
Abstract
Nodular fasciitis(NF) is a proliferative disease of fibroblasts and myofibroblasts that generally affects subcutaneous tissue, muscle tissue, and fascia. NF usually occurs in young adults aged 20–40 and is more common in the upper extremities and relatively rare in the region of the head and neck. Here, we report on two patients with NF in the ear and nose. Under general anesthesia, the masses of NF were completely resected along the safety margin. The patients recovered well after surgery and there was no recurrence after more than half a year of follow-up.
Introduction
Nodular fasciitis (NF) is a benign disease that originates in the subcutaneous and superficial fascia. 1 It is characterized by fibrous tumor-like hyperplasia and is easily misdiagnosed as malignant due to its rapid growth. NF occurs most frequently in the extremities, followed by the trunk and head and neck, 2 and less frequently in the ear and nose. This article reflects a case of nasal nodular fasciitis in a pediatric patient and adult external auditory canal and reviews the relevant literatures.
Case Presentation
Case 1
A 3-year-old male patient was admitted to our department. His parents reported that a localized lump was accidentally discovered on the left side of his nose four months before the visit. The mass was painless and then grew fast without paying attention to it. There was no similar disease in his family and no familial history of heredity. The patient did not have other positive signs.
On physical examination, the nasal tip was shifted to the right and deformed, and a circular localized lump was observed in the left nasal alar, with unclear boundaries with surrounding tissues, approximately 1.5 * 1.5 cm in size. Skin was free of redness, swelling, and ulceration, and the mass was firm, without tenderness or fluctuation (Figure 1A). A: Preoperative nasal lesion in the child. B: Postoperative recovery after six months.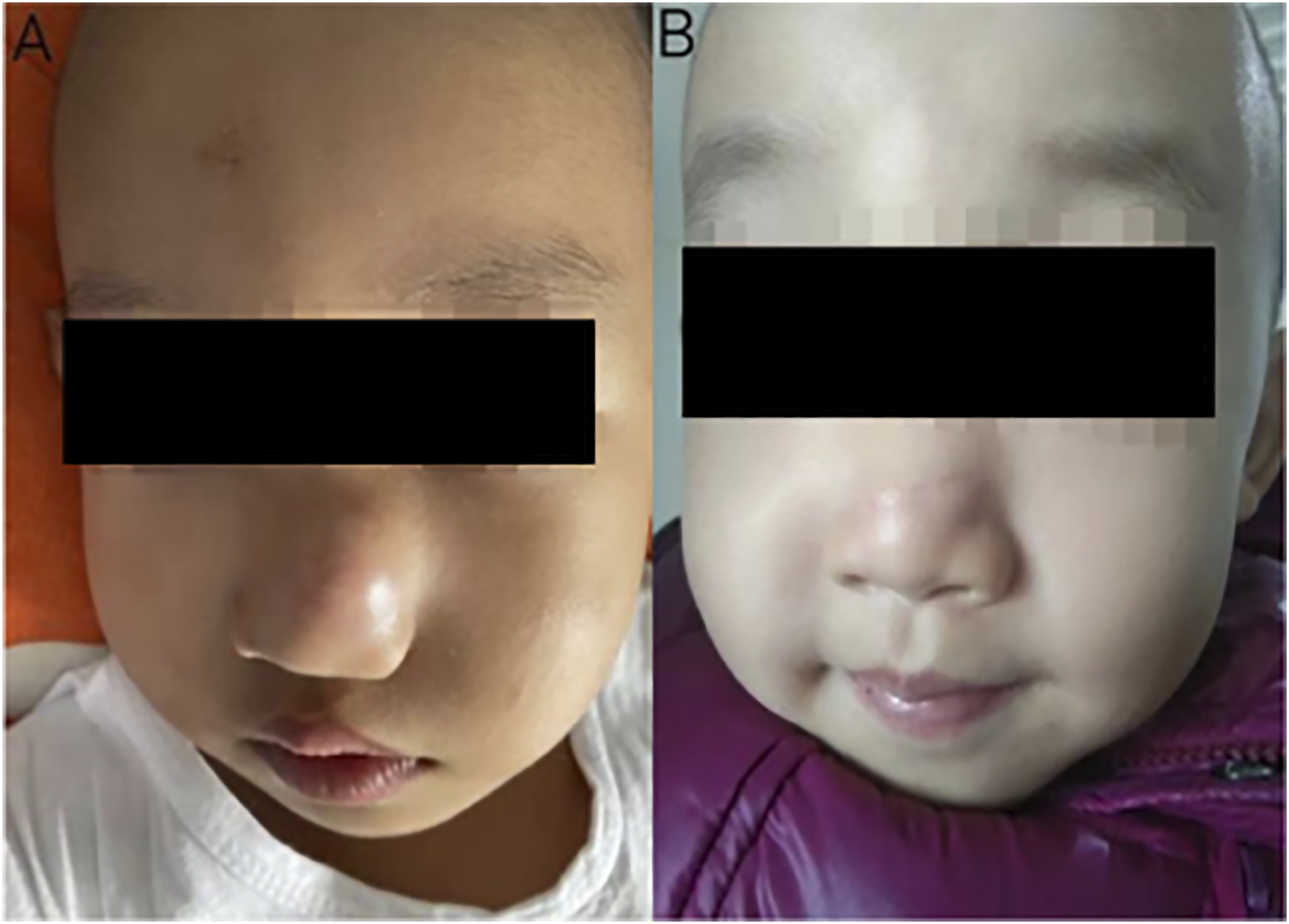
In another hospital, magnetic resonance imaging (MRI) showed a subcutaneous tumor in the left alar, which was considered benign. On ultrasonography (US), a hypoechoic mass was observed at a distance of approximately 0.1 cm from the body surface of the nasal lesion, which had a size of about 1.9 cm×1.0 cm×1.9 cm with well-defined limits and regular contours.
Color Doppler flow imaging(CDFI): Blood flow signals could not be assessed because the child cried.
