
Abstract
Introduction:
Thyroid nodules are common entities, with 5% malignancy. Differentiated thyroid cancer represents 90% of thyroid malignancies, with papillary carcinoma being the most common. Management is generally surgical; among its complications are injury to the recurrent laryngeal and superior laryngeal nerve, causing hoarseness, postsurgical hypoparathyroidism, hypothyroidism, and pain. Other noninvasive percutaneous interventions of thermal ablation such as microwave, radiofrequency, or laser incur lower costs and could be an option for treatment.
Objective:
To determine the effectiveness and safety of thermal ablation in lesions suspected of thyroid cancer (Bethesda V and VI/T1aN0M0) compared to surgical treatment.
Methods:
Systematic review/meta-analysis of observational studies and clinical trials. Database search includes MEDLINE/PUBMED, Embase, Scopus, Scielo, and BVS/LILACS. Studies on patients over 18 years of age with lesions suspicious of thyroid cancer were included.
Results:
A total of 10 studies were obtained, with 2939 patients: 1468 subjected to thermal ablation and 1471 to surgery. Regarding effectiveness, no differences were found in local recurrence [relative risk (RR) 1.17 (95% CI 0.69-1.99)] and cervical lymph node metastasis [RR 0.76 (95% CI 0.43-1.36)]. Regarding safety, infection [RR 0.29 (95% CI 0.05-1.74)], hematoma [RR 0.57 (95% CI 0.17-1.94)], and transient hoarseness [RR 0.77 (95% CI 0.39-1.51)] were evaluated, without difference. However, permanent hoarseness had significant differences in favor of thermal ablation [RR 0.29 (95% CI 0.11-0.75)].
Conclusions:
Thermal ablation for the treatment of T1aN0M0 papillary thyroid carcinoma is equally effective when compared to surgical techniques and offers a better safety profile, particularly in permanent hoarseness.
Introduction
Thyroid nodules are common entities, being incidentally documented in up to 67%. 1 A total of 19.6% in carotid Doppler, 25% in computed tomography of the chest, 16% in the neck, 2% in positron emission tomography with fluorodeoxyglucose, and 10% in nuclear magnetic resonance. 2
Approximately 5% of all thyroid nodules are malignant. The incidence of differentiated thyroid cancer (DTC) is increasing. In Europe, the incidence is between 3 and 9 cases per 100,000 person-years. 3 In Colombia, thyroid cancer is second in the classification of neoplasms and in cities such as Bucaramanga, an incidence of 9.7 per 100,000 women was estimated between 2003 and 2007. From 2008 to 2012, it increased to 14.5, representing an increase in 49.5%. 4 Despite an increase in incidence, mortality remains low, with around 0.5 and 0.7 deaths per 100,000 person-years for men and women, respectively. Metastases extend mortality by up to 10%. 3
DTC represents 90% of all thyroid malignancies. Papillary thyroid carcinoma (PTC) is the most common type of thyroid cancer, accounting for 90% of DTCs. 5 PTC generally follows an indolent course and has a high survival rate.5,6
Pathology study by fine-needle aspiration (FNA) is required in lesions with high suspicion in ultrasound to determine whether cancer is present. Bethesda V and VI lesions present a cancer risk of 70% and 99%, respectively, and generally require surgical management. Total thyroidectomy or hemithyroidectomy with or without central dissection is the most frequent surgical option.1,2
Among the risks of surgical interventions are lesions of the recurrent laryngeal and superior laryngeal nerves, and the rates of temporary and permanent weakness of the vocal cords reaching 10% and 2%, respectively, reaching a significant compromise of phonation (hoarseness). In addition, the proximity of the thyroid gland to the parathyroid glands increases the risk of postsurgical hypoparathyroidism that can lead to severe hypocalcemia, with temporary involvement in 32.8% and permanent involvement in 12.5%. Other complications associated with these interventions are hypothyroidism and postoperative pain.7,8
The 2015 American Thyroid Association recommends active surveillance for patients with low-risk PTC, with specific patient, tumor, and environmental characteristics (central location of the tumor, the absence of nodes suspicious for malignancy or distant metastases, the absence of a personal or family history of high risk of progression, ideally individuals over 60 years of age, and in those with the availability of medical follow-up). However, it is also associated with certain problems such as tumor enlargement, local recurrence, and lymph node metastasis or distant metastasis. 9 Some patients are not satisfied with active surveillance, without receiving any intervention, given the probability of cancer.
