
Abstract
Burkitt Lymphoma (BL) is a highly aggressive B-type non-Hodgkin lymphoma. It rarely develops at the level of the sinonasal cavities, especially in young children. We present the case of a 2-year-old boy who presented with a 2-month history of nasal obstruction, snoring, and epistaxis followed by a recent dyspnea. Examination revealed a protruding tissue mass in the left nasal cavity. Computed tomography scan showed a homogenous soft-tissue mass in the left nasal cavity extending toward the ipsilateral orbit, infratemporal fossa, nasopharynx, as well as the ethmoid and maxillary sinuses. Magnetic resonance imaging revealed a homogenous infiltrating mass with a hypo-intense signal on T2-weighted images reaching the infratemporal fossa and oropharynx. Biopsy confirmed the diagnosis of BL. The patient was referred to the clinical hematology department and received complex chemotherapy. Following chemotherapy, imaging revealed significant regression of the mass. We performed a nasopharyngeal biopsy which confirmed the absence of any persistent disease. This case report highlights a rare case of an extensive sinonasal BL emphasizing the importance of a high level of suspicion to ensure an early diagnosis and treatment.
Introduction
Burkitt lymphoma (BL) is a highly aggressive B-cell non-Hodgkin lymphoma. It can present as three different variants, either sporadic, endemic, or immunodeficiency associated.1,2 Each of these variants has its own clinical and epidemiological features. BL primarily affects the abdominal area. However, it develops in the head and neck region in 10% of cases, mainly at level of the lymph nodes, followed by the facial bones such as the maxilla and the mandible.1,3 More rarely, a primary BL can affect the nasal cavity, nasopharynx, and paranasal sinuses. However, sporadic forms, affecting these localizations in young children are extremely rare. 4 They manifest with rhinological symptoms that are not specific to sinonasal BL, which can cause a delayed diagnosis. 2 We present an atypical case of sinonasal BL in a 2-year-old boy in whom the diagnosis was suspected based on computed tomography (CT) scan and magnetic resonance imaging (MRI) and was confirmed by histological examination.
Case Report
We report the case of the 2-year-old boy, without any medical record, who presented to our department with a 2-month history of rapidly evolving nasal obstruction. It was associated with snoring, oral breathing, and a few episodes of left nasal bleeding. These symptoms were followed by the appearance of a left nasal mass and a recent onset of dyspnea. Physical examination revealed a pinkish-white colored tissue mass, completely filling the nasal cavity, reaching the nasal vestibule, and causing a complete deviation of the nasal septum toward the right side. No cervical lymphadenopathy was observed. Facial CT scan revealed a homogenous soft-tissue mass, completely filling the nasopharynx. It extended anteriorly toward both nasal cavities predominantly on the left side. It also infiltrated the sphenopalatine foramen, causing its enlargement and reached the left infratemporal fossa with an enlargement of the pterygopalatine fossa and lateral deviation of the masseter muscle. The mass extended to the ethmoid cells superiorly, damaging the lamina papyracea, reaching the orbit, and compressing the medial rectus muscle. We also noted an extension at the level of the superior orbital fissure and bony destruction of the pterygoid bone. No enlarged lymph nodes or intracranial extension were noted. The mass presented a moderate homogenous enhancement after contrast injection (Figure 1).