We operated under general anesthesia and completely resected the tumor along the safety margin. There was no severe adhesion between the tumor and the surrounding tissues. After resection, the tumor was sent for pathological examination and the skin defect was repaired by flap transposition.
The routine pathology showed spindle cells arranged in bundles with extravasation of red blood cells.
Immunohistochemistry(IHC): B1: SMA (+), CD10 (+), CD68 (+), Desmin (-), Ki-67 (3-5%, +), S-100 (minor +), and CD34 (vascular + ).
The Ubiquitin-specific protease 6 (USP6) gene was positive in the genetic test (Figure 2F). During the 8-month follow-up, the nasal shape of the child and the lesion on the nasal alar recovered well and there was no recurrence of the tumor (Figure 1B). A: Hematoxylin and eosin stain(HE stain). B: CD68. C: CD10. D: ki67. E: sma. F: Fluorescence in situ hybridization(FISH) of USP6 gene.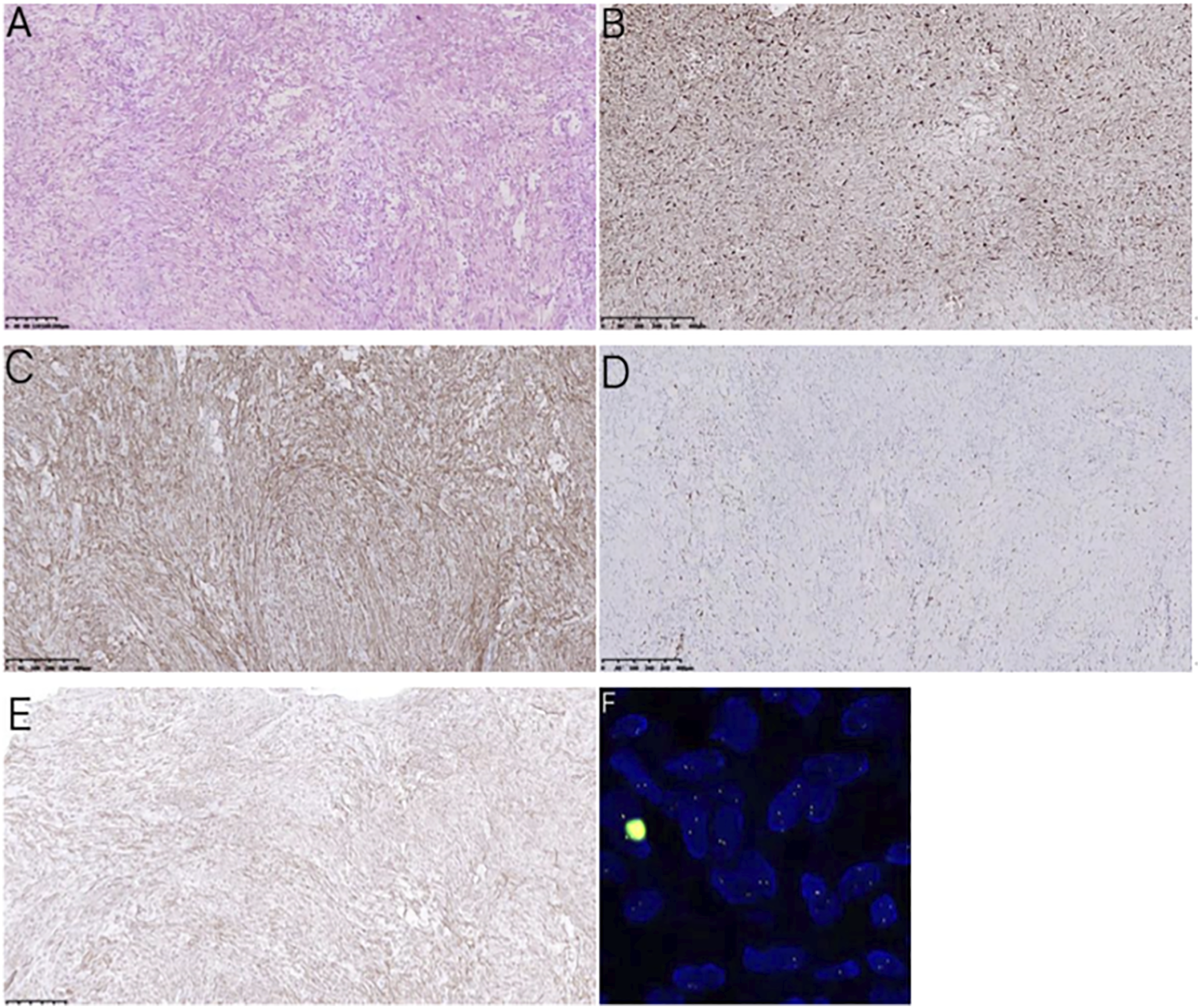
Case 2
A 47-year-old male patient was admitted to our department. He reported that a new organism was accidentally discovered in the right external auditory canal during the ear picking half a month before