
Abstract
Tenosynovial giant cell tumor (TSGCT) represents a family of benign tumors that arise from the synovial tissue of a joint, tendon sheath, or bursa. It usually involves the joints of the extremities and rarely occurs in the head and neck region. Here, we describe a case of a 32-year-old man with a submucosal mass bulging in the posterior pharyngeal wall since one month. The lesion was removed and diagnosed with localized type of TSGCT based on histopathological investigations and clinical presentation. It is very rare that TSGCT occurs in the retropharynx, which reminds clinicians to consider this entity as a possible diagnosis.
Introduction
Tenosynovial giant cell tumor (TSGCT) or giant cell tumor of the tendon sheath represents a family of benign tumors that arise from the synovial tissue of a joint, tendon sheath, or bursa. It may present as intra- or extra-articular lesion and is classified by biological behavior as localized or diffuse. 1 The localized type is considered absolutely benign, whereas the diffuse type is more aggressive, and may exceptionally include a malignant component. 1
Tenosynovial giant cell tumor usually involves the joints of the extremities and rarely occurs in the head and neck region. 2 In the head and neck region, it mostly affects the temporomandibular joint (TMJ) in the form of diffusion. 2 -4
Here, we present a case of TSGCT located in the retropharynx in an adult. To our knowledge, this anatomical site is very rare for this tumor. The ethics committee of the West China Hospital of Sichuan University approved this report, and the patient provided informed consent for publication.
Case Report
A 32-year-old man presented to our department with a longer than 1-month history of throat discomfort. Physical examination found that the tongue, tonsils, larynx, and vocal cords were normal, but a submucosal mass that was relatively fixed with respect to the cervical spine bulging in the posterior pharyngeal wall anteriorly from slightly above the level of the soft palate down to the tip of the epiglottis. The patient had no history of fever, pain, facial asymmetry, or trismus. No lymphadenopathy was noted.
Computed tomography (CT) was performed and showed a slight low-density mass with relatively clear boundaries in the left posterior pharyngeal wall extending from the upper pole of the left tonsil to the level of the epiglottis. Posteriorly, the lesion replaced part of the left prevertebral musculature until the cervical spine bone, but no osseous involvement was noted (Figure 1). Based on the CT features and symptoms, our initial diagnosis was lipoma. Therefore, we did not continue with a magnetic resonance imaging (MRI) examination.

Computed tomography revealed a slight low-density mass with relatively clear boundaries in the left posterior pharyngeal wall (yellow arrow).
With tonsillectomy instruments, we performed transoral surgery under general anesthesia to remove the lesion and found that a solid mass of about 3 cm × 1.8 cm × 1.2 cm with relatively clear boundaries was tightly attached to the anterior longitudinal ligament. After complete resection, the surgical specimens were sent for histopathological analysis.
Microscopically, the tumor was relatively well circumscribed and consisted of multiple cell types: sheets of ovoid and spindle-shaped small mononuclear cells, larger plasmacytoid mononuclear cells, and scattered multinucleated giant cells (Figure 2A). Immunohistochemical studies showed that the mononuclear and multinucleated cells were positive for CD68 (Figure 2B) and CD163 (Figure 2C), but negative for desmin, PCK, SMA, β-catenin, CD34, and S100 protein. No atypical mitotic figures or necrosis were identified. In view of the histopathological findings and clinical presentation, the final diagnosis was the localized type of TSGCT. After 2 years of follow-up, no evidence of recurrence was seen.
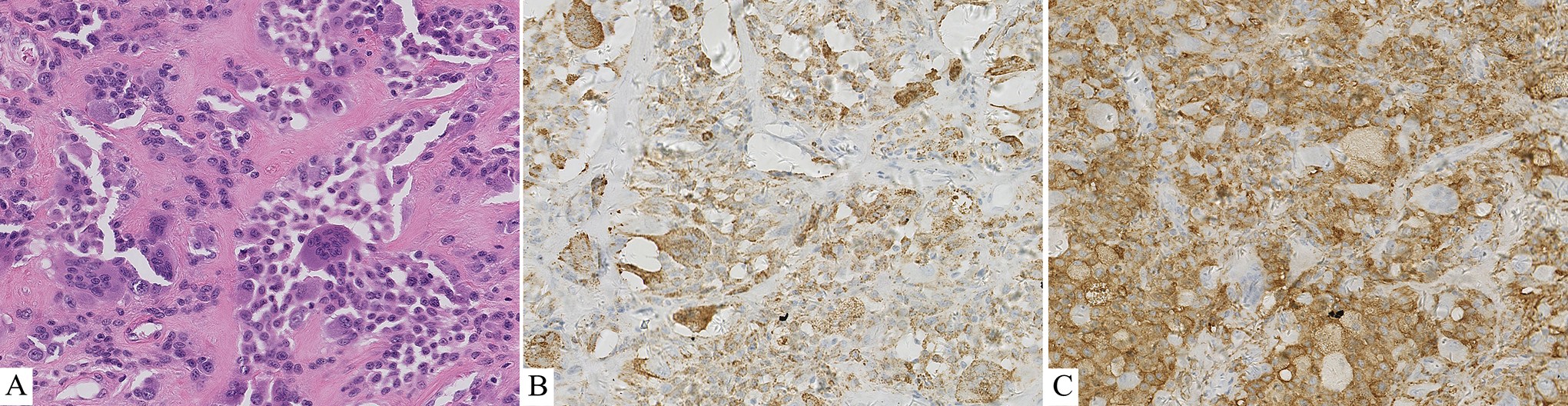
Histopathological findings. (A) Photomicrograph of the lesion showing a large numbers of sheets of ovoid and spindle-shaped mononuclear cells with scattered plasmacytoid mononuclear cells and multinucleated giant cells (H&E, ×200); Immunohistochemical studies showing that the mononuclear and multinucleated cells were positive for CD68 (B) and CD163 (C).
