
Abstract
Neurofibromas are benign peripheral nerve sheath tumors that can originate from several elements of peripheral nerves, including axons, Schwann cells, endoneurial fibroblasts, and perineurial cells. The occurrence of a solitary neurofibroma in the external nose, especially that isolated in the nasal columella, is extremely rare. To the best of our knowledge, only 4 cases of solitary neurofibromas in the external nose have been reported in the English literature: on the nasal dorsum, tip, and pyriform aperture, all originating from the trigeminal nerve. We report the first case of a solitary neurofibroma isolated in the nasal columella, which we found in an otherwise healthy 42-year-old man. We completely resected this tumor with a negative resection margin and performed reconstruction with a bilateral spreader graft and caudal septal extension graft using autologous septal cartilage. The postoperative course was successful in both cosmetic and functional results, with no sensory changes at the 1-year follow-up. Surgical treatment for this lesion was challenging due to the cosmetically obvious location and high rate of recurrence. A review of the literature highlights the clinical and histological characteristics, differential diagnosis, and management of solitary neurofibroma of the external nose.
Introduction
Neurofibromas are benign peripheral nerve sheath tumors that originate from proliferation of several peripheral nerve elements, including axons, Schwann cells, endoneurial fibroblasts, and perineurial cells. 1 Focal benign tumors can occur as isolated lesions, but multiple lesions generally appear in patients with neurofibromatosis type 1 (NF1). 2 Neurofibroma can develop in any anatomic location, but a neurofibroma originating from the external nose is rare. 3 To the best of our knowledge, only 4 cases of solitary neurofibroma on the external nose have been reported in the English literature, and all originated from the trigeminal nerve. 1,3 -5 An isolated solitary neurofibroma of the nasal columella is even more rare and quite challenging to treat surgically in view of its location, cosmesis, and high recurrence rate. Herein, we are the first to present a successful experience of a solitary neurofibroma arising from the nasal columella.