the visit. The new organism was initially the size of a millet and then rapidly increased to the size of a soybean. Four days before the visit, a thin yellow discharge appeared in the right ear canal without odor or blood. The patient had hearing loss and there were no other positive signs. Physical examination showed that the anterior wall of the cartilage of the right external auditory canal had a bean-shaped neoplasm that blocked the external auditory canal. The surface of the neoplasm was smooth and firm, it was not easy to bleed, and the depth was unclear. On the contrary, the left ear is normal (Figure 3). A: The right ear. B: The left ear.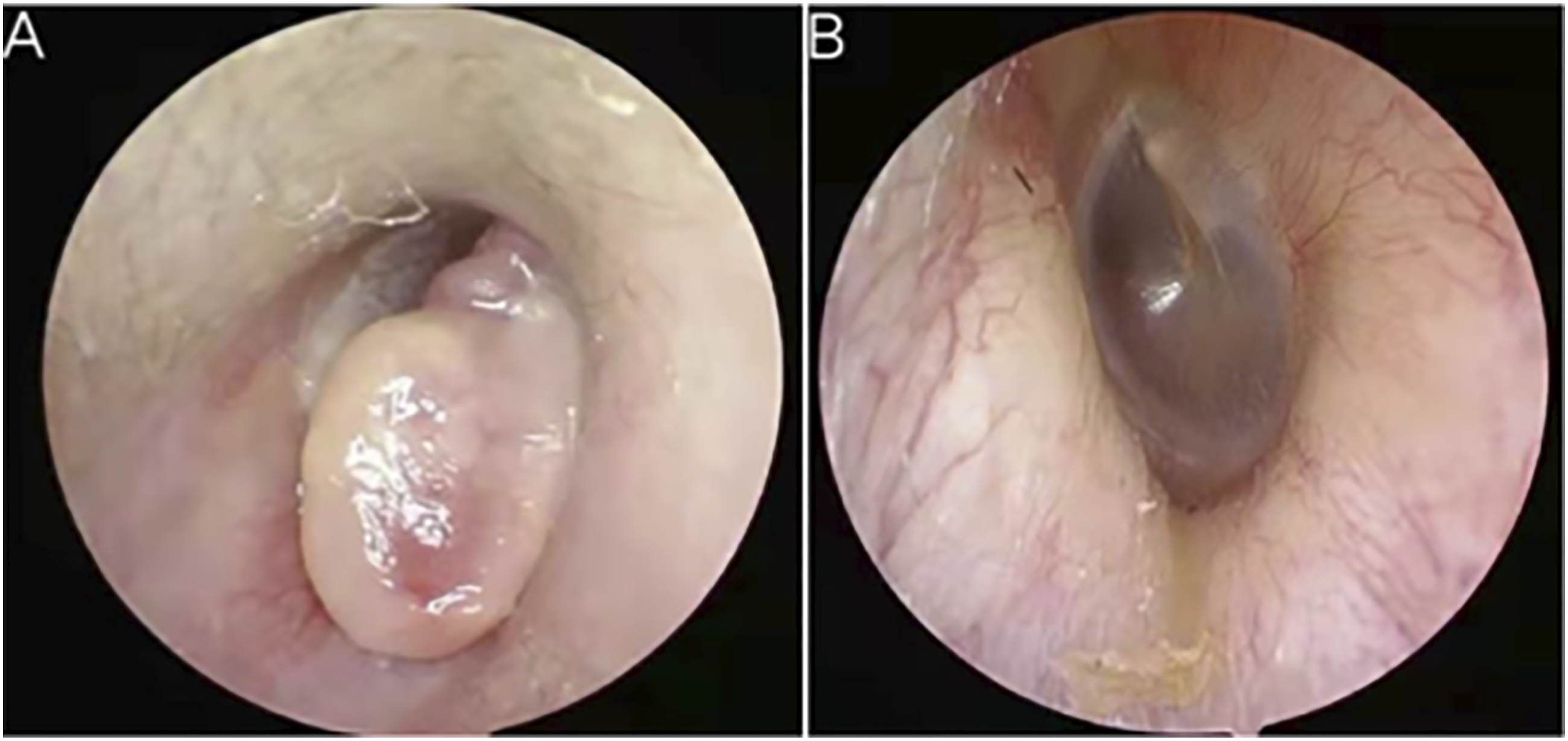
Pure-tone audiometry indicated a mild sensorineural hearing loss in the right ear (Figure 4A). On imaging examination, high-resolution CT (HRCT) of temporal bone showed a nodule with a diameter of about 7 mm in the right external auditory canal. The edge was clear, while the boundary between the nodule and the inferior wall of the external auditory canal was unclear. There was no apparent damage to the bone wall of the external auditory canal (Figure 4B-E). A: Pure tone electrical audiometry. B-C: Coronal CT scan of the temporal bone. The mass is indicated by the arrow. D–E: Sagittal CT scan of the temporal bone. The mass is indicated by the arrow.