There are noninvasive percutaneous interventions, guided by ultrasound images and the use of local anesthesia, which require the use of electrodes that transmit heat (between 60 and 100°C) to cause necrosis and fibrosis of thyroid tissue. 7 These methods constitute a therapeutic alternative in patients with benign thyroid nodules with associated symptoms, when there is a contraindication for surgical treatment or when the patient does not want this type of intervention, presenting a suitable therapeutic response, predominantly in nonfunctioning nodules, with minor costs, greater safety, and with better aesthetic results.8,10
Available percutaneous procedures are percutaneous ethanol injection and thermal ablation. The latter is divided into microwave ablation (MA), radiofrequency ablation (RFA), and laser ablation (LA). For its part, ethanol injection is the alternative of choice in cystic nodules, with an effectiveness rate of 85.6%, 2 but it is not recommended in the management of CDT. 3
Percutaneous interventions may also have a place in the treatment of suspicious Bethesda V or VI nodules. Papillary thyroid microcarcinoma has been studied most.3,7,8,10 Studies show that resolution and regression of the tumor lesion after 18 to 30 months of follow-up, depending on the technique used, 76.2%, 62.9%, and 57.3% after RFA, MA, and LA treatments, respectively, 8 with 99.3% reduction in lesion size by radiofrequency, microwave 95.3%, and laser 88.6%, without the evidence of lymph node metastases. 11 There are even reports of interventions in metastatic lymph nodes with an adequate response. Unfortunately, for other undifferentiated forms, these interventions have not been as successful, so surgery is still the main treatment. 7
It is important to have therapeutic alternatives for the treatment of malignant thyroid nodules instead of surgery to avoid complications associated with surgical management, cost reduction, and achievement of better aesthetic results so that the patient can make his or her preferred choice. For this reason, the available evidence will be analyzed through a systematic review and meta-analysis that evaluates the degree of safety and effectiveness of these percutaneous interventions compared to surgical ones in patients with Bethesda V or VI nodules.
Methods
Methodology: Systematic review of the literature and meta-analysis.
Criteria for including studies in the review:
Types of studies:
- Inclusion studies: clinical trials and observational studies.
- Exclusion studies: cluster, quasi-experimental or crossover clinical trials, case–control studies, cross-sectional studies.
Types of participants:
Studies involving patients older than 18 years with lesions suspicious of thyroid cancer (Bethesda V and VI—T1aN0M0) were included. T1a: ≤1 cm.
Excluded patients:
- Pregnant patients
- Severe pulmonary, cardiac, or renal pathology
- Other malignant pathology
Types of interventions:
Studies with any type of thermal ablation techniques (microwave, radiofrequency, or LA) compared to surgical treatment were included.
Types of outcomes:
The effectiveness and safety of thermal ablation techniques versus surgery were evaluated as the main outcomes. Regarding the former, local recurrence and the presence of cervical lymph node metastasis were evaluated. Regarding the second, transient and permanent hoarseness, infection, and the presence of hematoma were included.
Local recurrence is defined as the presence of tumor lesions at the intervention site (thermal ablation), in the thyroid intervention site (surgery), or in the thyroid lobe contralateral to the treated lesion. Cervical lymph node metastasis represents the presence of involvement by thyroid CDT in cervical lymph nodes ipsilateral or contralateral to the operated lesion after the intervention is verified by FNA or excisional biopsy.
Transient hoarseness is defined as the presence of alterations in the voice after carrying out the procedures, lasting less than 6 months. Permanent hoarseness occurs when the symptoms exceed 6 months. Infection and the presence of hematoma will be evaluated dichotomously, meaning whether or not the patients presented this complication after the intervention.
Search strategy:
To answer the research question, we used a combination of controlled terms (MeSH) and free terms (to consider spelling variants, synonyms, acronyms, and truncations) and Boolean operators (OR, AND).
The following words were searched under the key terms: “microwave ablation” OR “laser ablation” OR “radioablation” OR “thermal ablation” AND “thyroid cancer” OR “thyroid carcinoma.”
The literature search was between january 2000 and february 2023. It was limited to studies in English and Spanish.
Specifically, we searched the following databases:
MEDLINE/PUBMED
Embase, embase.com platform
Scopus
Scielo
BVS/LILACS
Study selection: Two authors independently selected studies, initially by title and abstract and then by full text. In case of disagreement, a third author decided to include or exclude the studies.
