
Abstract
Nodular fasciitis is a relatively uncommon disorder that occurs in soft tissues and results in a rapidly growing mass predominately found in adults. Proliferative fasciitis is a rarer variant of nodular fasciitis that is typically found in adults over age 40 and is extremely rare in pediatric patients. This case report involves a pediatric patient who presented with a large, posterior, rapidly growing mass on the right ear. This was excised and the subsequent biopsy required several pathology consultations and opinions. Multiple immunohistochemical and molecular studies eventually led to the findings of spindle cell mesenchymal neoplasm, consistent with proliferative fasciitis of pediatric type.
Keywords
Introduction
Proliferative fasciitis is a variant of nodular fasciitis that occurs predominately in adults age 40 years and older.1,2 It is a benign pseudosarcomatous myofibroblastic proliferative disorder that occurs in the soft tissues and presents as a rapidly growing lesion. These are not commonly found in the head and neck region.2,3 They can present with or without pain and other symptoms.1,2 While proliferative fasciitis growth is often rapid and may appear uncontrolled, it is typically only found in subcutaneous adipose tissue and does not extend outside of those bounds. 3 Treatment typically involves local excision. 1 This case is atypical in that it presented on the ear of a pediatric patient and is the one of the first cases of its kind in the literature that meets these criteria. A prior case of proliferative fasciitis was reported in the posterior ear of a 3-year-old male. 4
Case Report
A 7-year-old female presented to our facility after her parents noted a mass behind the right ear (Figure 1). This had been enlarging for the past 2 months and the patient complained of intermittent pain. There were no other relevant symptoms.

Intraoperative Examination of Tumor.
The physical examination revealed a 4 cm × 3 cm mass along the posterior pinna. The rapid growth of the lesion was quite concerning and our initial diagnostic impression was for a sarcoma. Immediate excision of the post auricular mass was recommended and discussed with the parents (Figure 2).

Surgical Excision.
The mass was subsequently sent for microscopic examination as 2 parts. The microscopic examination found prominent dermal expansion by a cellular mesenchymal proliferation with ulceration. The lesional population in the mass was principally composed of plumb spindle cells, and occasional regions displaying epithelioid morphology (including focal ganglion-like cells). Mitotic figures were readily identified in the mass, and there was no definitive evidence of necrosis (Figures 3 -5). Immunohistochemical stains for smooth muscle actin, performed on a representative section from each biopsy, were weakly positive in a minority of the targeted population, while those for S100 protein, desmin, CD34, ALK-1, and pankeratin were negative. Additional immunohistochemical stains performed at the Cleveland Clinic showed negativity for desmin, myogenin, MYOD1, ERG, pan-TRK, and ALK (D5F3). They demonstrated intact nuclear expression of INI1, SMARCA2, and SMARCA4. Stains for SOX10 and EMA, performed on a section from tissue submitted as part 2, were also non-reactive. A next generation sequence sarcoma fusion panel was performed at the Cleveland Clinic which failed to detect any gene fusions, including in the FOS gene. The overall findings were consistent with nodular fasciitis; however the presence of an atypical mitosis in conjunction with several hypercellular foci accounted for some unusual features in the mass. Slides from block A1 of this case were sent to Mayo Clinic for chromosomal microarray analysis, which showed a gain of chromosome 2. There was low-level signal for a FOSL1-RELA fusion detected in the submitted specimen. The quality of this finding was uncertain and repeat testing was recommended. The expert opinion of the Mayo Clinic pathologist suggested that the overall findings were consistent with proliferative fasciitis of pediatric type.