Case Presentation
A healthy 42-year-old man presented with a painless mass on the nasal columella that had not changed in size for 10 years. His chief complaint was cosmetic. He had no nasal symptoms such as nasal obstruction or bleeding and did not complain of any sensory changes of the nose, philtrum, or upper lip. He denied history of nasal trauma or surgery or familial history of neural tumors. He did not have nodular mass-like lesions at other sites. On his nose, a round, soft, non-tender, and movable mass was located at the middle portion of the nasal columella. It was approximately 1 × 1 × 0.5 cm in size and covered by thinned but intact skin (Figure 1A).
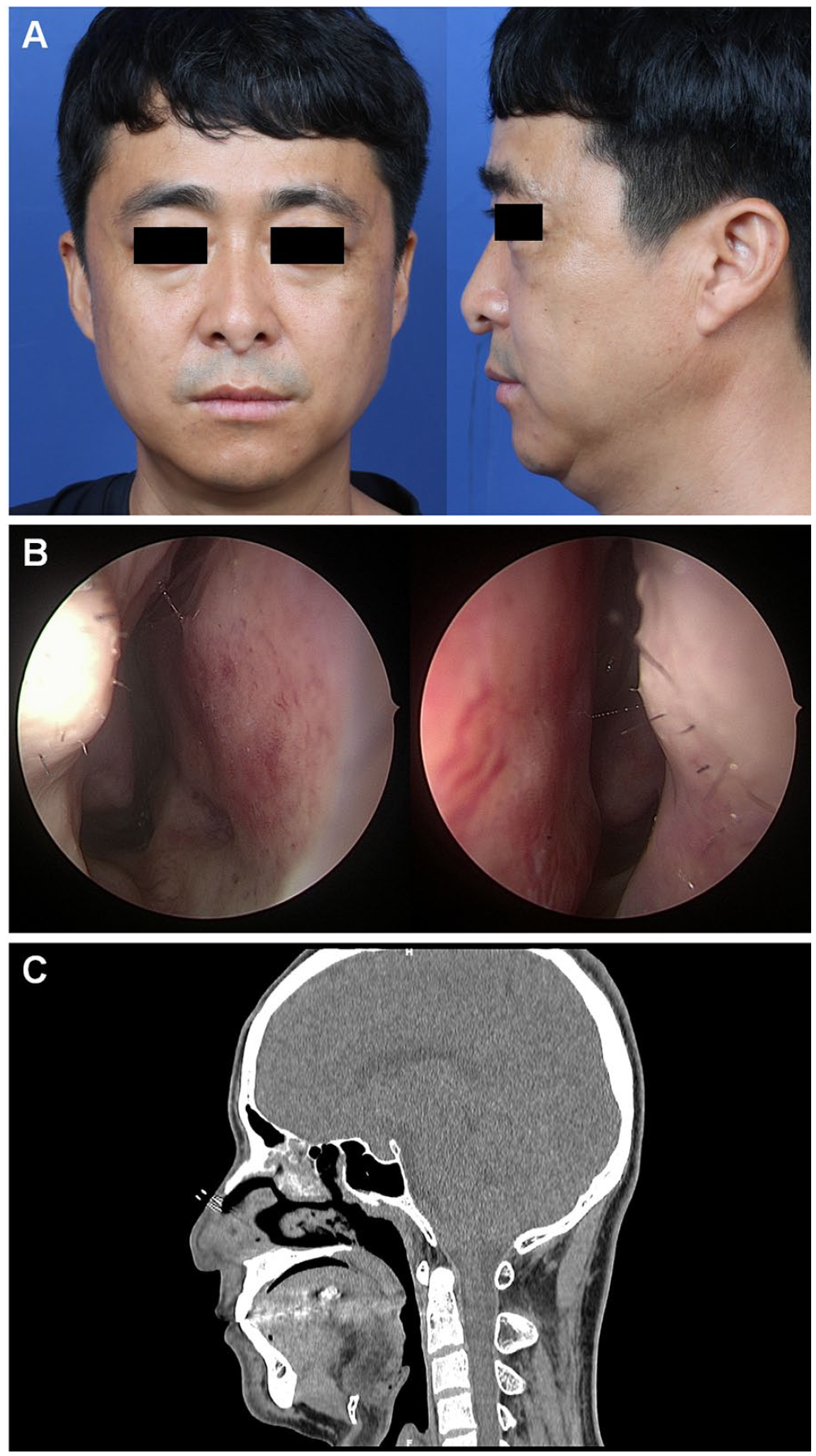
Preoperative workup of the patient.
Nasal endoscopy revealed a nasal septum deviated to the left but no other abnormalities (Figure 1B). Paranasal computed tomography (PNS CT) scans without contrast enhancement demonstrated a 1.2 × 0.9-cm, well-defined, round, solitary mass on the columella (Figure 1C). Mild nasal septal deviation to the left and soft tissue densities in the left ethmoid and maxillary sinuses, thought to be chronic sinusitis, were also identified.
He was concerned that his nose would be upturned after the tumor was removed and wanted to correct the slight external nose deviation to the left if possible. We planned surgical mass excision and septorhinoplasty. Under general anesthesia, complete surgical excision of the mass was performed via an inverted “V” shaped transcolumellar incision and a marginal incision through the anterior end of the lower lateral cartilage. The tumor was 1 × 0.8 cm in size, not encapsulated, and gelatinous in appearance (Figure 2A). It was excised with clear resection margins without extension to the nasal septal cartilage or lower lateral cartilage (Figure 2B). The nasal columellar defect was reconstructed using nasal septal cartilage harvested during septoplasty. A right septal extension graft and bilateral extended spreader grafts were performed to control the projection and rotation of the tip and nasal lengthening (Figure 2C). The excessive sagging skin of the columella was appropriately cut and primarily sutured.