The information extracted from each study is as follows:
- Author
- Year of publication
- Type of study
- Inclusion criteria
- Exclusion criteria
- Name of the intervention (ablation technique)
- Size of the intervention
- Comparator size
- Tracking time
- Local recurrence, cervical metastasis, bleeding, infection, hypoparathyroidism, hoarseness, and hypothyroidism.
Assessment of risk of bias:
Two authors assessed the risk of bias for each included study using the Cochrane Collaboration tool for nonrandomized studies ROBINS I, which assesses the following domains:
Confounding bias
Bias in the selection of study participants
Bias in the classification of interventions
Bias due to deviations from planned interventions
Bias due to missing data
Bias in the measurement of results
Bias in the selection of the reported outcome
Subsequently, the RevMan 5.4 software is used for the respective bias risk graphs, Figure 2.
Analysis Plan
For the preparation of the analysis, the RevMan 5.4 software (a Cochrane collaboration tool) was used, through which the respective forest plots of dichotomous variables were plotted, using the analysis of RRs as a guide to establish the effects on the effectiveness and safety outcomes between thermal ablation and surgery.
Heterogeneity was assessed using the Chi2 test and the I2 statistic. Heterogeneity was considered with a Chi2 test with a P value less than .1. Regarding the I2 statistic, it was determined that 0% to 40% is not significant heterogeneity, 30% to 60% represents moderate heterogeneity, 50% to 90% significant heterogeneity, and 75% to 100% is considerable heterogeneity. In the cases in which low heterogeneity was found, the analysis was carried out using fixed effects and in the cases in which moderate or high heterogeneity was found, the analysis strategy was carried out using random effects (Cochrane collaboration guide).