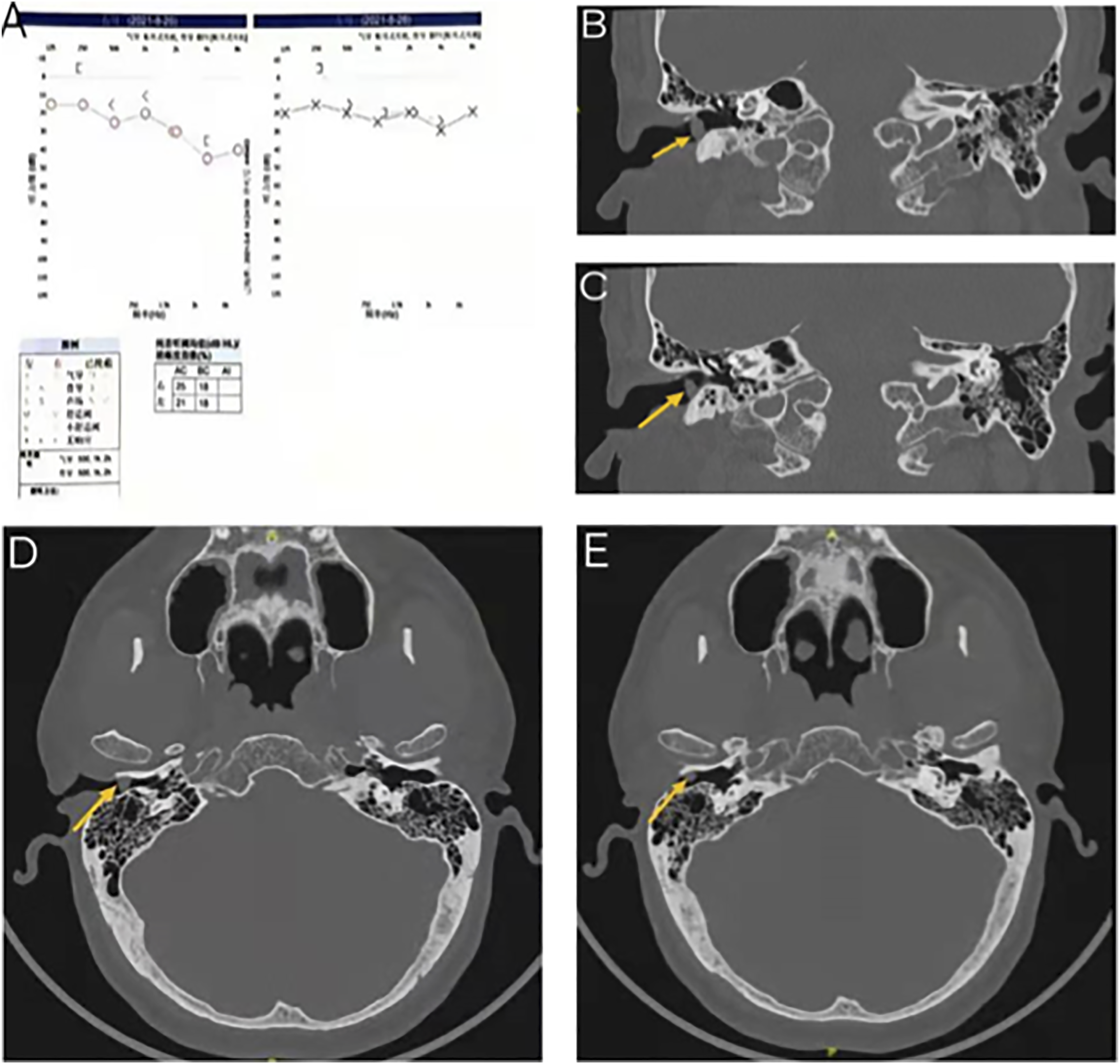
We completely removed the tumor through the ear canal under the otoscope and there was no adhesion between the tumor and the basal tissue. Skin grafting was not performed due to the small base. The result of intraoperative freezing showed superficial necrosis, with underlying fibrous proliferation and vascular proliferation. Local spindle cell proliferation was significant, bone tissue was present, and cells were slightly atypical. The diagnosis of nodular fasciitis was based on the routine pathology after the operation. IHC: B1: SMA (+), CD10 (+), CD68 (+), Desmin (-), Ki-67 (3-5%, +), S-100 (minor +), and CD34 (vascular + ).The USP6 gene was positive (Figure 5). A: Hematoxylin and eosin stain(H&E stain). B: CD68. C: CD10. D: ki67. E: sma. F: Fluorescence in situ hybridization(FISH) of the USP6 gene.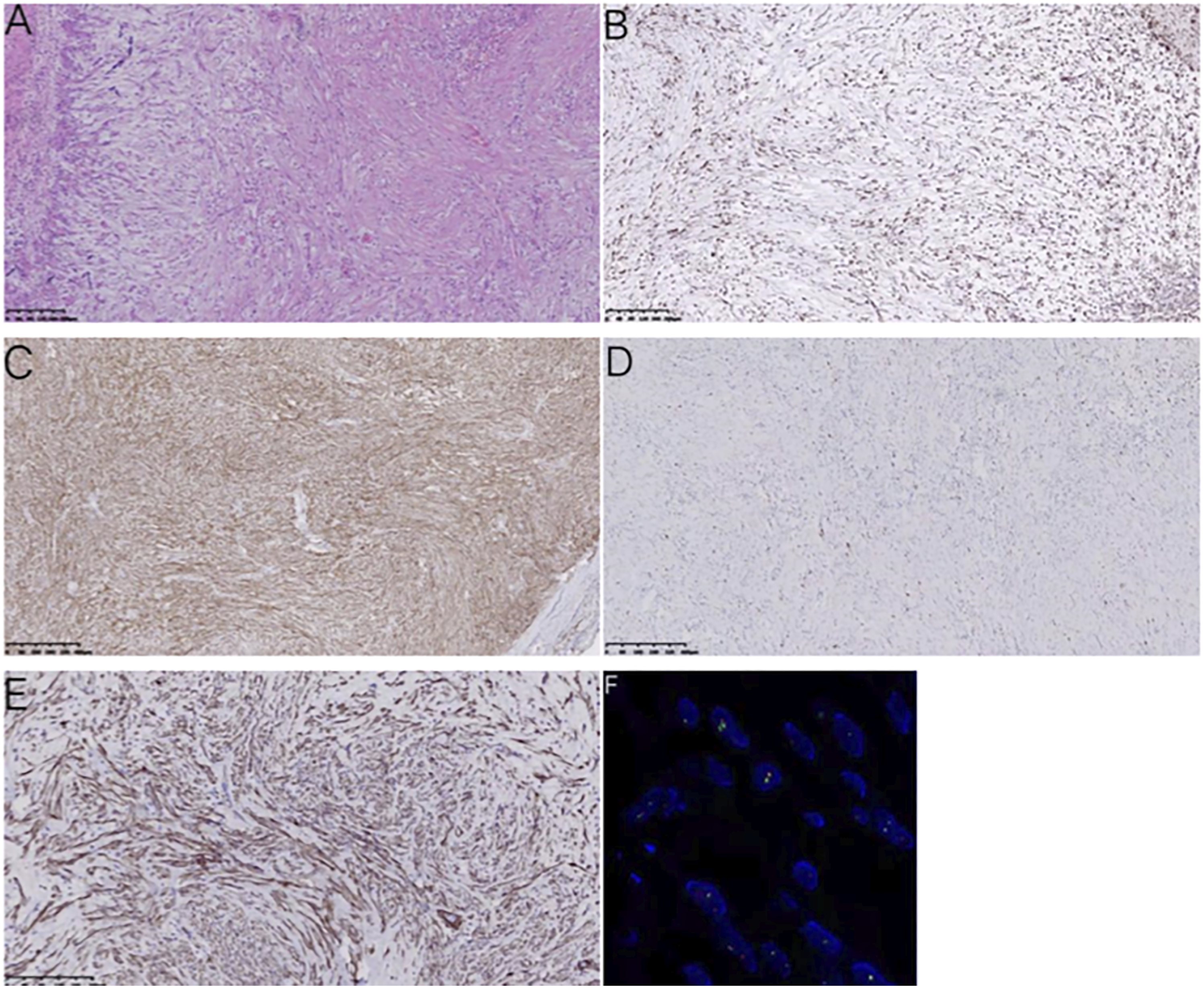
During the 7-month follow-up, the right external auditory canal of the patient was unobstructed and there was no recurrence of the tumor.
Discussion
Nodular fasciitis is a proliferative lesion composed of fibroblasts and myofibroblasts that generally affects subcutaneous tissue, fascia, and muscles. 1 NF can occur at any age, but it occurs primarily in young adults aged 20–40, regardless of sex. It can present as a fast-growing mass in a few weeks, which is self-limiting and rarely malignant, usually less than 2 cm in diameter. 2 Furthermore, NF can arise on multiple parts of the body, and the most common site is the upper extremities. It can also affect the lower extremities, the trunk, and the head and neck region, with up to 13–20% of NF arising in the head and neck region. 3 Although the head and neck region is relatively common, involvement of the nose is rare and seldom reported. In 1995, Harrison et al. published the first report on nasal NF, 4 and only then a few related reports included cases of nasal NF.5-7 The involvement of the ear is more common than that of the nose, accounting for about 1.5% of all cases of NF. Representative cases of the ear were reported by Thompson et al. and Ahn et al.8,9 In general, NF of the nose and ear is less common and is often unilateral, and most masses have clear boundaries and rapid growth.