Discussion
Tenosynovial giant cell tumor rarely occurs in the head and neck region, preferentially affecting the TMJ. 3 -5 About 60 cases involving the TMJ have been reported in the English literature. 6 In other parts of this region, including the neck, 7,8 cervical spine, 9 -11 clinoid, 12 and retropharynx, TSGCT appears to be even rarer. Here, we report a case of a TSGCT in the retropharynx to strengthen clinicians’ understanding of this disease.
Tenosynovial giant cell tumor often arises in or near the synovial tissue of a joint, bursa, or tendon sheath, so it usually involves the hand, foot, knee, hip, ankle, and elbow. 1 However, the tissue of origin of a TSGCT in the retropharynx remains unclear. Although many fasciae are located around the retropharyngeal space, such as the buccopharyngeal fascia anteriorly, the carotid sheaths laterally, and the prevertebral fascia posteriorly, the tumor did not seem to arise from these structures. We speculate whether the retropharyngeal TSGCT originated from the anterior longitudinal ligament because the tumor was tightly attached to it; however, this is difficult to confirm.
Although rare in children, TSGCT may occur at any age, mainly in the third to fifth decades, 1 with no significant sex predilection in the head and neck region. 1,6 The clinical presentation of TSGCT is relatively nonspecific. There may be a painless mass with very slowly progressing or joint discomfort accompanied by repeated swelling and restricted range of motion. 1 In the TMJ, hearing loss, otalgia, fullness, and trismus may occur when the tumor involves the middle and inner ears. 3
Radiographical examination is essential and very valuable. X-ray and CT may show bone abnormalities or cystic erosion in or around the joint in diffuse forms, as well as a cyst without calcification, symmetrically on either side of the joint line or at the capsular insertion lines in localized forms. 1,3 The most contributive examination is MRI, in which the localized forms may show a well-delineated mass without aggressive behaviors, and the diffuse forms are usually articular, showing as a soft tissue lesion infiltrating the tendon sheath and adipose tissue around the joint. 1,13,14 All of the lesions have a characteristic weak or intermediate signal on T1- and T2-weighted sequences, which is related to variable tissue hemosiderin loading. 3,14
The diagnosis depends on the histopathological findings. Microscopically, the tumors, which are mainly composed of small mononuclear cells, larger plasmacytoid mononuclear cells, and multinucleated giant cells, tend to be circumscribed or nodular. The larger plasmacytoid mononuclear cells are the true lesion cells that consist of round, eccentrically placed nuclei and eosinophilic cytoplasm. 2,6,15 Immunohistochemically, the mononuclear cells and multinucleated giant cells express CD45, CD68, and CD163. 6 The larger lesion mononuclear cells may also be positive for desmin and clusterin. 16,17 However, none should be positive for S100 protein. 2,6
The main differential diagnosis for TSGCT in the head and neck region is chondroblastoma and giant cell tumor of bone (GCTB). Although the 3 lesions have mononuclear cells and giant cells, most of the mononuclear cells in chondroblastoma are positive for S100 protein, but negative in TSGCT. As for GCTB, it usually arises from the bone or cartilage accompanied by osseous destruction. 18,19 The multinucleated osteoclast-like giant cells of GCTB are larger with abundant nuclei (>20 in many), and the tumor may manifest a broad range of histologic variations, such as fibrosclerotic areas with collagenous stroma, secondary aneurysmal bone cyst with hemosiderin deposition, and osteoid deposition. 2 In the retropharyngeal space, TSGCT should also be distinguished from some malignant tumors (eg, lymphoma, sarcoma) and other benign tumors (eg, lipoma, hemangioma).
Surgical resection remains the current standard therapy. 20 The localized forms can usually be controlled by total resection and show little recurrence (0%-15%). 1 The diffuse forms involve difficult surgical issues, and local control is uncertain. Recurrence rates range between 21% and 50%. 1,20 Radiation therapy is the most widely used adjuvant treatment, although the levels of evidence are low. 1 It is usually performed in diffuse or recurrent forms to reduce recurrence. Recently, medical targeted therapies have obtained extensive attention. The inhibitors of colony-stimulating factor 1 (CSF1)/CSF1 receptor axis have been tested in patients, showing very good therapeutic effects. 20 However, more and larger randomized trials need to be conducted to confirm these results.
In summary, TSGCT occurs rarely in the retropharynx, usually with nonspecific symptomatology and slow progression, which makes it difficult to be identified and considered in the early phase. Our report has summarized its clinical characteristics and histopathological findings, emphasizing the need to consider this entity as a possible diagnosis by clinicians when a retropharyngeal mass is identified.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.