Regarding the publication bias in the selected studies, the respective funnel plot of the variables was performed using RevMan 5.4, where the symmetry in the distribution of the organization of the interventions in the studies was observed.
Results
Systematic Literature Search
Through the systematic review, it was possible to identify 1382 articles. After eliminating the duplicates, 1301 remained, and of those 111 were selected by title, of which 96 were excluded because they mentioned other interventions, corresponded to benign pathologies or had a design that did not meet the inclusion criteria. After the above review, 14 studies were identified per abstract to be evaluated in full text, of which 4 were excluded, finally leaving 10 articles for qualitative synthesis and meta-analysis (Figure 1).
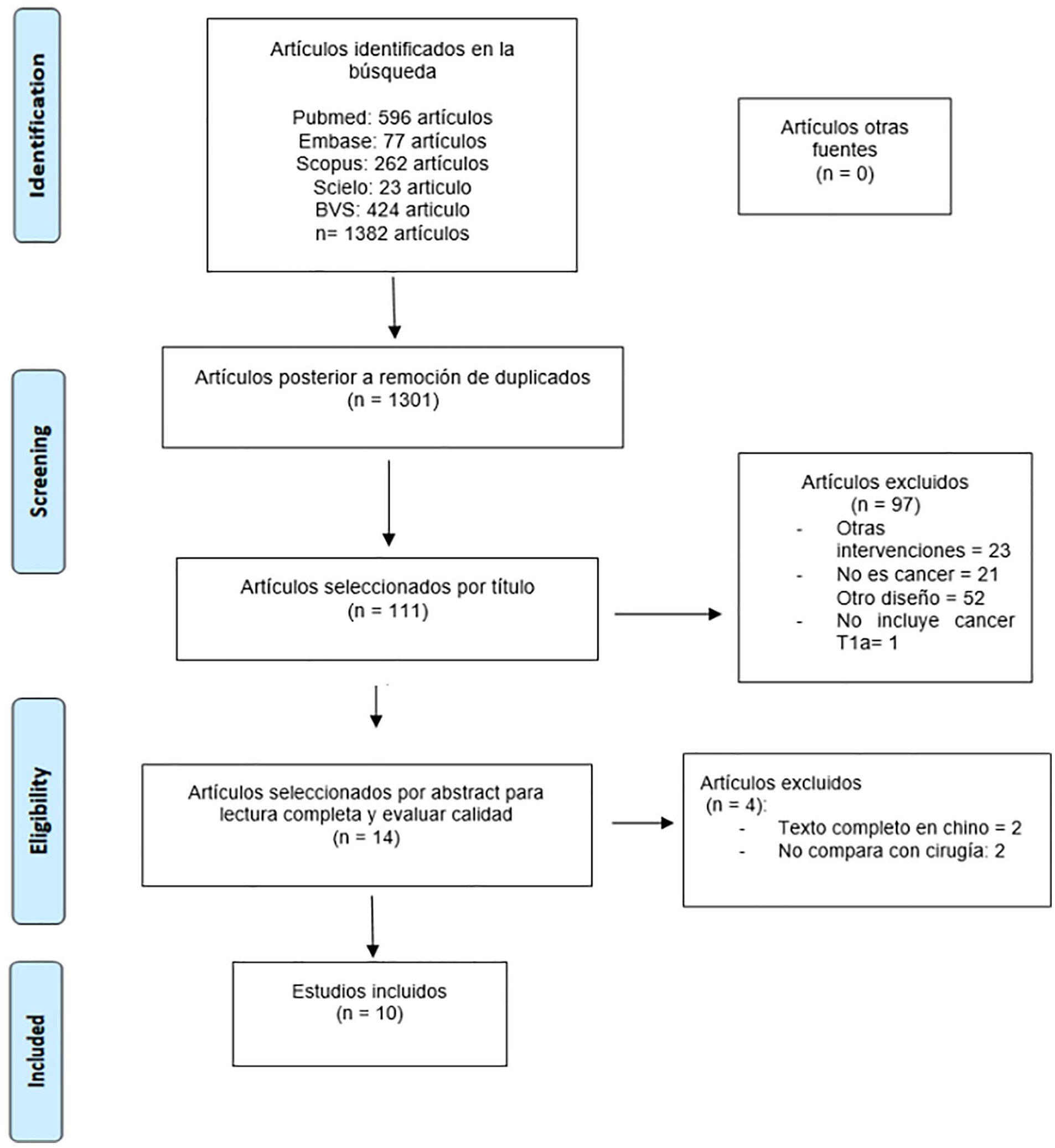
Flowchart Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA).
Study Characteristics and Quality Assessment
All studies showed a low risk of confusion bias in the classification of the interventions, measurement of results, and selection of the reported outcome.
Four studies showed unclear risk of selection of study participants,12-15 while the other 6 studies showed low risk. One study showed high risk due to lack of data, 15 other 5 studies showed unclear risk13,16-18 and the remaining 5 showed low risk (Figure 2).
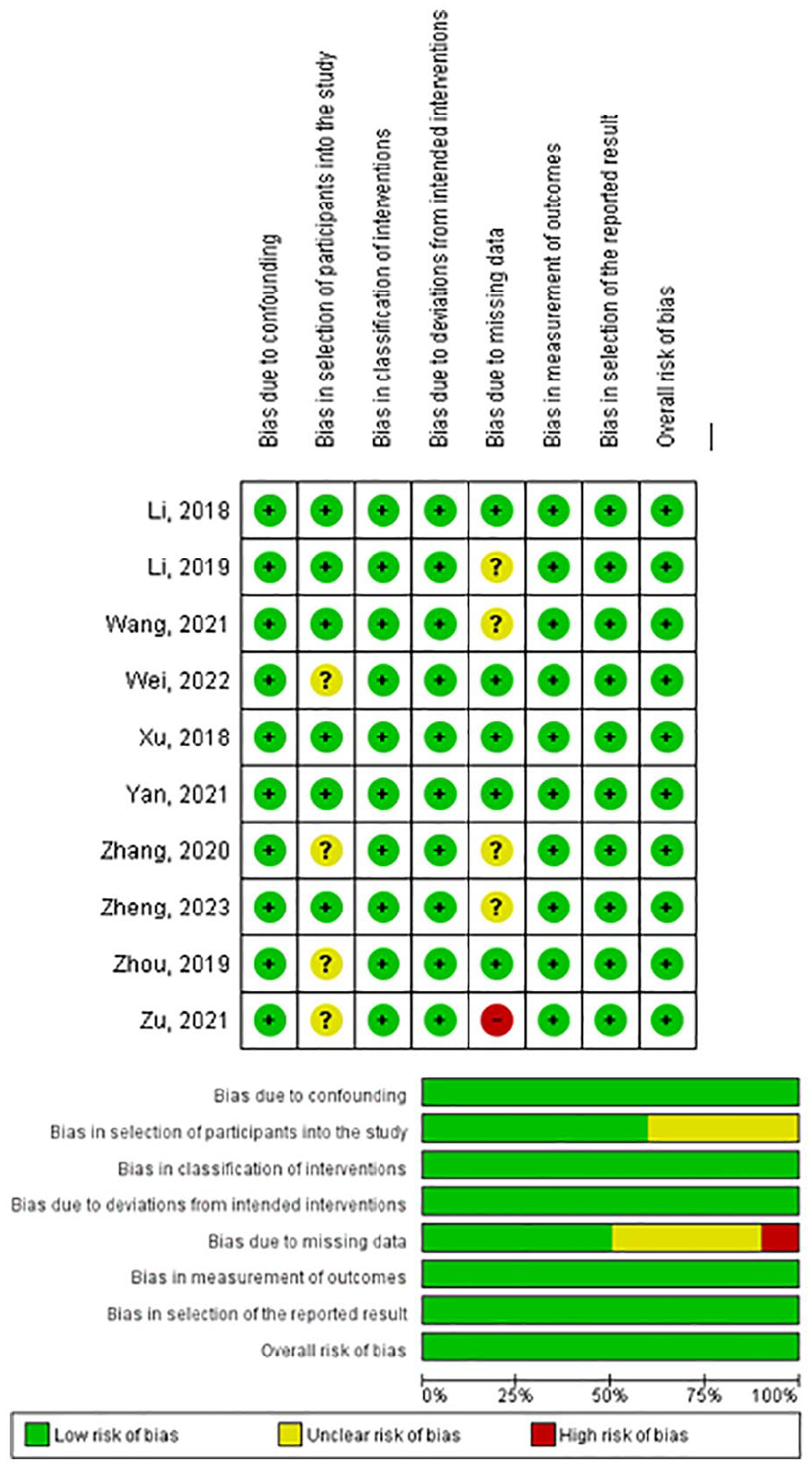
Risk of bias assessment.
Nine studies had an observational design, of which 8 were retrospective and 1 prospective, and the 10th study was a nonrandomized clinical trial.