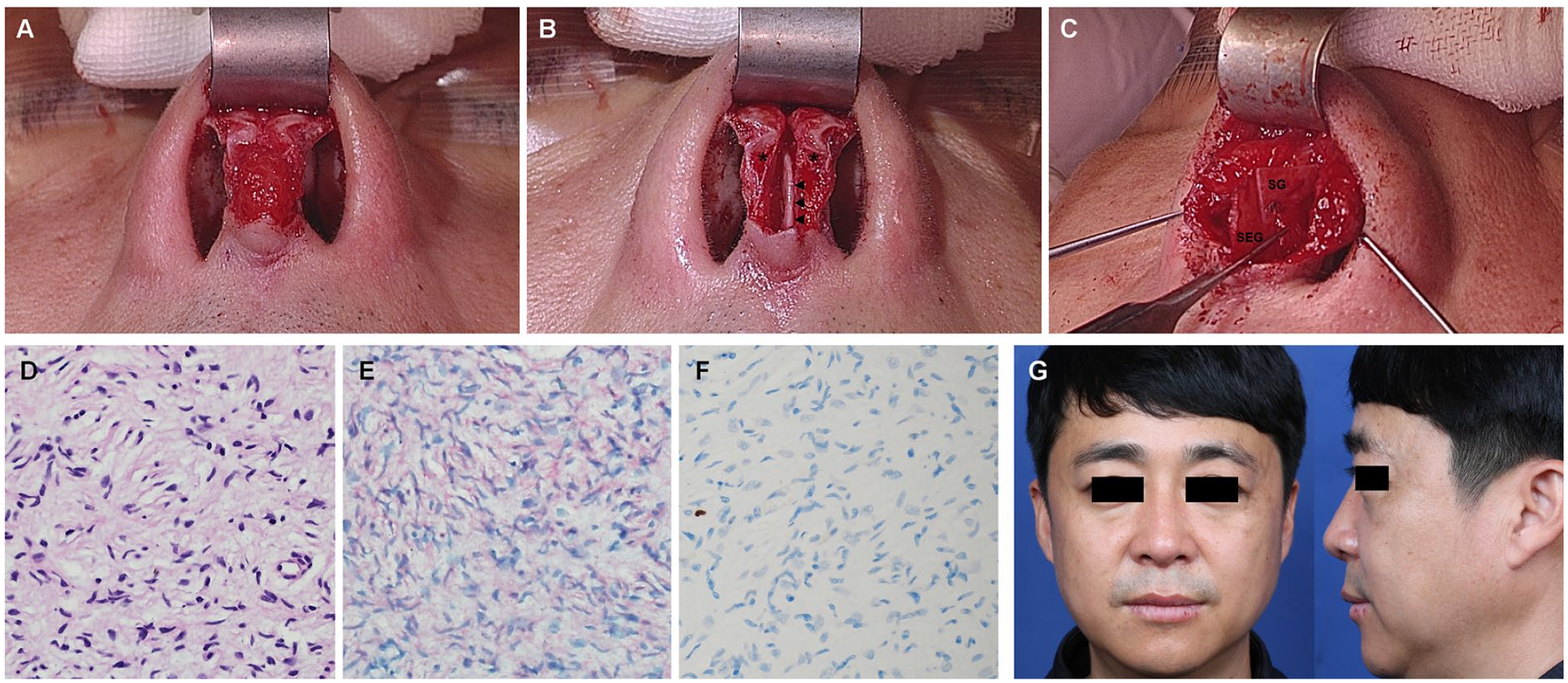
Intraoperative and histopathological findings. (A) Photograph showing the gelatinous mass on the nasal columella during surgery. (B) Photograph after en bloc mass excision. There was no extension to the nasal septum or lower lateral cartilage (arrow heads: caudal nasal septum, asterisks: lower lateral cartilage). (C) Reconstruction was performed using nasal septal cartilage. A right septal extension graft and bilateral extended spreader grafts were performed. (D) Microscopic examination showed that the neurofibroma consisted of spindle cells, with disorderly proliferation and wavy, tortuous nuclear bundles (H&E stain). (E) Positive immunoreactivity for S-100. (F) Negative immunoreactivity for Ki-67 (400×). (G) Postoperative medical photography at 6 months after the operation. H&E, hematoxylin and eosin; SEG, septal extension graft; SG, extended spreader graft.
Histopathological findings of the specimen demonstrated a solitary neurofibroma in which disordered spindle cells proliferated with wavy, tortuous nuclear bundles (Figure 2D). Immunohistochemical staining of the spindle-shaped tumor cells showed a positive reaction to S-100 (Figure 2E) and no reaction to Ki-67 stain (Figure 2F). The postoperative course was successful, with excellent cosmetic and functional results and without sensory changes. There was no recurrence during the 12-month follow-up period (Figure 2G).
