
Abstract
Hamartomas are benign tumors characterized by an abnormal combination and arrangement of normal tissues during development. It is more common in lung, gastrointestinal tract and other parts, rare in the head and neck, such as oral cavity, nasal cavity, nasopharynx, etc. This case report describes a patient with nasopharyngeal hamartoma who presented with headache and rhinorrhea and was confirmed to have smooth nasopharyngeal neoplasm by electronic fibro laryngoscopy. After admission, the nasopharyngeal neoplasm was removed under general anesthesia and was postoperatively diagnosed as a hamartoma polyp. The patient recovered well postoperatively.
Introduction
Hamartomas are tumor-like malformations that generally grow slowly and rarely become malignant. They commonly occur in the lungs, skin, liver, chest wall, kidneys, and gastrointestinal tract, and rarely in the head and neck, even more rarely in the mouth, nasal cavity, nasopharynx, laryngopharynx, tongue, Eustachian tube, and larynx.1,2 In recent years, clinicians and pathologists have been aided by the development of endoscopic technology which has improved our understanding of the disease, and facilitated the identification of an increasing number of hamartomas. However, by reviewing the relevant literature, we found that the proportion of head and neck hamartomas diagnosed in infants was higher than that in adults. 3 Here, we report a case of adult nasopharyngeal hamartoma treated at our hospital, which was diagnosed and cured by endoscopic surgery.
Case Report
A 47-year-old man was admitted to our hospital presenting with a headache and runny nose. Six months prior, the patient developed a headache without an obvious cause, accompanied by clear nasal discharge after eating hot and spicy food, and occasional minor nasal bleeding. Electronic fiber laryngoscopy revealed neoplasms in the nasopharynx, and narrowband imaging did not identify any obviously dilated microvessels on the mucosal surface or malignant lesions (Figure 1). Further examination was performed and an enhanced computed tomography (CT) of the pharynx showed a soft tissue protrusion in the top lateral wall of the nasopharyngeal, with a length of about 1.0 cm and a slightly wide width of about 1.2 cm at the base, and an uneven density. An enhanced scan revealed mild enhancement and a fat-dense shadow (Figure 1). Magnetic resonance imaging (MRI) of the nasopharynx showed an irregular short T1 and equal-length T2 signal, and the fat suppression image indicated a slightly high signal. The mass connected with the top of the nasopharynx to the left, with a size range of approximately 1.5 × 1.0 × 2.1 cm (left and right × front and back × upper and lower), and showed an uneven signal. Contrast-enhanced MRI of the nasopharynx revealed a soft tissue lesion on the left side of the nasopharyngeal top wall, which showed marked heterogeneous enhancement (Figure 1). Physical examination revealed that the patient’s general condition was acceptable, and no obvious abnormalities were found in the heart, lungs, and abdomen. Based on the patient’s medical history and the related auxiliary examinations, the nasopharyngeal neoplasm was initially considered a benign lesion. Enhanced CT and MRI revealed no bone destruction in the nasopharynx. During the operation, a nasal endoscope was inserted into the patient’s right nasal cavity, and a nasopharyngeal mass with a smooth surface and base was located at the top of the nasopharynx and left lateral wall. A plasma electric knife was inserted into the patient’s left nasal cavity, and low-temperature plasma was used to completely remove the mass along the base, with minimal bleeding (Figure 2). Postoperative pathological examination revealed hamartomatous polyps (Figure 3). The patient showed promising postoperative results and recovered well.