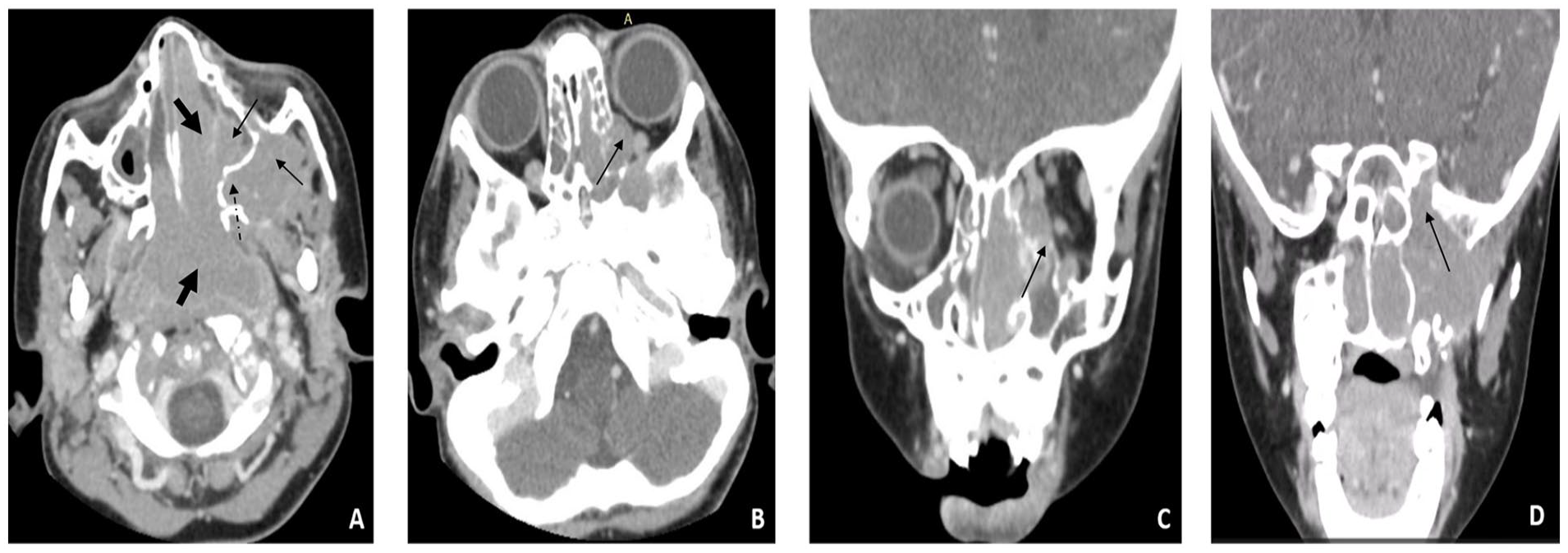
(A) Homogenous tissue mass centered at the level of the nasopharynx and both nasal cavities showing a moderate homogenous contrast enhancement (thick black arrows). It reaches the left maxillary sinus and infratemporal fossa (thin black arrows). Infiltration and enlargement of the left pterygopalatine fossa (dashed black arrow). (B, C) The mass infiltrates the ethmoid cells superiorly with a lysis of the left lamina papyracea (black arrow) and an intra-orbital extension. (D) Infiltration of the superior orbital fissure (thin black arrow).
MRI showed a homogenous mass with a hypo-intense signal on T2-weighted slides (Figure 2). It was localized at the level of the nasopharynx, with an extension toward both nasal cavities, as well as the left infratemporal fossa. Inferiorly, it massively reached the oropharynx.
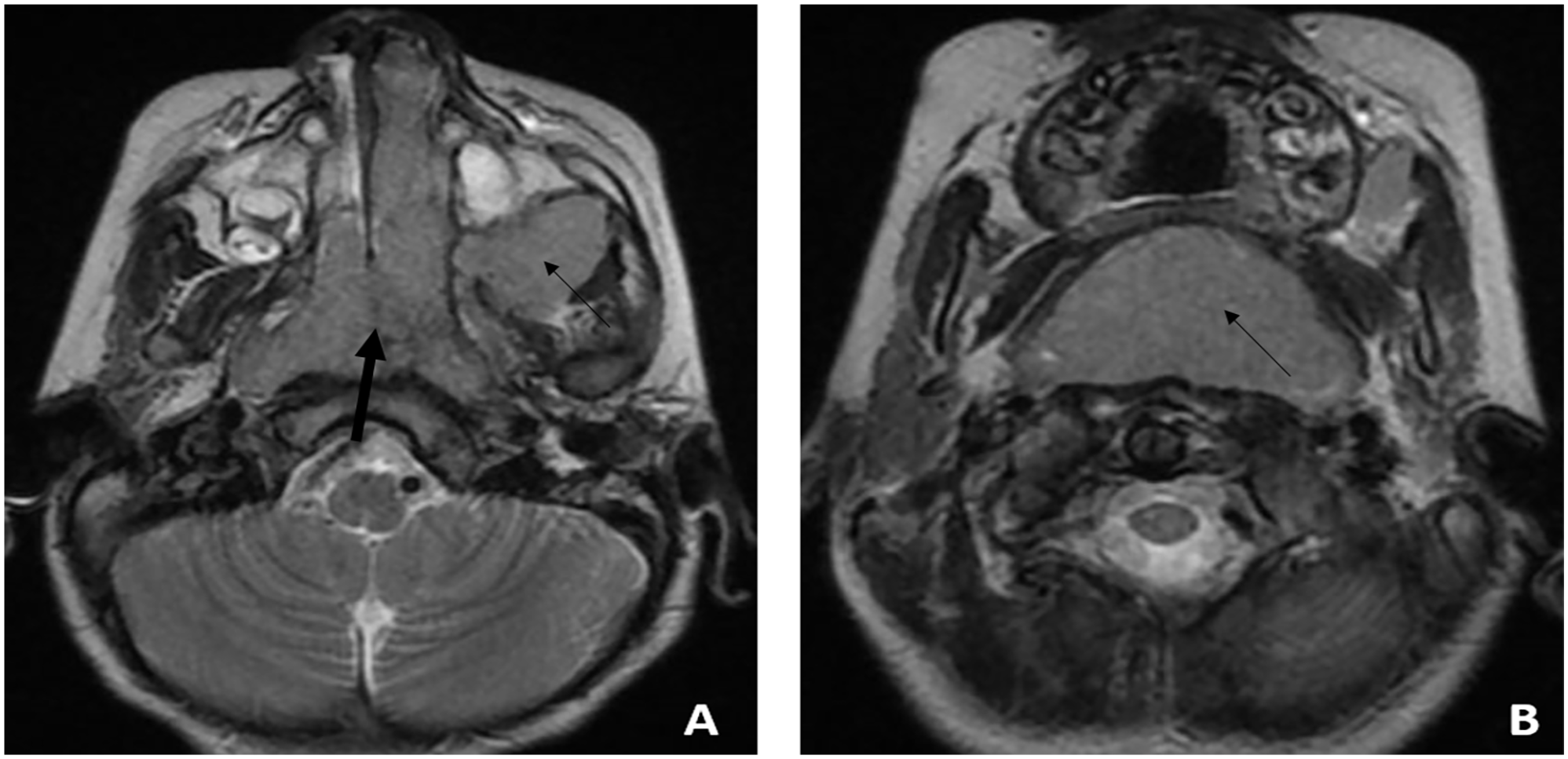
Magnetic resonance imaging, T2-weighted axial slides. (A) Homogenous mass with a hypo-intense signal localized at the nasopharynx, filling both nasal cavities mainly at the left side (thick black arrow) extended toward the infratemporal fossa (thin black arrow) (B) the mass reaches the oropharynx inferiorly (thin black arrow).
Based on the imaging findings, the dyspnea was attributed to the oropharyngeal extension. We then performed a biopsy of the left nasal cavity mass. The histopathological examination showed a diffuse proliferation of monomorphic cells with basophilic cytoplasm and round nuclei, finely dispersed chromatin, and multiple mitotic figures. The proliferation was sprinkled with multiple tangible body macrophages showing the “starry-sky” aspect. The tumorous cells also showed crush images. The immunohistochemical study revealed that tumor cells expressed CD10 and CD20. The proliferative index was determined by Ki67 nuclear staining and measured 100% (Figure 3). These histopathological findings confirmed the diagnosis of BL.
