
Abstract
Radiofrequency ablation (RFA) provides a relatively safe and noninvasive option for treating benign thyroid nodules and thyroid cancer that is cosmetically superior to surgery. Following a loss of consciousness 1 h after thyroid RFA, a 56-year-old patient was transferred to the emergency room. Despite undergoing coronary angiography due to 3 cardiac arrests, the results were normal. Although brain, chest, and abdominal computed tomography scans were performed, the emergency physician failed to detect any hematoma formation. Despite the use of mechanical ventilation and extracorporeal membrane oxygenation, the patient exhibited persistent hypoventilation. It was later discovered that an aggravated massive hemorrhage had occurred, due to which inferior thyroid artery embolization and surgical hematoma evacuation were performed. Unfortunately, prolonged brain hypoperfusion resulting from airway compromise and common carotid artery occlusion resulted in brain death and, ultimately, the patient’s demise. In conclusion, massive hemorrhages caused by RFA require immediate diagnosis and hemostasis.
Introduction
Radiofrequency ablation (RFA) has recently gained popularity in the recent years as a promising alternative to surgery for treating benign thyroid nodules and thyroid cancers. RFA is relatively safe, with a low risk of complications, as evidenced by 2 systematic review studies reporting incidence rates of 2.38%-3.8% for complications and 1.35%-1.5% for major complications.1,2 Hemorrhage and hematoma formation occurred in only 0.0%-17% of cases and were typically minor complications that resolved with brief digital compression or required no special treatment. 3 However, a case of airway compromise caused by massive hemorrhage have been reported even with fine needle aspiration, 4 highlighting the need for caution with RFA. Herein, we present a case of delayed diagnosis of massive hemorrhage by RFA in a patient who was transferred to our emergency room 1 h after thyroid RFA treatment at another hospital, ultimately resulting in the patient’s death.
Case Report
On the same day as her thyroid nodule RFA treatment at another hospital, a 56-year-old patient complained of chest discomfort and shoulder pain 1 h after the procedure and subsequently experienced decreased consciousness while being monitored. The patient had a history of coronary artery disease, diabetes, and hyperlipidemia and was taking medications such as clopidogrel. During the transfer by an emergency vehicle, the patient was in a coma but had a heart rate of 106 beats per minute and an oxygen saturation (SpO2) of 98%, indicating that cardiac arrest cardiopulmonary resuscitation (CPR) was not necessary. Upon arrival at our emergency room, the patient was mentally drowsy but responsive, with a systolic blood pressure of 82 mmHg and a diastolic blood pressure of 56 mmHg, as well as a SpO2 of 98%. Due to her decreased consciousness, it was not possible to inquire about other symptoms, and no specific findings, such as cervical swelling, were observed during the physical examination. One hour after visiting the emergency room, the patient experienced sudden cardiac arrest without a palpable pulse. CPR was performed for 6 min along with oral intubation, which resulted in the recovery of spontaneous circulation. Electrocardiography did not rule out anterior cardiac infarction; therefore, the patient underwent coronary angiography; however, no findings suggestive of myocardial infarction were observed. Brain and abdominal computed tomography (CT) scans were normal, while chest CT showed active bleeding filling the retropharyngeal space at the level of the sixth cervical spine and the formation of a large hematoma pressing against the posterior wall of the left main bronchus (Figure 1A). However, this critical finding was missed by the emergency physician, and the patient was misdiagnosed with cardiac arrest of an unknown cause despite twice regaining spontaneous circulation with CPR 6 h after her initial visit to the emergency room. Despite being admitted to the intensive care unit 9 h after visiting the emergency room and undergoing extracorporeal membrane oxygenation cannulation, the patient showed persistent hypoventilation. A chest CT was performed 21 h later when cervical edema was confirmed by physical examination, and a large hematoma extending to the trachea, which compressed the airway, was belatedly discovered (Figure 1B). The otorhinolaryngologist was informed of this only after the CT scan. At this point, the possibility of massive hemorrhage due to RFA was first raised. Catheter angiography was performed 24 h after visiting the emergency room, and contrast extravasation (Figure 2A) was observed in the left inferior thyroid artery. Embolization was performed using a glue and lipiodol mixture. However, occlusion by a large hematoma resulted in no flow to the right common carotid artery (Figure 2B). Immediately following a neck CT, the patient’s left thyroid gland was found to be disrupted, with a large hematoma reaching the C6-T2 level (Figure 1C). Hypoxic-ischemic brain injury to the right was also confirmed. The patient was transferred to the operating room for hematoma evacuation at 25 h after visiting the emergency room. A large hematoma extending from the carina to the nasopharynx was confirmed in the operating room. A left hemithyroidectomy was also performed due to continuous oozing caused by a capsule rupture of the left thyroid. However, the brain CT performed after surgery revealed further progression of hypoxic-ischemic brain injury, and brain death was determined. The patient passed away on the 19th day after visiting the emergency room.
