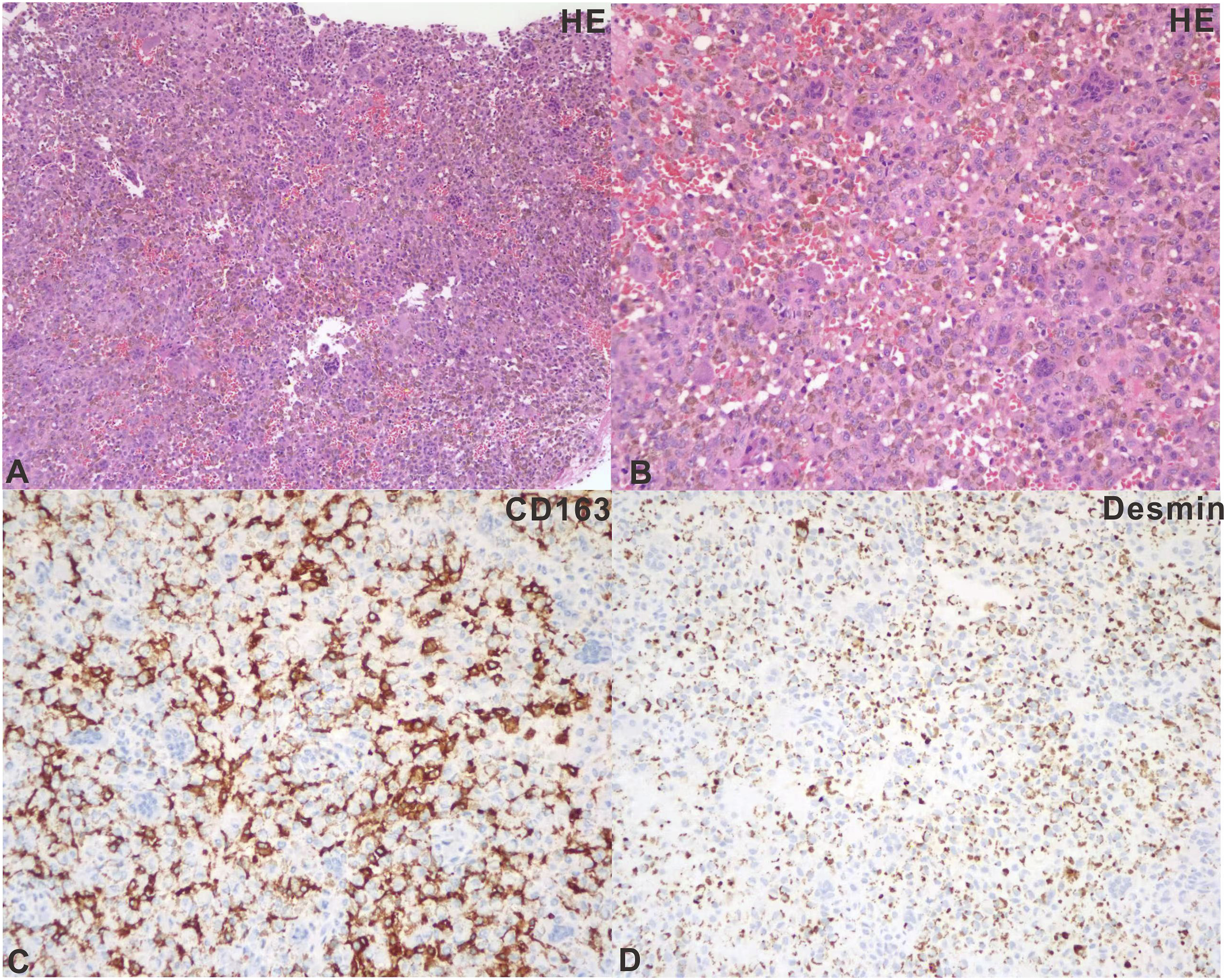
Case 3
A 32-year-old male patient had hearing loss for two months accompanied by tinnitus.