Discussion
Neurofibromas can take 1 of 2 types: solitary or plexiform. 6 The solitary type is usually associated with a lone peripheral nerve and produces well-delineated, rubbery, and firm lesions. On the other hand, the plexiform type is associated with many nerve bundles and infiltrates aggressively through soft tissue. Neurofibromas can be seen in diffuse forms in patients with autosomally dominant NF1, and they are rarely seen in their solitary form. Therefore, café-au-lait spots and other cutaneous nodules suspicious of neurofibromatosis or that characterize cutaneous neurofibromas should be thoroughly investigated to rule out the possibility of neurofibromatosis. 3,7,8 Neurofibromas can be found in any anatomical location, but they are most commonly found in the head and neck area. 2 However, only 4% of the neurofibromas found in the head and neck area invade the paranasal sinuses or nasal cavity. 9 Interestingly, this case presented with a solitary neurofibroma contained within the nasal columella.
The nasal columella is a rare location for neurofibromas. Nasal neurofibromas usually have nonspecific symptoms, such as nasal obstruction, swelling, epistaxis and proptosis, or facial pain. 1,3 -5 In our case, the tumor did not produce any special symptoms, and the biggest problem was cosmetic. When a mass is found in the nasal columella, a radiological study is necessary before surgery. 10 In this case, only a non-enhanced PNS CT scan was obtained. Because it can more finely differentiate the tumor from adjacent soft tissues, magnetic resonance imaging (MRI) is thought to be a higher-grade modality than CT. 9 -11 It might have been better to perform MRI so that the surgical excision could have been more accurately planned. However, not all cases of neurofibroma require MRI. Other preoperative diagnostic tests, such as fine-needle aspiration (FNA) biopsy, can also be used to evaluate the tumor, although it is difficult to differentiate neurofibromas from other non-epithelial tumors by FNA biopsy. 11
To our knowledge, only 4 cases of solitary neurofibromas in the external nose have been reported. In those cases, the solitary mass occurred on the nasal dorsum, 3 nasal ti, 4 and nasal ala. 1,5 The case presented here is unique in that it describes a solitary neurofibroma confined to the nasal columella. In the nasal dorsum and nasal tip, complete mass excision was performed using an open rhinoplasty approach, and no complications or recurrence were observed during a 12-month follow-up period. 3,4 On the other hand, the cases occurring in the pyriform aperture, reported by the same author, were treated using en bloc resection via an intranasal approach. 1,5 Neither of those cases showed recurrence during the 18- and 12-month follow-up periods, respectively, and good functional and aesthetic outcomes were maintained. The open rhinoplasty approach provides the widest surgical exposure, which enables safe and effective en bloc resection, but it can result in a transcolumellar scar and could cause columellar flap necrosis, as well as prolonged surgical time. In our case, the open rhinoplasty approach was inevitable because we needed to completely remove the nasal columellar mass with a negative resection margin.
Histological examination is the gold standard and most reliable method for diagnosing neurofibromas. In this case, our histopathological examination of the specimen revealed a solitary neurofibroma with spindle cells proliferating in disordered arrangements and nuclear bundles that appeared wavy and tortuous. 12 The spindle-shaped tumor cells demonstrated positive immunoreactivity for the S-100 protein, a neural crest-derived cell marker. Most neurofibromas have a benign course, though malignant changes are possible and occur in 1 to 5% of cases. 13 Mitotic activity and nuclear pleomorphism are usually not indicative of malignancy. We used Ki-67 stain, a marker of cellular proliferation, to exclude malignancy. 14 Overexpression of the p53 protein can also serve as a useful biomarker for evaluating the malignancy of tumors. 13,14
In this case, we performed tumor removal and reconstruction together, but a 2-stage operation is generally needed when there is a high risk of recurrence. 6,15 Moreover, close observation is required when a malignant transformation is likely. 13,14 On the other hand, delayed nasal reconstruction would have been unsatisfactory in this case because the patient's only complaint was cosmetic. In this case, the mass was excised with clear resection margins under appropriate oncological precautions, and no recurrence occurred during the 12-month follow-up period. We decided that a 2-stage operation was not mandatory because of the patient inconvenience incurred by delaying reconstruction.
Conclusion
This case highlights the importance of considering neurofibroma as a differential diagnosis for a nasal columella mass, even in rare locations, and the importance of a comprehensive surgical plan that considers both tumor removal and reconstruction of the nasal defect.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education [Grant number: NRF-2022R1C1C1004860 to YJJ].
Ethical Approval
The requirement of ethical approval was waived for this Case Report, as determined by our institutional review board.
Patient Consent
Written informed consent was obtained from the patient for the use of his images.