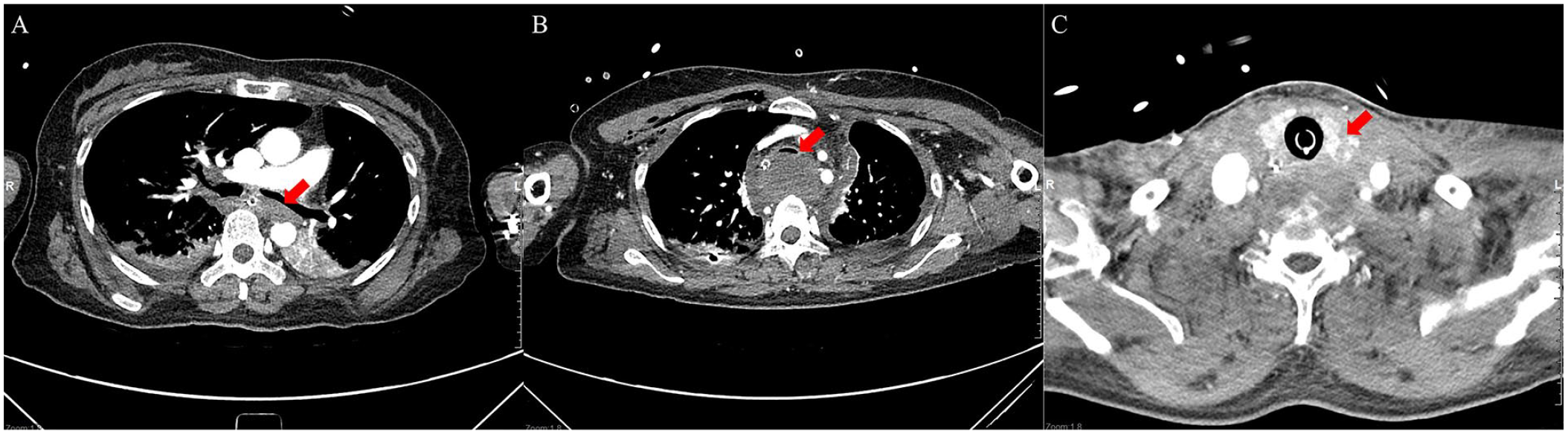
Contrast-enhanced computed tomography (CT) images. (A) The first chest CT scan. A hematoma pressing against the posterior wall of the left main bronchus can be observed (arrow). (B) The second chest CT scan which was performed 21 h after visiting the emergency room. The increased hematoma pressing against the posterior wall of the trachea can be observed (arrow). (C) Neck CT performed after catheter angiography and embolization. Disruption of the left thyroid gland can be observed (arrow).
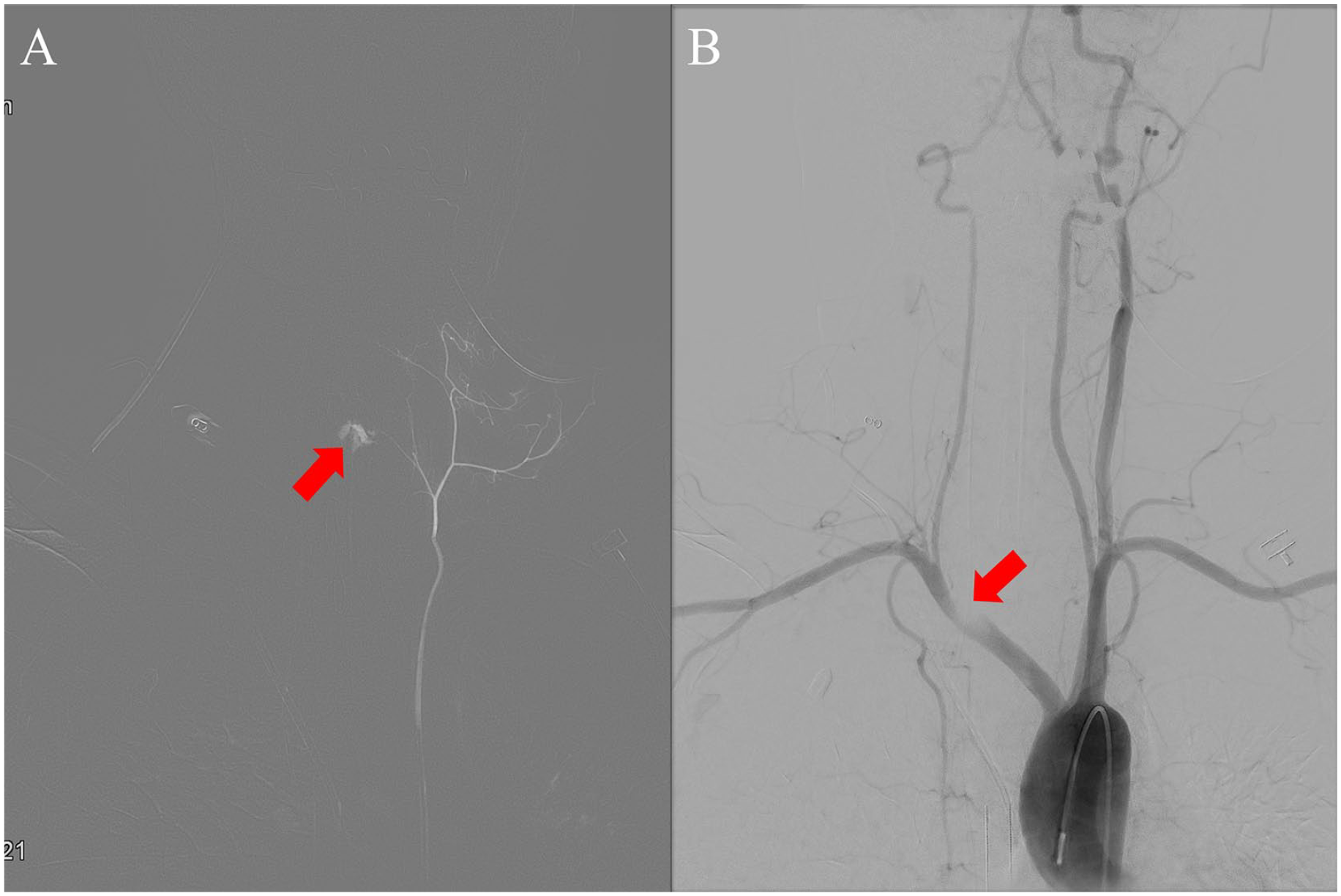
Catheter angiography images. (A) Extravasation of contrast is observed in the left inferior thyroid artery (arrow). (B) No flow of the right common carotid artery and narrowing of the innominate artery can be observed (arrow).
Discussion
As an ablative therapy for thyroid nodules, RFA is relatively safe, noninvasive, and cosmetically superior to open surgery. However, RFA is associated with known complications, including minor complications such as pain, skin burns, and hematoma, as well as major complications such as nerve damage, thyroid nodule rupture, and tracheal injury. 3 This case report presents the first documented instance of a patient dying from a massive hemorrhage caused by RFA performed on the thyroid nodule. A previous case report documented an injury to the inferior thyroid artery during RFA for secondary hyperparathyroidism, which was treated promptly due to the patient’s symptoms and physical examination findings of cervical swelling. 5 We highlight several important factors that contributed to the patient’s death in this case. First, the physician who performed the RFA did not inform the emergency physician of the procedure’s risks when the patient was transferred to the emergency room. The emergency physician was unaware of the RFA procedure and therefore did not consider the procedure’s significant history, neglecting the potential risks. Second, given the patient’s previous history of cardiovascular diseases such as