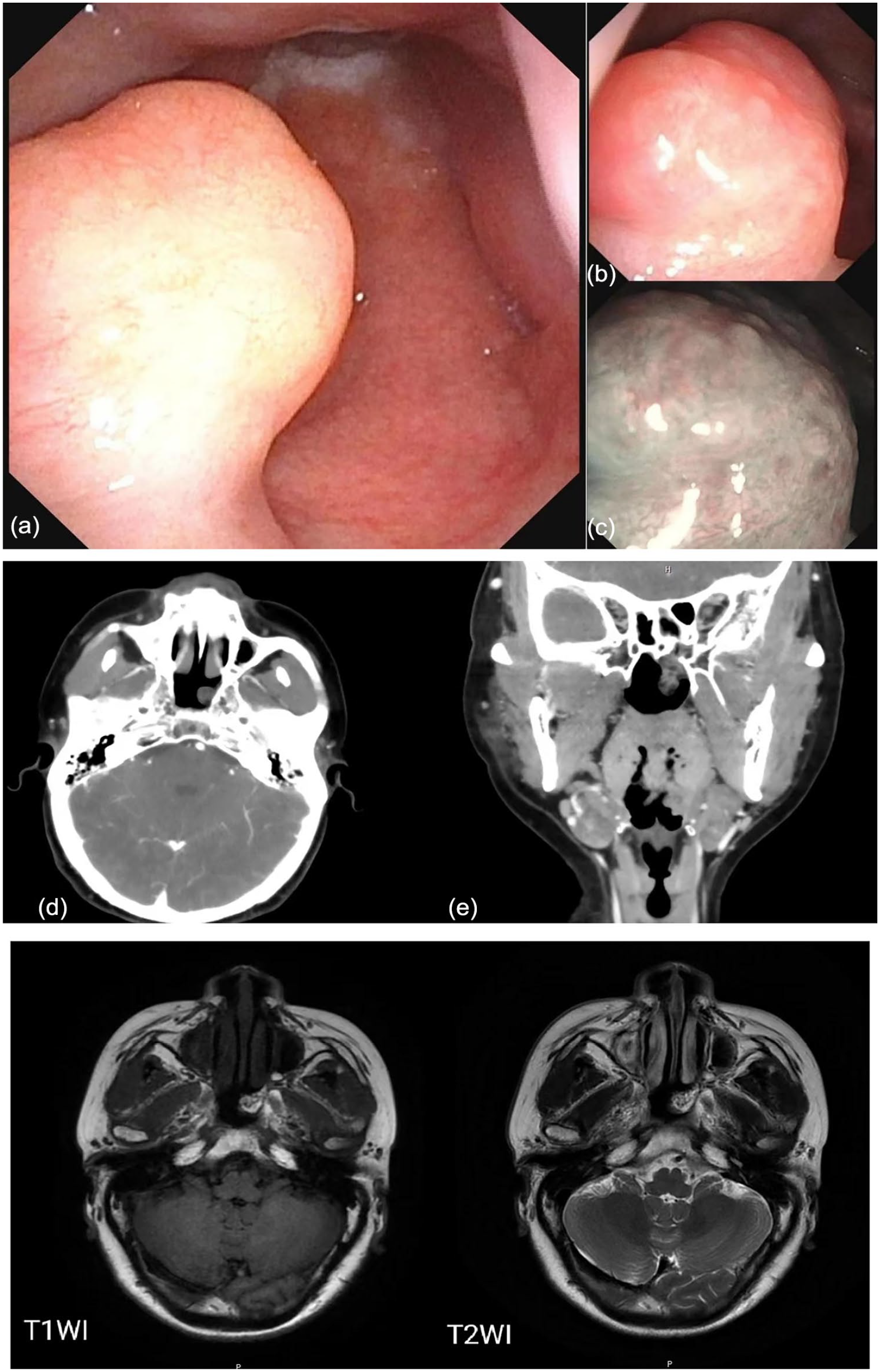
(a and b) Fiber laryngoscopy reveals a smooth upliftment of the left lateral wall of the nasopharynx with a smooth pink surface. (c) Narrowband imaging pattern shows faintly visible microvessels on the mucosal surface without any obvious dilation. (d) Examples of the axial-enhanced computed tomography (CT) of the nasopharynx and (e) coronal-enhanced CT of nasopharynx; contrast-enhanced CT of the nasopharynx revealed a soft tissue protrusion on the left side of the top of the nasopharynx, and the enhanced scan showed mild enhancement. Axial T1WI showed irregular short signal shadow on the left lateral wall of the nasopharynx. Isometric T2 signal.