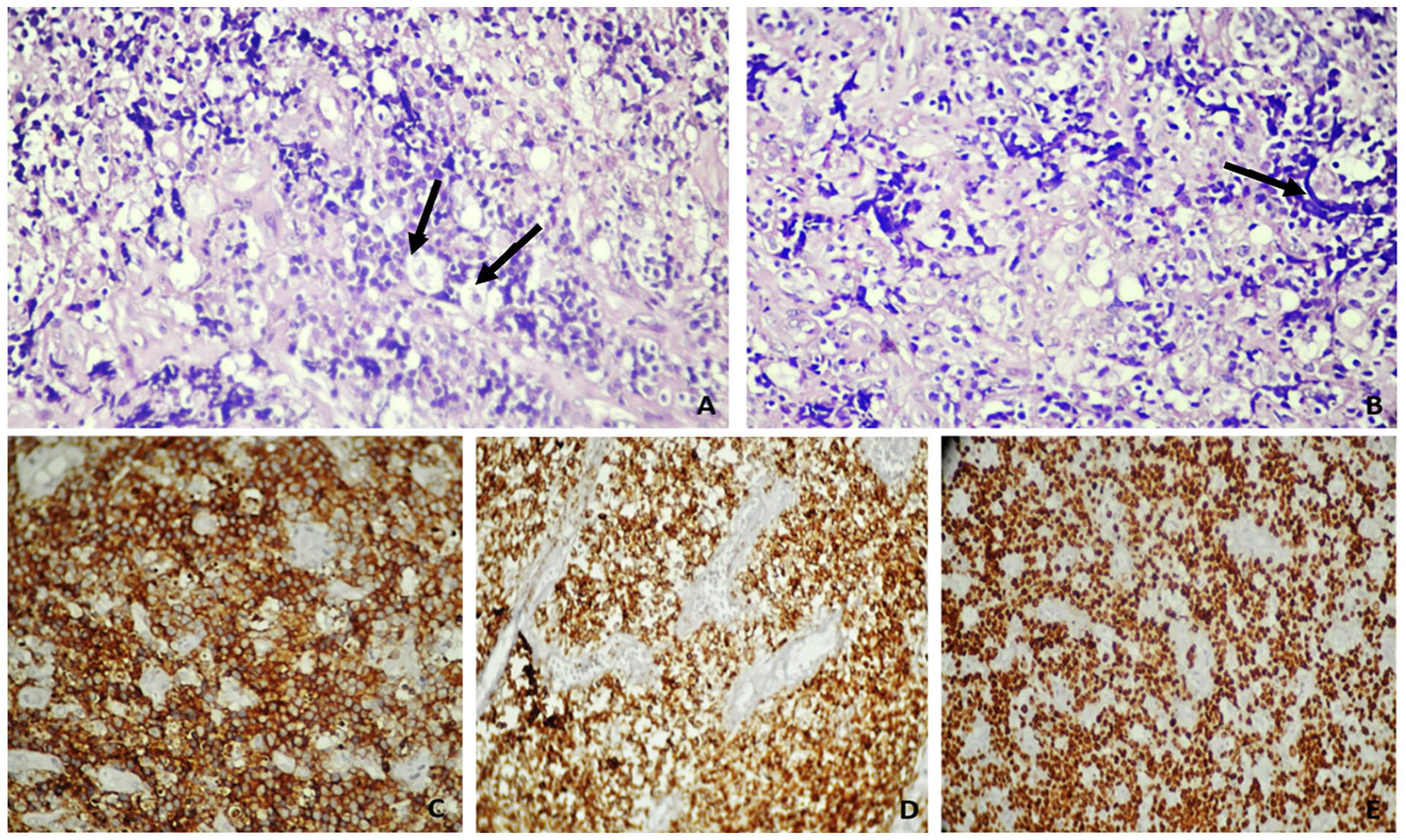
Histopathological examination showing cellular proliferation of round blast cells sprinkled with multiple tangible body macrophages (black arrows) ((A) HE × 400). Massive lymphomatous cell proliferation with crushing artifact images (black arrow) ((B) HE × 400). Immunohistochemical study: the tumor cells express CD10 ((C) HE × 200) and CD10 ((D) HE × 200). The Ki67 proliferation index is approximately 100% ((E) HE × 200).
The child was referred to the clinical hematology department. Thoracic abdominal and pelvic CT scans did not show any distant extension of the disease. Bone marrow biopsy and cerebrospinal fluid examination did not reveal tumorous proliferation. Human immunodeficiency virus (HIV) serology was negative. The disease was classified as stage II based on the Jude staging system. The patient was placed under a complex chemotherapy based on a COP cycle (cyclophosphamide, prednisone, and vincristine) followed by 2 cycles of COPADM (Cyclophosphamide, Vincristine, Prednisone, Adriamycin, Methotrexate) and 1 cycle of CYM (Cytarabine and Methotrexate).