He had no headache, dizziness, nausea, or vomiting. He then underwent a CT and magnetic resonance examination, suggesting the intracranial space occupying lesions. A biopsy suggested choleadiatoma. For further diagnosis and treatment, he came to our hospital. There was no relevant medical history or family history and the patient was otherwise in good health. No smoking or drinking history.
CT scan: Bone absorption and destruction were observed in the left wing of the sphenoid bone, the left temporal bone and the front and back walls of the left external auditory canal, and some bone hyperplasia and sclerosis were involved in the left TMJ. The lesion broke through the left temporal bone and formed a mass in the adjacent temporal lobe parenchyma. The intracranial mass was predominantly cystic solid components, measuring approximate 2.7×4.0×3.0cm, with a small amount of calcified shadow in the solid components. Enhancement was observed in the solid part on contrast-enhanced CT scan. (Figure 1 , A3)
MRI: Bone destruction was seen in the left wing of the sphenoid bone and temporal bone, an obvious low-signal mass of T1 and T2 was seen from convex to intracranial, with a size of about 4.5×4.9×2.8 cm, and no enhancement after injection of contrast agent. Left temporal lobe invasion and edematous shadow of the T2 signal were seen (Figure 1, B3-F3).
We performed the surgery in collaboration with the neurosurgeon. A horseshoe incision was chosen in the left frontotemporal region and behind the ear. The lesion in the mastoid, middle ear canal, external ear canal , TMJ area, and intracranial space around the TMJ were completely resected. Postoperative pathology: Diffuse giant cell tumor of the tendon sheath (pigmented villonodular synovitis) with focal chondrogenesis, tumor invasion of surrounding bone tissue, and immunohistochemical staining showed tumor cells: PCK (-), EMA (-), SMA (focal +), Desmin (-), CD34 (-), S100 (-), P63 (-), CD68 (indicating histocytes and multinucleated cells +), H3G34W (-), H3K36M (-), H3K27M (-), and Ki67 (LI: 5%)
Discussion
Diffuse-type tenosynovial giant cell tumor (D-TSGCT) is a very rare benign neoplasm. An epidemiological study of D-TSGCT in the United States in 1980 estimated that the annual incidence was approximately 1.8 per million patients. 5 According to a multicenter retrospective study in China in 2015, the ratio of male to female patients was 1.36:1, the average age was 36 years, and the average time from the first symptom to diagnosis was 18 months. 1 Overall, 73.84% of the cases occurred in the knee joint, 18.14% in the hip joint, followed by the ankle, wrist, shoulder, elbow, and finger joint. Cases of temporal bone (TMJ) are very rare, with fewer than 100 reported D-TSGCT cases in TMJ. Jason A Brant systematically analyzed 76 reported cases of D-TSGCT in TMJ, 33 of which involved the middle cranial fossa, 32 affected temporal bone, 9 involved the dural membrane, and 15 with lesions of the external auditory canal or tympanic membrane. 2 Tenosynovial giant cell tumor occurring in the TMJ, especially diffuse tenosynovial giant cell tumor, tends to invade surrounding tissues, such as the external auditory canal, middle ear cavity, mastoid process, temporal bone scale, middle cranial fossa dura, and even intracranial invasion. 2 The 3 cases reported herein involved the external auditory meatus, middle ear, temporal bone, and sphenoid bone, and one of them involved the brain tissue of temporal lobe. Therefore, D-TSGCT that occurs in the TMJ seems to be more aggressive than in other joints, and its reasons and specific mechanism need to be further studied.