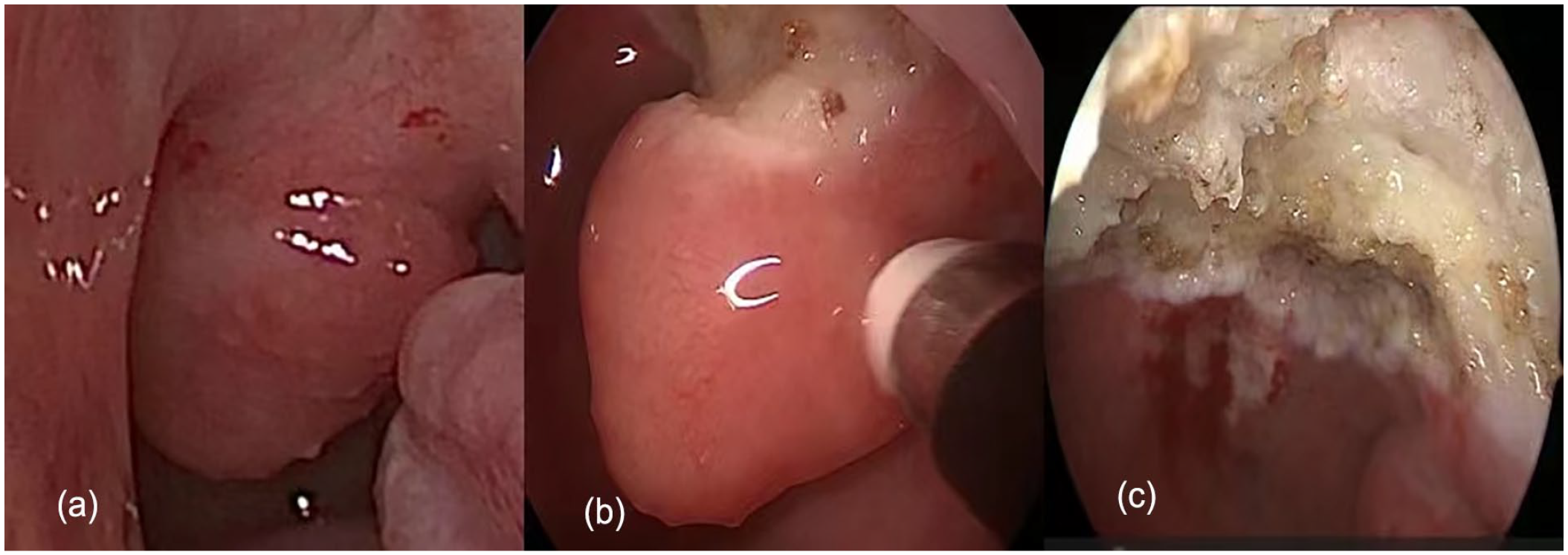
(a) A reddish neoplasm on the left lateral wall of the nasopharynx was identified preoperatively. (b) During the operation, the neoplasm along the base was completely removed with plasma. (c) The postoperative surgical wound was small without obvious bleeding.

(a) At a low magnification, the polyp is covered by respiratory epithelium. (b) Using a medium magnification revealed hyperplastic blood vessels, smooth muscle, and a large amount of adipose tissue in the interstitium. (c) At high magnification, residual intrinsic mixed glands were seen.