Surgery or ablation was selected based on the patient’s general condition, wishes for intervention, or other reasons for all studies. Regarding the ablation method, 7 studies used microwaves,12,15-20 2 studies used radiofrequency,13,21 and 1 study used laser. 14
Clinical Features
Table 1 shows the detailed characteristics of the 10 studies and the type of ablation used. A total of 2939 patients were included: 1468 (49.9%) in the thermal ablation group and 1471 (50.1%) in the surgery group. Within the thermal ablation group, MA was performed in 1006 patients (68.5%), ARF in 426 patients (29%), and AL in 36 patients (2.5%).
Characteristics of the Included Studies.
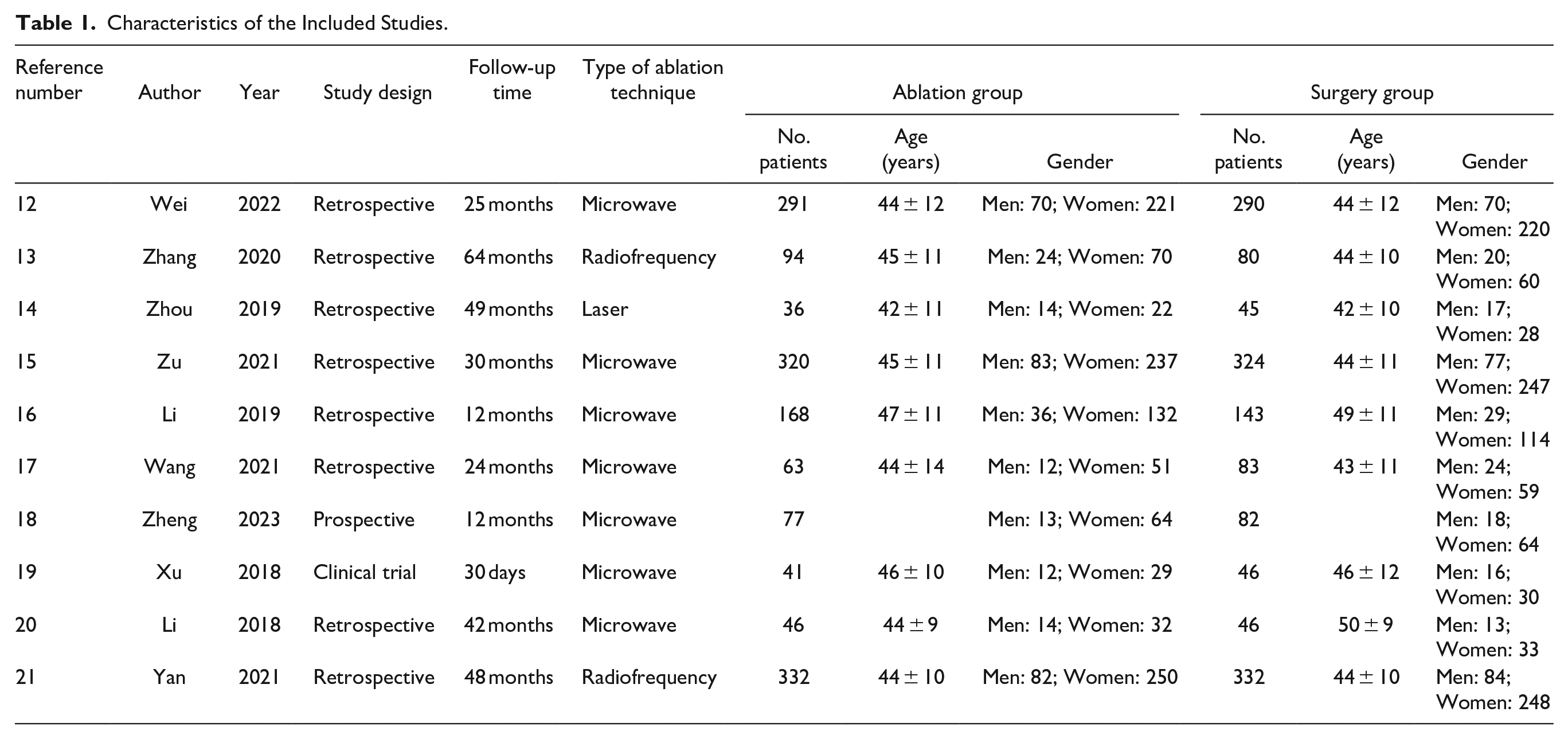
In the thermal ablation group, a higher proportion of women of 75.7% (1108) was found and their average age was 44 years. In the surgical group, there was also a predominance of women, representing 75% (1103) of patients with an average age of 45 years.
Criteria for treatment were similar in most studies, biopsy or cytology-confirmed CDT ≤ 1 cm, no contact with the thyroid capsule or extrathyroidal extension, and neither lymph node involvement nor distant metastases. Two studies included patients with PTC < 2 cm (12, 18), with classification T1a ≤ 1 cm and T1b > 1 cm. For this meta-analysis, we decided to include only T1a given the low number of patients in group T1b and that there is not enough evidence in this group for the use of thermal ablation techniques.
Nine of the studies included patients with solitary PTC, while 1 study did not report the number of tumors in the included patients. 19