The etiology of D-TSGCT is unclear. The current general view is that it is caused by chronic synovial inflammation for various reasons. Other possible factors include trauma, bleeding, and lipid metabolism. Myers and Masi reported that approximately 88% of patients with localized TSGCT and 59% of patients with diffuse TSGCT had a history of associated trauma. 5 Some scholars also believe that D-TSGCT is a tumor. 6
D-TSGCT develops slowly and appears as a painless mass in its early stage. As the mass continues to grow, pain and joint movement limitation may occur, leading to joint stiffness and joint destruction. D-TSGCT originating from the TMJ may have different clinical manifestations depending on the extent of its invasion. When the lesions were confined to the joint capsule, the main manifestations were temporomandibular joint disorder and lockjaw. Further expansion of the lesion may result in preauricular or parotid masses, while invasion of the external auditory canal or tympanic cavity of the middle ear is associated with symptoms such as hearing loss and discharge of the ear. Invasion of the intracranial can cause headaches or other cranial nerve compression symptoms. Therefore, patients with TMJ do not necessarily show symptoms associated with TMJ impairment. Patients who visit the ENT clinic usually have symptoms such as hearing loss and other symptoms of the ear, at which point the lesions invade the external auditory canal or the middle ear. None of the 3 cases reported in this paper had obvious symptoms related to TMJ injury. However, when hearing loss occurred or the mass was accidentally found during physical examination, the history of chief complaint was short due to atypical early symptoms. With the help of CT, MRI, and other examinations, we need to consider the possibility of D-TSGCT when bone destruction occurs around the temporal-mandibular joint. We can perform a preoperative puncture or intraoperative frozen fast inspection, when necessary, to provide a basis for our clear diagnosis and selection of appropriate surgical procedures.