diabetes, hyperlipidemia, and coronary artery disease, other potential causes were overlooked by focusing solely on these conditions. Third, due to the patient’s reduced consciousness, symptoms caused by the hematoma, including neck pain and shortness of breath, were not assessable. Fourth, the hematoma was diffused through the posterior area of the thyroid and mediastinum, and physical changes related to the hematoma, such as neck swelling and bruising, were not observable during the initial physical examination. Consequently, the possibility of RFA-induced disease was overlooked, and the massive hemorrhage and hematoma formation were missed despite a chest CT being performed. By the time the hematoma was identified, the patient had already experienced prolonged hypoventilation due to airway obstruction. Furthermore, prolonged hypoperfusion to the brain due to the occlusion of the right common carotid artery resulted in brain death, which ultimately led to the patient’s demise. Based on this case report, physicians must remember the risk of massive hemorrhage after an RFA procedure. Though symptom-related inquiries might be challenging due to the loss of consciousness, and initial physical examination might not show any specific findings, a CT scan should be performed immediately and carefully examined to detect the possibility of active bleeding. Rapid hemostasis through angiography or surgery should be performed. In conclusion, while RFA is generally considered a safe ablative therapy for thyroid nodules, it has the potential to cause significant harm, such as the formation of a large hematoma resulting from arterial injury, which can ultimately lead to airway compromise and carotid artery occlusion, and in turn, result in patient death. Therefore, immediate and prompt diagnosis and treatment are imperative.
Footnotes
Data Availability Statement
Fully anonymized data that contributed to this article are available on reasonable request only.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting this case.