Following treatment, we noted a total regression of nasal obstruction, snoring, and dyspnea. CT scan following the first CYM cycle showed a partial response of 78% based on the Cheson criteria with significant regression of the tumorous size, as well as a regression of the choanal, infratemporal fossa, prevertebral and intra-orbital extensions alongside with a total disappearance of the oropharyngeal extension. MRI revealed only a thickening of the posterior nasopharyngeal wall, which had a hypo-intense and an intermediate signal on T1- and T2-weighted images, respectively with a diffuse enhancement following gadolinium injection without any endocranial, choanal, bony, and deep-neck spaces extensions. PET (Positron Emission Tomography) scan showed an intense nasopharyngeal hypermetabolism (Figure 4). We then performed a nasopharyngeal biopsy following chemotherapy; it did not show any sign of a persistent disease.
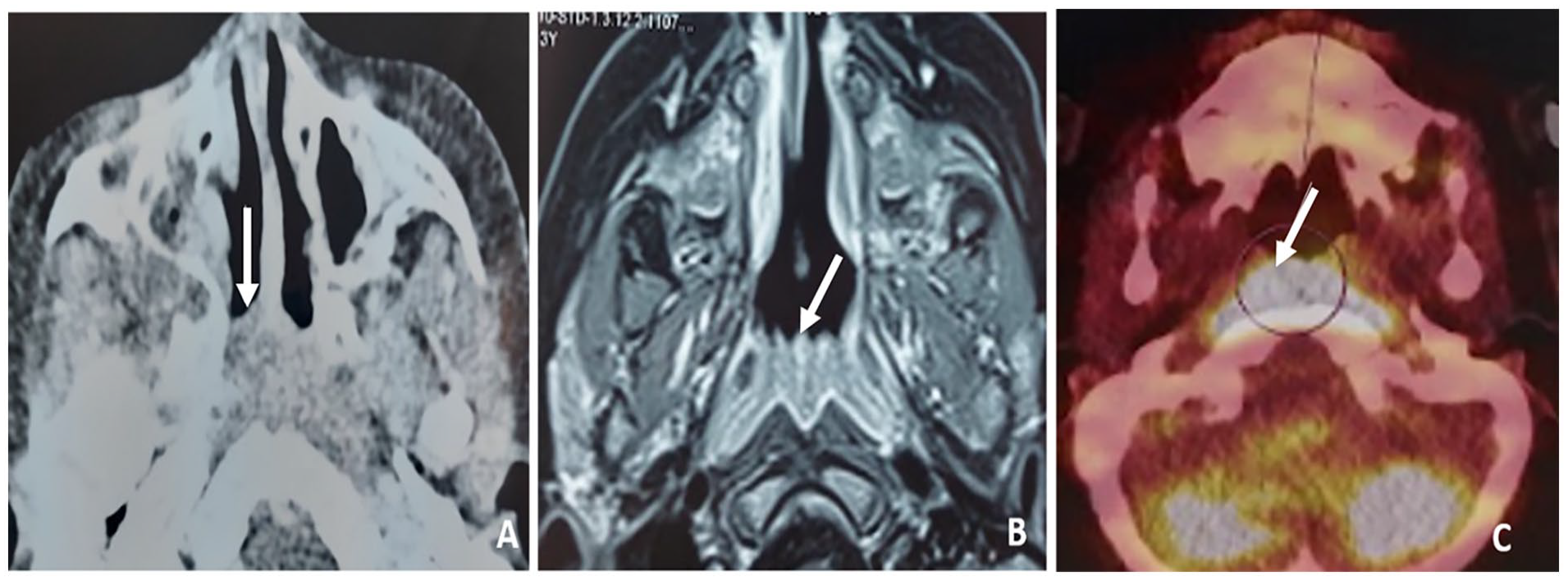
(A) Contrast-enhanced computed tomography scan, axial slide, regression of the tumorous mass that measures 41 × 22 mm with a minimal choanal extension (white arrow) (B) MRI, axial slide: thickening of the posterior nasopharyngeal wall with a homogenous enhancement following gadolinium injection (white arrow) without a choanal, prevertebral, and deep-neck spaces extension. (C) PET scan axial slide, intense nasopharyngeal hypermetabolism (white arrow) with a maximal SUV (Standard Uptake Valeu) index of 11.33.