Compared to fasciitis in other parts of the body, NF often occurs as a sporadic solid or cystic mass in the head and neck region, which tends to shrink in size, but is more likely to involve skeletal muscle. 10 Because nasal NF is in the middle of the face, it can easily cause facial damage and affect the appearance, which influences the physiology and psychology of the patient, thus affecting quality of life. Additionally, nasal NF often has a short course, rapid growth, and continuously compresses surrounding tissues, such as the nasal septum and alar cartilage, resulting in altered nasal appearance. 7 NF of the ear is more prevalent than nasal NF and usually occurs in young adults, which is more common in the preauricular and postauricular area and less common in the external auditory meatus. The lesion is mainly in the dermis, accompanied by a superficial ulcer and hemorrhage. It is compressive to the surrounding bone wall and causes discomfort in the ears. The large lesion can also cause hearing loss. Among the fifty cases of NF in the auricular region collected by Thompson et al. 37 cases (74%) were in the preauricular and retro-auricular areas, and six cases (12%) were in the external acoustic meatus. One of them had conductive hearing loss. In this report, the average size of the lesions in the external auditory canal was 1.3 cm, and the average duration of the symptoms was 1.6 months, which were smaller than those of NF in other locations (1.9 cm, 5.0 months). Additionally, compared to the recurrence rate (1%–2%) at other sites, the local recurrence rate (9.3%) of NF in the auricular region was higher. 8
Although imaging tests lack high specificity for the diagnosis of NF, some imaging signs can serve as a reference for differential diagnosis. On CT, NF is presented as a soft tissue density mass adjacent to the fascial layer, and the mass is flat or oval, homogenous, and well-circumscribed. Most cases of NF can present homogenous density tumors adjacent to the fascial layer. Furthermore, the fascia extends linearly and the fascia near the tumor is slightly enhanced after enhancement, which is known as the fascial tail sign. 11 It is a valuable marker for distinguishing NF from other superficial tumors. On MRI, NF usually presents as a solitary oval mass with a clear boundary and a regular morphology. Compared to skeletal muscle, most cases of NF showed homogenous isointensity in T1WI and hyperintensity in T2WI. There are also some specific imaging signs on MRI: the inverted target sign is, in the T2WI hyperintensity area, the center of the lesion without any enhancement, while the peripheral with notable enhancement; the fascia tail sign is known as the thickened fascial layer around the lesion, and the linear extension after enhancement that resembles a tail; the solar halo sign is the notable and irregular enhancement of the fascia layer near the lesion, with mild or no enhancement of the lesion, which resembles a halo around the sun; the cloud sign is the growth of the lesion along the fascia into the muscle that resembles a cloud covering the sun. These signs, especially the fascial tail sign and the cloud sign, are helpful in distinguishing NF from other soft tissue diseases. 12 On CT and magnetic resonance imaging, superficial NF usually presents as a relatively well-defined soft tissue mass, while the deep lesion tends to be more significant and less well-defined, that is, the deep lesion may exhibit aggressive behavior similar to that of the malignant tumor. Therefore, NF can be easily confused with other diseases. 13
Pathological examination can be used as evidence to establish the diagnosis of NF. Immunohistochemical detection and USP6 gene rearrangement are of great significance. Macroscopically, NF is an unencapsulated, tan or whitish, round or oval mass. Microscopically, proliferative myofibroblasts are stellate or spindle, arranged in short bundles, interwoven or semistriated patterns, with oval nucleoli and basophilic cytoplasm. The tissue is loose and rich in mucus, with tissue fissures, red blood cell extravasation, and other classic histological features of NF. 14 On the basis of the amount and type of extracellular matrix, NF can be divided into mucinous, cellular, and fibrous types, and these three types can appear simultaneously in the same case. Immunohistochemical detection is more helpful for the diagnosis of NF. In immunohistochemistry, vimentin and SMA(anti-actin antibody) are diffusely positive, and smooth muscle actin, troponin, muscle-specific actin, CD10, and CD68 can also be positive. 15 In approximately one-third of NF, cytoplasmic staining for β-catenin can be positive, while immunostaining for desmin, corpus callosum, S-100, keratin, CD-34, ALK, and P53 are negative. 16 Rearrangement of the Ubiquitin-specific protease 6 (USP6) gene is the most frequent specific manifestation in NF, and most cases of NF have been confirmed to express the USP6 gene rearrangement. The USP6 gene, located on chromosome 17p13, encodes a deubiquitinase that regulates intracellular transport, protein transport, inflammatory signaling, and cellular transformation. 17 Erickson-Johnson et al. found that 92% (44/48) of NF cases could detect USP6 gene rearrangement by FISH, and the sensitivity and specificity of FISH for diagnosis were 93% and 100%, respectively. 18 Amary et al. reported the expression of USP6 gene rearrangement in 31 of 34 cases, and the sensitivity of FISH was 91%. 19 Furthermore, when performing USP6 detection in 20 patients, Shin et al. found that, in the morphologically distinct cases, the sensitivity of FISH for diagnosis was 86%, the specificity was 100%, the positive predictive value was 100%, and the negative predictive value was 90%. 20 These indicate that in the diagnosis of NF, the detection of USP6 by FISH, as a supplementary diagnostic tool, has a high application value. Especially when the morphology of NF is not characteristic, it can significantly reduce the risk of misdiagnosis and inappropriate treatment. As discussed above, the histopathological morphology and immunophenotype of the two cases reported in this article are consistent with the manifestations of NF.