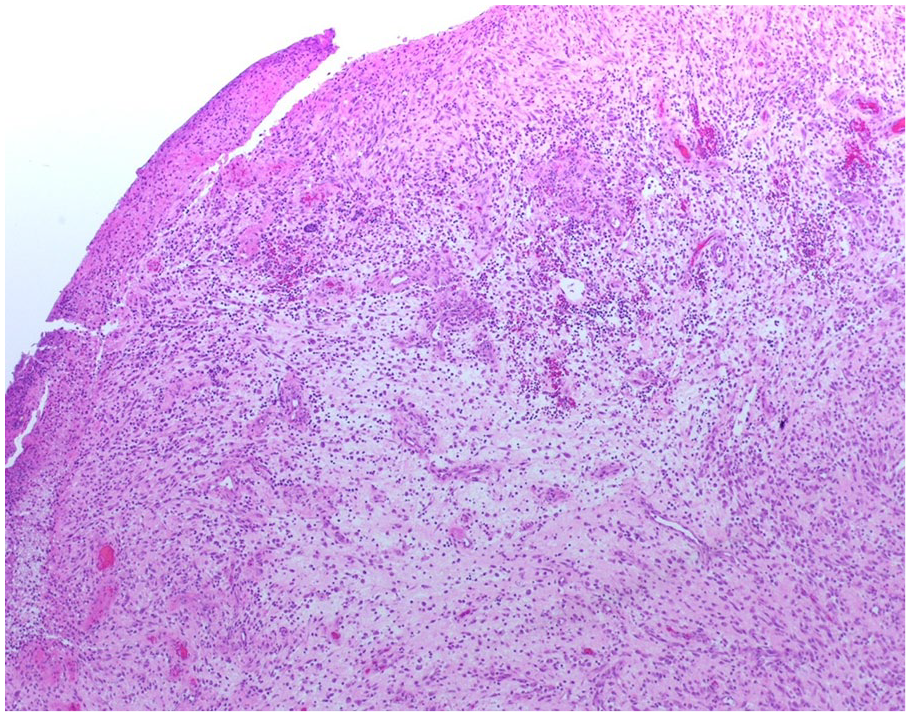
40x Magnification.
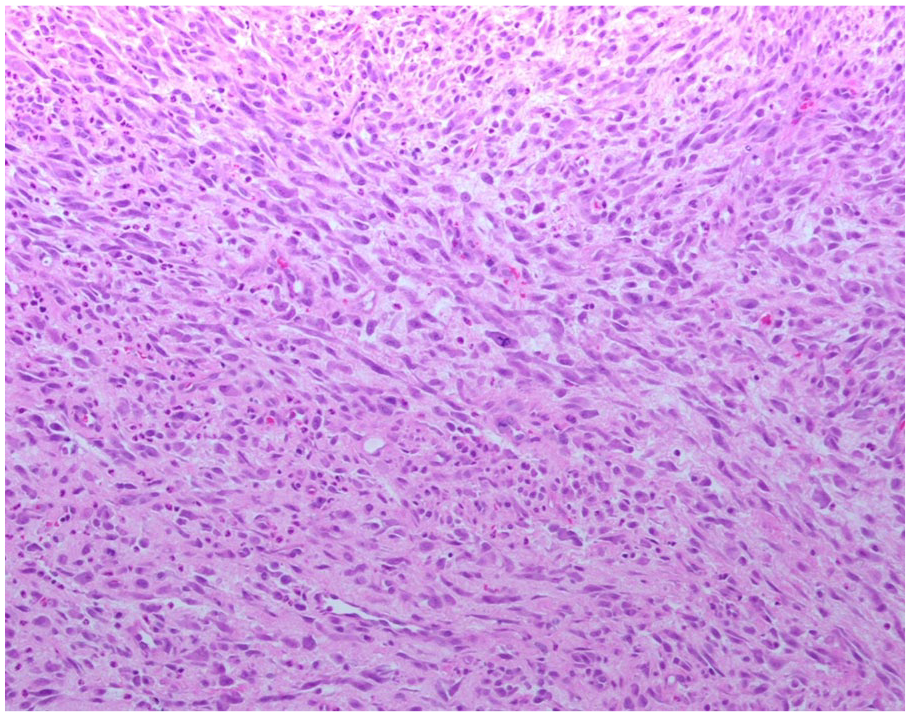
100x Magnification.