Discussion
BL is a highly aggressive B-cell non-Hodgkin lymphoma that presents the most common head and neck malignancy in children.1,2 BL of the head and neck (BLHN) occurs in 10% of cases and is predominantly localized at the level of cervical lymph nodes. It can also affect the oropharynx and nasopharynx, while the paranasal sinuses are rarely affected3,5 The maxillary sinus is reported as the most commonly affected sinus while the sphenoid and ethmoid sinuses were less commonly involved.6,7
BL presents as endemic, sporadic, or immunodeficiency associated forms. The endemic form develops in Equatorial Africa and affects younger children; it is mainly localized in the jaw, facial bones, and adjacent soft tissues.2,3,8,9 The reported incidence in the maxilla and mandible is 58%.2,10 The immunodeficiency associated form commonly occurs in association with HIV or following an organ transplant. 3
On the other hand, sporadic forms most commonly affect the abdominal region and the bone marrow. However, sporadic forms of BLHN are a rare occurrence, mainly involving the Waldeyer ring and lymph nodes.8,11,12 This variant affects patients at the age of 10, 40, and 70 years old, while its occurrence at the age of 2 years is very uncommon, with a reported incidence of 0.7 case per million.4,6,13 When sporadic BLHN involves the sinonasal sinuses, it mainly affects children between 6 and 12 years old.3,14 -16 Here, we report a rare case of a sporadic sinonasal BL witnessed in a 2-year-old boy. Sporadic forms occurring at the level of sinonasal cavities in this age group have seldom been reported and were limited in the literature to case reports.4,6 A few cases of sinonasal BL associated with HIV were also reported, but they affect adults.10,17,18
Manifestations of BLHN are variable and depend on the site of involvement and the extension toward the adjacent structures. Reported symptoms in endemic forms included cervical lymphadenopathy, swelling of the affected region such as jaw swelling or facial mass, as well as proptosis, teeth mobility, paresthesia, and pain. 1,11,19,20 When the Waldayer ring is involved, symptoms rather include dysphagia, dyspnea, wheezing, and even airway obstruction. 11 Clinical manifestations of BL in children can also include systemic signs such as fever, weight loss, and headache.2,21 On the other hand, BL of nasal cavities and paranasal sinuses manifest with nonspecific rhinological symptoms including nasal obstruction, sleep-disordered breathing, nasal congestion, swelling, headaches, rhinorrhea, epistaxis, nasal voice as well as facial, cheek, and nasal swelling. Otalgia and hearing loss have also been reported.2,3,7,22 An acute airway obstruction can also be observed in the case of a locally advanced rhinological BL.2,3 Our patient mainly presented with rhinological symptoms in association to dyspnea that was attributed to the massive oropharyngeal extension.
A rapid aggravation of symptoms can be witnessed due to the aggressive nature of the tumor and its rapid expansion time that can even reach 24 to 48 hours.5,16,23 However, the duration of symptoms’ evolution in rhinological forms remains highly variable between a few weeks and a few months.3,6,10,22 In our patient, rhinological symptoms evolved rapidly for two months before confirming the diagnosis.