Discussion
Hamartomas were first described by Albrecht in 1904 and are thought to be caused by the proliferation of abnormal tissues during pre- and postnatal development and to be benign tumors.4 -7 Hamartomas are classified as epithelial, mesenchymal, or mixed epithelial-mesenchymal types. Adenomatoid hamartoma of the respiratory epithelium adenomatoid hamartomas are a subtype of epithelial hamartomas. 8 It is also the most common type of hamartoma of the nasal cavity and nasopharynx. The clinical manifestations of hamartomas in the nasopharynx lack specificity. A review of the relevant literature revealed that nasal airway obstruction, nasal obstruction, hyposmia, headache, facial pain, rhinorrhea, and posterior rhinorrhea were the most common clinical manifestations. 9 Hamartomas generally present as a single round mass with a smooth surface, similar to inflammatory polyps, pink or off-white in color, located under the mucosa, with a smooth surface and soft texture. The hamartoma manifested as a mass with heterogeneous density and calcification on CT scans. Bone erosion and destruction were observed when the tumor was larger. On MRI, T1 was isointense, T2 was slightly hyperintense, and after enhancement, uneven enhancement and a cystic cavity were also observed. 10 Due to the lack of specificity in clinical manifestations and imaging characteristics, nasopharyngeal hamartoma should be differentiated from various benign and malignant lesions in clinical diagnosis, as follows: (1) Hemangioma: bright red or light purple in color, smooth surface, soft texture. MRI revealed hypointensity on T1, hyperintensity on T2, and marked contrast enhancement; (2) Glioma: pink in color and medium or hard in texture. CT showed an expansile mass with a density similar to that of the brain tissue, but the skull base bone was intact. On MRI, both T1 and T2 showed high signal intensities, but the enhancement was not obvious; (3) Meningoencephalocele: a round or semicircular mass in the nasal cavity, soft, smooth surface, and pulsating; the mass can become large when holding breath. CT and MRI confirmed a bone defect in the skull base, the mass communicated with the brain, and the signal intensity of MRI was the same as that of the brain tissue. In this case, the patient mainly presented with headache, rhinorrhea, and smooth neoplasm in the nasopharynx under an electronic fiber laryngoscope. Nasopharyngeal hemangioma and meningoencephalocele were not initially ruled out. Therefore, in addition to actively improving nasopharyngeal-enhanced CT, MRI, and other examinations before surgery, blood transfusions were also performed to reduce the occurrence of accidents. The amount of bleeding during the resection of the neoplasm was low in this patient, and there was no obvious vascular plexus around the neoplasm. Combined with other relevant imaging examinations, the diagnosis of hemangioma was excluded; however, the diagnosis of hamartoma mainly depended on the histopathological features including a tumor-like proliferation of mature tissue components with disordered structure. The postoperative pathological assessment of this case met the histological definition of hamartoma including having 3 well differentiated components (blood vessels, smooth muscle, and adipose tissue). The data confirmed that the final diagnosis was hamartoma.
Conclusions
Head and neck hamartomas are rare in clinical practice, and their preoperative diagnosis is very difficult with a high rate of misdiagnosis. Imaging studies should be implemented to assist in the diagnosis of slow-growing, smooth-appearing masses of the head and neck, particularly the nasopharynx. After excluding hemangiomas, gliomas, meningoencephaloceles, and other tumors, the possibility of this disease should be considered. Although hamartomas are self-limiting diseases, their clinical manifestations remain unclear. Hamartomas can be treated surgically to relieve symptoms and eliminate the lesions. Clinicians must make a differential and definitive diagnosis as early as possible to avoid misdiagnosis and improve patient outcomes.
Footnotes
Acknowledgements
I sincerely thank my tutor Li Lianqing for his valuable advice and careful guidance on the revision of the article, and thank all the authors for their selfless help in data collection.
Authors’ Contributions
YF: Data collection and article preparation; YF, ML, and YD: Article preparation; GJ: Picture collection; LL and LG: Article preparation and review. All authors read and approved the final article.
Consent for Publication
The patient provided us informed consent for the publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This article was approved by the Ethics Committee of Liaocheng People’s Hospital.