In 1 study, they performed the thermal ablation procedure under general anesthesia. 19 The rest of the studies mention performing the procedure under local anesthesia, hydrodissection to separate vital tissues, and then performing the ablation. As a control of the procedure, an ultrasound with contrast was performed, injecting a bolus of 2.4 ml of ultrasonic contrast agent suspension to determine that the ablation was complete. If there was a residual enhancement, an additional ablation was performed during the same session of treatment.
In 5 studies, all patients in the surgical group underwent lobectomy with prophylactic ipsilateral central lymph node dissection.14,17,19
In a study of the 46 patients in the surgical group, 9 underwent total thyroidectomy and 37 lobectomy. They did not describe whether or not they underwent lymph node dissection. 20 The Lin Yan 2021 study describes performing lobectomy without prophylactic ipsilateral central lymphadenectomy. In another study, the patients in the surgical group were divided as follows: 6 underwent lobectomy with ipsilateral central node dissection, 45 underwent lobe and isthmus dissection with ipsilateral central node dissection, and 55 underwent total thyroidectomy with ipsilateral central node dissection. 18 In the Mingbo Zhang 2020 study, 58 patients underwent lobectomy (39 with ipsilateral central node dissection and 19 without node dissection) and 22 total thyroidectomy (14 with ipsilateral central node dissection and 8 without node dissection). In the study by Ying Wei 2022, 59 patients underwent total thyroidectomy, 211 lobectomy, and 20 subtotal thyroidectomy.
The average duration of hospitalization was greater for the surgical group, consisting of 5.64 days compared to 0.79 days in the ablation group.