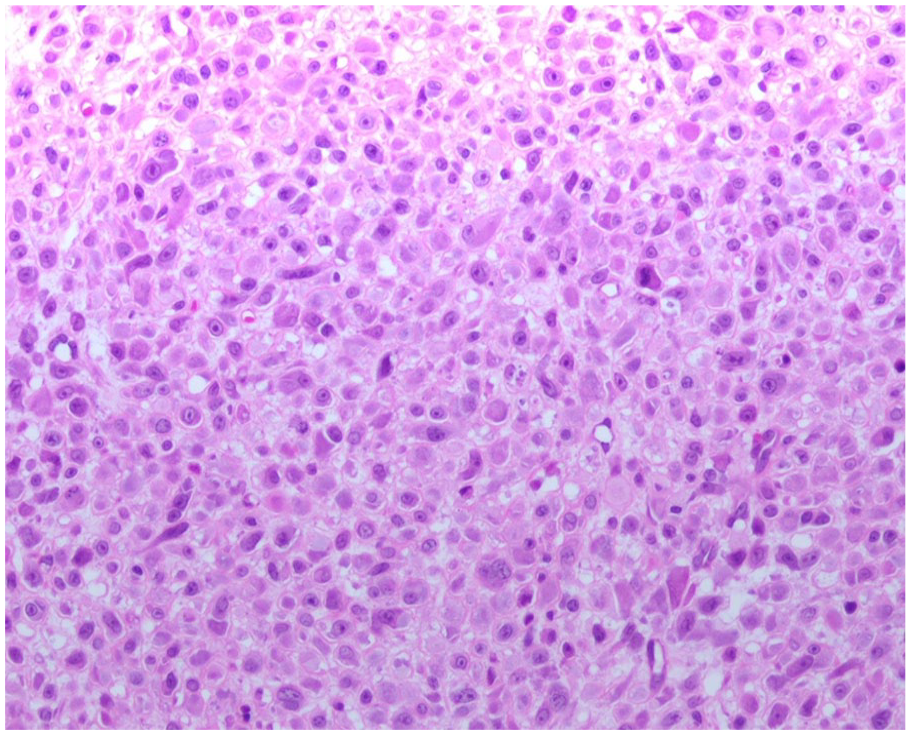
200x Magnification.
Expert consultation at the Cleveland Clinic Department of Pathology interpreted the findings as spindle cell mesenchymal neoplasm, consistent with proliferative fasciitis of pediatric type. Multiple immunohistochemical and molecular studies described above, along with the expert opinion of a Mayo Clinic pathologist, were utilized to arrive at this diagnosis. These lesions have a propensity for local recurrence in this anatomic location, and given the presence of an atypical mitosis and the fact that the tumor appears to reach the black-inked margins, conservative re-excision with negative margins should be considered for cases of this nature.
Discussion
Nodular fasciitis is commonly observed in adults over age 20 but is rarely found in pediatric patients. 5 Proliferative fasciitis is a variant of nodular fasciitis and often misdiagnosed as a soft tissue sarcoma because of its rapid growth and similar histology.3,5 Proliferative fasciitis is rarer than nodular fasciitis with the pediatric form even more rare. There were two cases of nodular fasciitis that were reported in 2023 in the preauricular area in pediatric patients aged 7 and 13. 5 Neither of these cases was classified as proliferative fasciitis. Most cases involving proliferative fasciitis involve subcutaneous adipose tissue in the extremities, with most cases occurring in the forearm. 6
A mutation involving an MYH-USP6 gene fusion has been reported for nodular fasciitis, but no mutations have been linked directly to proliferative fasciitis. 3 A chromosomal microarray analysis for this case was performed at the Mayo Clinic. It showed a gain of chromosome 2 and a low-level signal for a FOSL1-RELA fusion was detected. The quality of this finding was uncertain and repeat testing was recommended.
While local injury has been linked to nodular fasciitis, the same is not true of proliferative fasciitis, leaving the origin unknown.3,7 The events leading to the origin of the mass are not vital to determining the correct diagnosis. Additionally, the imaging features of proliferative fasciitis are not consistently duplicated and pathological findings are often what lead to the correct diagnosis. 3 Histologically speaking, proliferative fasciitis and proliferative myositis are nearly identical, with the mass location being the predominant difference.3,8 Proliferative myositis is found predominately in the trunk and shoulders of the body and forms in the skeletal muscle, while proliferative fasciitis forms in subcutaneous adipose tissue and is predominately found in the upper extremities. 8
The histological appearance of proliferative fasciitis and proliferative myositis includes the presence of ganglion-like myofibroblasts and spindle myofibroblasts as the predominant cell population, with minor differences present between adult and pediatric forms. 3 Cases of pediatric proliferative fasciitis have been found to be less infiltrating and more lobular than the adult forms and present with more cellularity, higher myxoid/collagen ratios, numerous mitoses, and a more solid growth pattern.3,4
Immunohistochemical stains for this case were negative for S100 protein, desmin, CD34, ALK-1, ALK (D5F3), pankeratin, myogenin, MYOD1, ERG, and pan-TRK. This is consistent with what would be expected of proliferative fasciitis. 3 Additionally, there were no mutations found in INI1, SMARCA2, and SMARCA4, which is consistent with proliferative fasciitis. 3 The overall findings were consistent with what would be found in nodular fasciitis, except for the presence of atypical mitosis and hypercellular foci. This led to the diagnosis as spindle cell mesenchymal neoplasm, consistent with proliferative fasciitis of pediatric type.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This is IRB exempt.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.