D-TSGCT that occurs in the TMJ has a variety of clinical manifestations and is easily confused with diseases in the surrounding tissues of the TMJ. Therefore, we often need to determine the type of disease by imageology. On X-ray, D-TSGCT was presented as a soft tissue mass with periarticular bone erosion. The CT demonstrates an osteolytic lesion typical around the TMJ. Magnetic resonance imaging shows joint effusion, hemochromatosis, synovial dilatation, and bone erosion. The MRI findings are not consistent, subject to the influence by the proportion of fat, hemosiderin, fibrous stroma, pannus, fluid, and cellular components in the mass. The representing images were both T1 and T2 low signal and no enhancement after gadolinium injection. Even so, considering that D-TSGCT and many diseases around the TMJ have similar imaging manifestations, D-TSGCT needs to be differentiated from many other diseases in the TMJ region, such as synovial chondromatosis, 7 chondrosarcoma, 8 giant cell repair granuloma, 9 and giant cell tumor, and most of the time we need to rely on pathological examination to get the final diagnosis.
For any symptomatic D-TSGCT, the preferred treatment is surgery to remove the mass, synovial membrane, and affected bone. Patients with D-TSGCT visiting the ENT clinic often have bone damage of the external auditory canal, middle ear, mastoid, or other parts of the temporal bone, so we need to address these affected areas at the same time. When intracranial invasion occurs, the collaboration between the otorhinolaryngologist and neurosurgeon is needed. The appropriate incision and surgical path are quite important for complete tumor resection, good exposure of the temporomandibular joint, and an esthetic appearance after recovery.
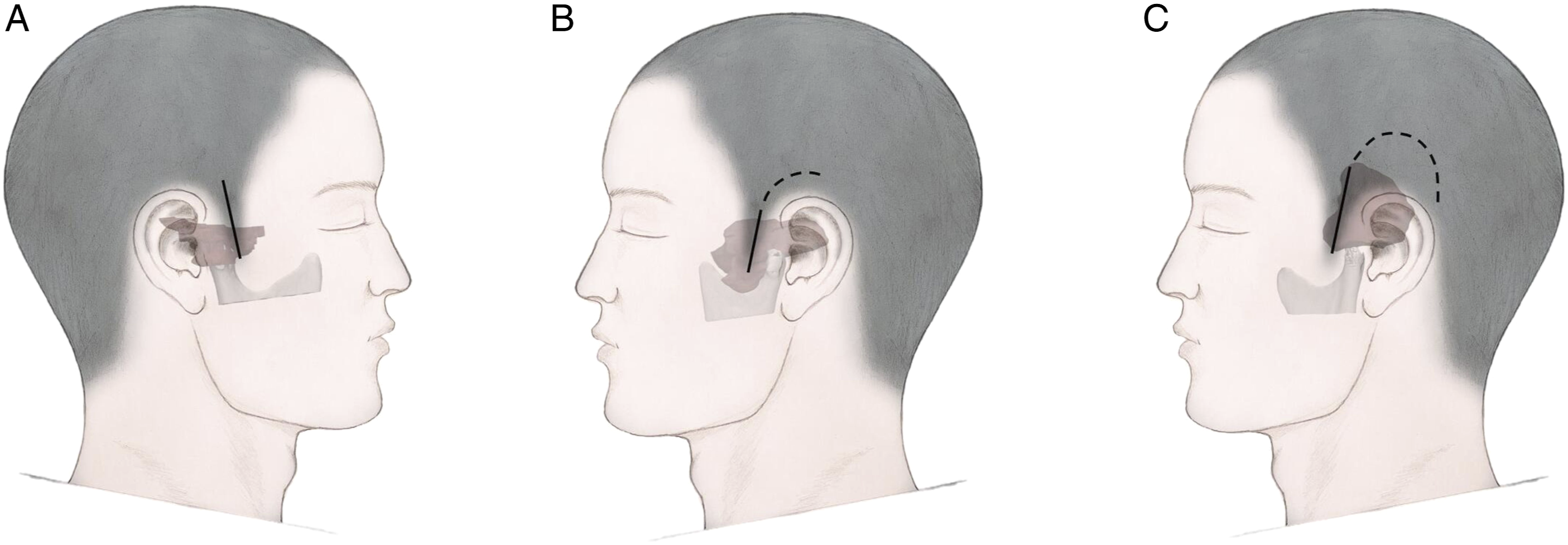
In the 3 patients described in this paper, incisions were made within the hairline to maintain esthetics. Different incisions were selected according to the extent of the lesions involved, but both exposure to TMJ and complete resection of the lesion were considered. Typically, an anterior longitudinal incision was performed, extending upward or backward, depending on the extent of invasion of the skull or the middle ear accordingly. The first patient had obvious involvement of the parotid gland and a longitudinal incision was made within the temple hairline in front of the right ear (Figure 3(C) and (D)), which was conducive to complete removal of the lesions in the parotid gland. The second patient involved the middle ear and the mastoid process. A C-shaped incision was selected that extends backward behind the ear to ensure simultaneous resection of the lesions of the mastoid process, skull base, and temporomandibular joint (Figure 4(A))). The