Effectiveness
The effectiveness of the ablation procedures after their completion was verified with contrast-enhanced ultrasound in all the studies evaluated and long-term follow-up that included neck ultrasound to determine the presence of findings suggestive of local recurrence or lymph node metastasis that varied depending on the study. Four studies had a mean follow-up of less than or equal to 24 months, including 1 study that had a follow-up of 30 days; the remaining 6 were followed up for more than 24 months, see Table 1.
In the local recurrence variable, with a total of 1427 patients in the thermal ablation group and 1425 in the surgery group, encompassed in 9 studies, it was observed that there were no statistically significant differences, RR of 1.17 was shown (95% CI 0.69-1.99), with low heterogeneity (Chi2 = 2.59 with P value = .92, I2 = 0%). Regarding cervical lymph node metastases, when comparing the same groups of patients, no differences were found regarding the techniques of thermal ablation and surgery, finding an RR of 0.76 (95% CI 0.43-1.36), with low heterogeneity (Chi2 test = 0.73 and P value = 1.0, I2 = 0%).
Safety
The hoarseness variable was subclassified into transitory and permanent. In transient hoarseness, 9 studies were evaluated with 1427 patients in the ablation group and 1425 in the surgical group. It was found that there were no statistically significant differences, demonstrating a RR of 0.77 (95% CI 0.39-1.51) with moderate heterogeneity (Chi2 = 10.26 with P value = .11, I2 = 42%). For this reason, random-effects analysis was considered. In permanent hoarseness, 1468 ablation patients and 1471 surgery patients were evaluated in the 10 selected articles, finding statistically significant differences with a RR of 0.29 (95% CI 0.11-0.75) with low heterogeneity (Chi2 = 1.86 with P value = .97, I2 = 0%).
In infection and presence of hematoma, no statistically significant differences were found between the 2 evaluated techniques, presenting in the first an RR of 0.29 (95% CI 0.05-1.74) with low heterogeneity (Chi2 = 0.02 with P value = .99, I2 = 0%) when comparing 4 studies that included 445 patients undergoing ablation and 463 patients undergoing surgery. Regarding hematoma, other 4 studies with 693 ablation patients and 705 surgery patients found an RR of 0.57 (95% CI 0.17-1.94) with low heterogeneity (Chi2 = 0.52 with P value = .77, I2 = 0%).
Publication Bias Results
Ten studies were included, in which symmetry was observed in the funnel plots, demonstrating a low probability of publication bias.
Discussion
Thyroid cancer is second among the types of cancer in Colombia, 4 highlighting the need for different treatment approaches. The most frequently used technique is surgery, but TA exists as an alternative method for CDT T1a cases.21-26 For this reason, the decision was made to compare the effectiveness and safety of these techniques in patients older than 18 years in the present study.
Regarding the first of them, local recurrence and the presence of cervical lymph node metastasis were evaluated. No significant differences were found, demonstrating that the 2 techniques are effective for tumor control (RR of 0.76, 95% CI 0.43-1.36). This has been found in other systematic reviews and meta-analyses consulted27,28 and in other primary studies,13,29-31 which show us that these percutaneous interventions constitute an alternative for the treatment of CDT T1a.
Hoarseness was studied in terms of safety. Hoarseness was subclassified into transient and permanent. Given the clinical relevance of the latter, it is of transcendental importance in the quality of life of patients.14-17 Although no statistically significant differences were found in transient hoarseness (duration less than 6 months), in permanent hoarseness it was shown that there was a difference in favor of ablation techniques with respect to surgery by 71% (RR of 0.29, 95% CI 0.11-0.75). In evaluated studies, this complication has been reported as the most frequent in TA techniques, mainly in tumor lesions close to the posterior capsule.12,18 Although thermal ablation techniques are not innocuous and may represent a potential risk of hoarseness, it generally occurs transiently. This voice complication during TA can be caused by heat injury, bleeding, or even with the administration of anesthesia.15,17 To avoid this type of complication, the hydrodissection technique is used.12,16,20 Surprisingly, in the study by Zhou, 14 where the laser was evaluated, no cases of hoarseness were obtained in comparison with the other techniques. However, it would be necessary to evaluate more studies with a greater number of patients to determine the impact on this outcome between each of the thermal ablation techniques.
In the presence of infection or hematoma, there were no statistically significant differences when comparing these 2 therapies, which shows us that despite the fact that surgery is an invasive procedure, the experience of the surgeon and the surgical technique are essential to counteract these complications.