However, due to the rarity of this malignant entity in comparison to sinonasal infectious diseases, the diagnosis of sinonasal BL can be delayed. In fact, rhinological symptoms in sinonasal BL remain not specific to this entity and can delay the diagnosis, especially since BLHN rather mainly manifests with cervical lymphadenopathy. Besides, these signs are common in the pediatric population. Thus, rhinological forms can be misleading as they mimic acute and chronic rhinosinusitis. 2 Previously reported cases also manifested initially as viral and bacterial upper respiratory infections that were irresponsive to treatment.3,10 Other cases rather manifested with an otalgia and were treated as otitis media with effusion.2,22 Physical examination findings can also be misleading as sinonasal BL typically presents as a polypoid mass resembling polypoid sinusitis and other tumorous conditions. 5
However, though the clinical presentation is not specific, associated signs must raise the clinical suspicion of possible BL; these signs include: neurological signs, facial swelling, prolonged fever, visual signs as well as the absence of regression of rhinological symptoms under adequate treatment.2,6 BL should also be considered as a differential diagnosis of nasopharyngeal tumors. 17
The diagnosis of sinonasal BL is based on a biopsy of the suspected mass with histopathological examination which typically reveals monomorphic intermediate size B-cells with round nuclei, basophilic cytoplasm, multiple small nucleoli, finely dispersed chromatin, diffuse sheets, and numerous mitotic figures with a characteristic starry-sky pattern.1,5,24 At immunohistopathology, BL expresses CD10, CD19, CD20, CD22, CD74, and CD79a.5,15 Bone marrow and cerebrospinal fluid examination as well as the dosage of lactate dehydrogenase level and Epstein-Barr virus serology may also be required.5,25 Other authors recommend HIV testing in all BL cases. 26
Imaging, based on CT and MRI, helps to determine the extension toward adjacent structures. CT scan shows soft-tissue density mass with or without a bony erosion; it is superior to MRI in diagnosing bone destruction.18,25,26 MRI is better at evaluating soft tissue and bone marrow extensions. It shows a homogenous mass with a moderate signal on T1-weighted images and an intermediate or hypo-intense signal on T2-weighted images due to the decreased cellularity. These lesions also show restricted diffusion on diffusion-weighted images.1,11,12,27 At the level of soft tissues, the mass demonstrates homogenous enhancement without central necrosis and tends to infiltrate surrounding structures without their destruction, especially in sporadic forms. In contrast, endemic variants are characterized by bony destruction and osteolytic lesions of the maxilla-facial bones with an enlargement and invasion of the adjacent structures.11,12 In our patient, BL also presented as an infiltrating homogenous mass with a hypo-intense signal on T2-weighted images suggesting sinonasal lymphoma. However, CT scan and MRI are not specific to this entity, and their findings can mimic other aggressive diseases of the sinonasal cavities, either infectious or tumorous. Abdominal and chest CT scans are required to evaluate distant extension. 5
BLHN is highly sensitive to chemotherapy, and its management is based on complex chemotherapy that includes cyclophosphamide, vincristine, methotrexate, and prednisone. 7 Our patient was also placed under complex chemotherapy resulting in the regression of the mass on post-therapeutic imaging with the regression of histological signs in favor of BL. On the other hand, radiotherapy and surgery are not recommended and are reported to increase morbidity without increasing the survival rate. 7 Surgery is also not indicated, even in localized forms. Its use is restricted to complications requiring prompt intervention such as bowl obstruction.12,28
Prognosis of BLHN is generally poor with a survival rate of 50%. The association with HIV has been reported as a factor associated with a worse prognosis.21,29 Prognosis also depends on the timing of the diagnosis and chemotherapy, as well as the stage of the disease at presentation.5,9 Patients who receive an early treatment were associated with better outcomes in comparison to the delayed treatment which can cause BL to reach other distant organs.2,16 Other factors associated with a worse prognosis included advanced age, elevated lactate dehydrogenase levels, bulky mass, advanced stage as well as bone marrow, central nervous system, and mediastinal involvement. Children are reported to have a better prognosis in comparison to adults.4 -6,12
Survival rates were variable in the literature. They can reach 90% in localized forms detected precociously.4,22 The duration of the remission period remains variable but can reach 18 months with better survival rates in children. 15
Conclusion
BL rarely develops within paranasal sinuses and the nasal cavity, especially in young children. Rhinological manifestations as well as the clinical presentation are not specific to this entity; they can mimic other infectious and tumorous conditions which can mislead the diagnosis and delay treatment. A high clinical suspicion is required to avoid missing the diagnosis. The diagnosis can be suspected with imaging based on CT scan and MRI, but its confirmation is based on histopathological examination. Management is based on complex chemotherapy. Prognosis is highly related to the delay in the diagnosis and treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series since we anonymously reported clinical and imaging information concerning our patient’s case. A written informed consent was obtained from our patient’s legal parents for his anonymized information to be published in this article.
Informed Consent
Written informed consent was obtained from the parents of the patient for his anonymized information to be published in this article.