third patient was obviously involved in the temporal lobe, so a horseshoe incision was selected in the left frontotemporal region and behind the ear (Figure 4(B)) to facilitate the complete removal of intracranial lesions. The horizontal segment of the carotid artery on the deep surface of the surgical cavity should be carefully protected during surgery. It is beneficial to maintain the integrity of the temporomandibular joint capsule at the base of complete removal of the tumor. In the meantime, it was necessary to preserve the integrity of the external auditory canal skin and tympanic membrane as much as possible during surgery, which could help prevent the occurrence of postoperative external auditory canal stenosis by combining with external auditory canal tamponade. Finally, the temporal muscle flap was utilized to fill the surgical cavity. (Figure 4(C)) The complete removal of the lesions greatly reduced the risk of recurrence. In this study, 3 patients were followed for 3 years, 2 years, and 1 year, respectively, without recurrence. Surgery images of Case 2. A: Exposure of the tumor. B: The surgery cavity after excision of the tumor. C: Preparation of the temporal muscle flap. D: Using the temporal muscle flap to fill the surgery cavity. Schematic diagram of the incision. A: Patient 1. B: Patient 2. C: Patient 3. The full line indicates the basic incision and dotted line indicates the extended incision depending on the extent of the tumor.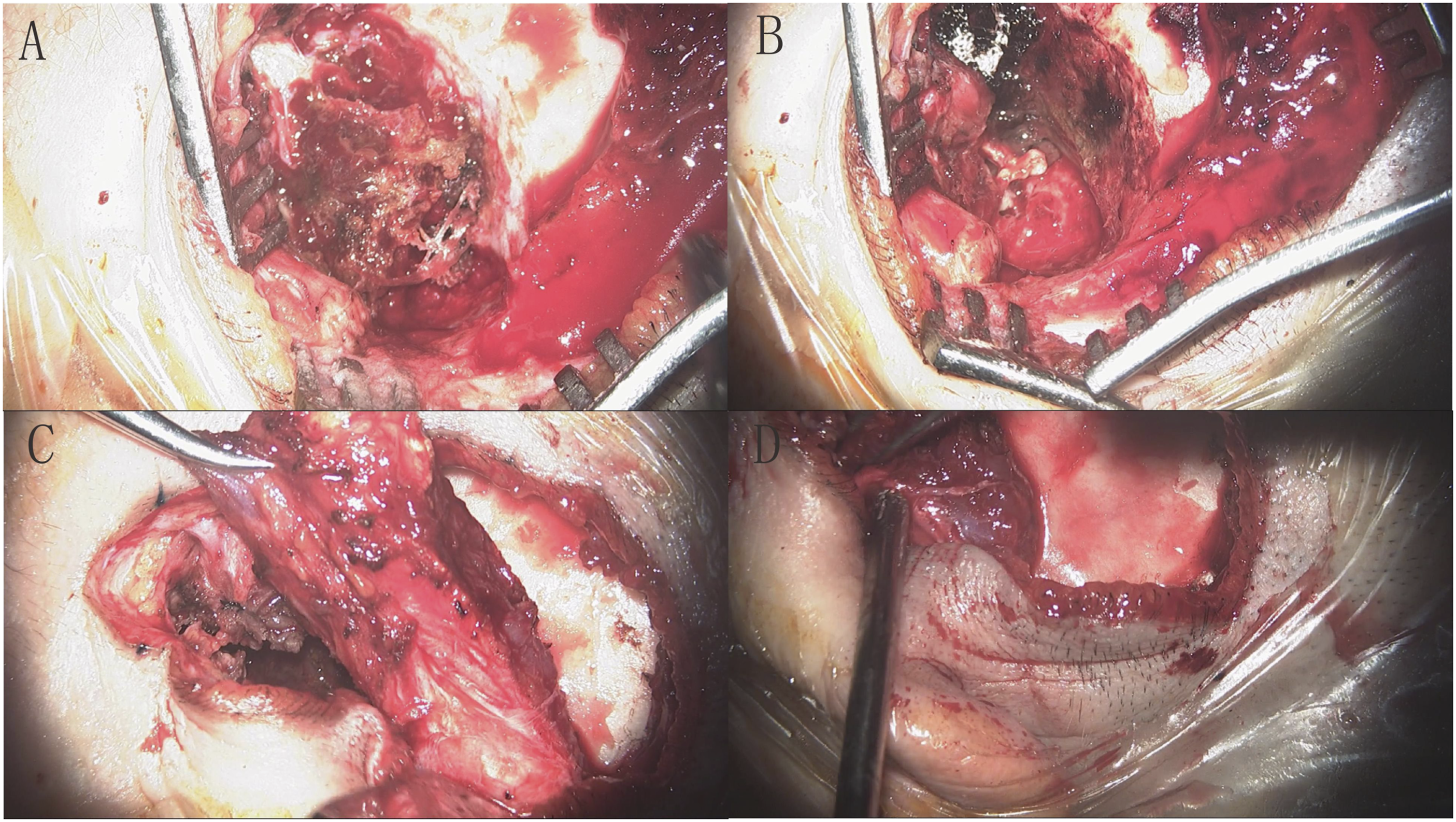
Radiation therapy is recommended for patients who have relapsed or tumors that cannot be completely resected.10,11 The reported recurrence rate of D-TSGCT in TMJ is approximately 9%. Other therapies, including emactuzumab and PLX3397, which target the CSF1/CSF1R pathway, have also shown some effectiveness. 12
In conclusion, MRI plays a critical role in the preoperative diagnosis of this disease, showing a characteristic low signal on the T1- and T2-weighted images, and no enhancement after gadolinium injection. An anterior longitudinal incision, extending upward or backward depending on the extent of the tumor, is sufficient for both radical excision of the tumor and maintenance of good appearance. Long-term follow-up of patients will help us to understand more about the nature of this disease, as well as studies focusing on the pathogenesis of this disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.