In the current systematic review and meta-analysis, thermal ablation techniques and surgery were not considered comparable with respect to variables such as hypoparathyroidism and hypothyroidism, despite being commented on in several of the selected primary studies. Surgical techniques could have this type of complication after vascular manipulation and thyroid tissue extraction. On the other hand, there is very little probability of presenting these events in thermal ablation.7,8,10
Among the 10 selected studies, 2 of them included patients with CDT with both T1a and T1b tumor sizes, with an average maximum diameter of 12 mm.12,18 In addition, there are already studies evaluating the behavior of thyroid carcinoma in patients with CDT T1b, with tumor sizes of 1.4 cm, 32 and T2 reaching 3.8 cm, 33 where there were no differences in terms of effectiveness with respect to surgical management. This shows the experience of TA techniques in larger tumors. However, more studies are needed to observe the behavior of this treatment in tumors of these sizes.
It is important to clarify that the current indications for performing procedures such as TA in malignant thyroid nodules, based on the 2017 Korean guidelines for RFA 10 and on subsequent studies,34,35 are not only related to the size of these (less than 1 cm), but also according to the type of patient. For example, in those who refuse or cannot undergo surgical treatment, it could be an option for those who do not have lymph node metastases, except that are central without surgical indication, or distant, or that present high-risk histologies. It also constitutes an alternative as a form of palliative treatment to improve compression symptoms and thus quality of life.10,34 The location of the carcinoma is also of vital importance and constitutes another indication, where it is intended to have at least 2 mm of normal perilesional thyroid tissue, and it should not be adjacent to the thyroid capsule, absence of concave angle with the thyroid, that is not close to the isthmus, to the recurrent laryngeal nerve or the trachea or some posterior location.34,35
In the same way, the ultrasound characteristics of the nodules such as solidity, the absence of large calcifications, and the single nodule constitute important indications for this type of percutaneous intervention.10,34
This study has some strengths and limitations. Among the strengths, it can be observed that despite the fact that other systematic reviews and meta-analyses have studied the complications of TA with respect to surgery, 27 they have described them generally, without specifically establishing the differences between each type of complication. In our study, we evaluated hoarseness and especially its permanent presentation, given its importance in the quality of life of patients. Second, in this study, it was possible to evaluate the 3 main TA techniques for the treatment of CDT, such as radiofrequency, laser, and microwave (the latter being more representative).
Among the limitations of this study, we found that a total of 2939 patients were included in the 10 selected studies. It is expected that a greater number of patients would also improve the quality of the research. However, this number is similar to that of other systematic reviews and meta-analyses on this topic.27,28 In addition, most of the studies chosen are observational, which have the implicit possibility of selection bias; therefore, the availability of randomized clinical trials is necessary to obtain more solid results. In addition, the follow-up to assess relapse in thyroid cancer in these studies is still very short. Besides, the patients in the selected studies were from the Asian continent, which demonstrates the state of research on these techniques in these countries, particularly in China. It is recommended to encourage the execution of TA techniques as a treatment for thyroid cancer in the Latin American population to have more experience and a greater number of studies on this topic.
Conclusion
In this systematic review and meta-analysis, it can be observed that thermal ablation techniques for the treatment of T1aN0M0 PTC are equally effective when compared with surgical techniques in terms of local recurrence and the presence of cervical lymph node metastases, therefore offering a better profile. Safety, particularly in permanent hoarseness, also establishes TA as an excellent therapeutic alternative in selected patients.
Footnotes
Acknowledgements
The authors would like to thank Dr. Claudia Ibañez for her dedication and collaboration in the methodological aspects of the work.
Data Availability
The information was obtained from primary studies extracted from databases for subsequent analysis and interpretation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The resources allocated for this article are those of the authors.
Ethical Considerations
The group of researchers follows the topics for medical research in humans according to the Declaration of Helsinki—59th General Assembly, Seoul, Korea, October 2008, additionally taking into consideration the resolution 8430 of 1993 in Colombia, which establishes the requirements for the development of research activity in health. We consider that the study can be classified as “risk-free research” given that it is a secondary study that will analyze original primary studies without making any intervention or modification to them. In addition, authorship and the veracity of the information will be respected in all publications consulted and the authors will not make a biased selection of the articles. The authors will be included regardless of the results presented if they fulfill the inclusion criteria.