Nodular fasciitis, as a rare soft tissue disease, can be easily confused with other benign or malignant spindle cell lesions, such as benign fibrous histiocytoma (BFH), myxoma, inflammatory myofibroblastic tumor (IMFT), and myxofibrosarcoma. Occasionally, with multinucleated giant cells and few or no ganglion-like cells, NF can be confused with BFH, but NF has a shorter course and faster growth. Some cases of NF are hypocellular with notable myxoid changes, which can be misdiagnosed as myxoma, but NF lesions are deeper. 21 On cytology, IMFT is similar to NF, while IMFT is usually located in the abdominal cavity, and spindle cell proliferation accompanied by inflammatory cell infiltration can be observed on pathological examination. In addition, myxofibrosarcoma occurs mainly in patients over the age of 50 years, with a long history and characteristic curvilinear vessels.21,22 NF has a certain degree of invasiveness and can invade the periosteal tissue, which is easily confused with malignant tumors such as spindle cell sarcoma. Sarcoma has a longer course and larger mass and commonly arises in the lower extremities, with a high degree of cellular atypia revealed by pathological examination. 23 If sarcoma is misdiagnosed as NF, it will delay treatment, and if NF is misdiagnosed as sarcoma, it will cause excessive or disabling surgical injury during treatment, causing great pain for patients. Therefore, the pathological examination and differential diagnosis of NF are particularly significant.
The primary treatment for NF is surgical excision, but the main reason for recurrence is incomplete resection of the lesion, with a rate of less than 10%, probably due to the lesion site.24,25 Furthermore, some cases of NF that are not suitable for surgery can be treated by intralesional corticosteroids, and the clinical effect is good. For example, Keren S et al. treated the periorbital mass with an intralesional injection of triamcinolone acetonide in a child diagnosed with NF. The lesion completely changed after four months and there was no recurrence after 12 months of follow-up. 26 Husain A et al. found that steroid injection was administered to a patient with NF that recurred six months after surgical resection of the right temporal region, and the lesion was significantly involuted in only two weeks. 27 Furthermore, because some cases of NF can spontaneously resolve, clinical follow-up can be an option for patients who are not suitable for surgery. Rani D et al. found that in 7 of 9 patients diagnosed with NF after cytological aspiration, the mass (located anywhere in the body) spontaneously resolved within 2–16 weeks [28]. In the cases we reported, the tumor was completely removed along the safety margin and there was no recurrence at follow-up.
Although NF of the nose and ear is rare, a precise diagnosis and appropriate treatment are still important to otolaryngologists. In the case of an irregular or fast-growing mass in the head and neck region, especially in the face and the external auditory canal, we should consider the possibility of NF to make a correct diagnosis.
Footnotes
Author’s Note
Tianhong Zhang is the corresponding author, and she contributed to the conception of the study. Wanjie Luo and Tianyu Ma are the co-first authors who contribute to writing this manuscript. SiQi Wang, Xiaowei Qin, and Li Jiang contribute to collecting all images. Yuyao Wang contributes to modify the manuscript. All authors read and approved the final manuscript. Wanjie Luo and Tianyu Ma contributed equally to this work
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The research is approved by the Ethics Committee of the first hospital affiliated Harbin Medical University.