
Abstract
Objective:
To provide an up-to-date review summarizing the pathophysiology and management of the most common orbital and intracranial complications of acute rhinosinusitis (ARS).
Methods:
A narrative literature review was conducted using the following search criteria in the PubMed database: “sinusitis” AND “complications” AND (“orbital” OR “intracranial” OR “osseous” OR “Pott’s puffy tumor”). Titles and abstracts were screened for relevance. Additional articles were found by hand-searching references. Articles were chosen for inclusion based upon relevance, quality, full-text availability, and date of publication. Common or interesting radiographic findings were highlighted as figures using patient imaging data based on senior author expert opinion.
Results:
ARS is one of the most common diagnoses made in the United States. While the vast majority of these cases resolve with oral antibiotics and conservative medical management, rare instances of ARS may be complicated by the spread of infection into orbital, intracranial, and osseous spaces. This review seeks to guide physician management with evidence-based recommendations. The pathophysiology of complex sinusitis is explored and risk factors, evaluation, and up-to-date prevention and management recommendations are discussed. This review of the literature highlights that when orbital, intracranial, and osseus complications are suspected, a multidisciplinary team should be assembled to consider both medical and surgical management options. In this way, outcomes of these complex infections can be optimized.
Conclusions:
ARS is common and self-resolving in most cases. However, clinicians should suspect orbital and intracranial complications in at-risk individuals with worsening symptoms that do not respond to standard therapies, and initiate early interventions as directed by multidisciplinary teams.
Keywords
Introduction
Acute rhinosinusitis (ARS) is extremely common, accounting for 20% of antibiotic prescriptions and billions of dollars in annual health care expenditures.1,2 Most patients will be seen by primary care physicians in the office or in an urgent care setting. Most often, these infections will respond appropriately to medical management. This narrative review is dedicated to the discussion of complicated ARS with infectious spread into the orbit, bone, or central nervous system requiring more aggressive interventions.
ARS begins as infection and inflammation of the nasal and paranasal sinus mucosa. Most ARS is viral in etiology and resolves with supportive symptomatic management alone. Acute bacterial rhinosinusitis is suspected when symptoms last for more than 10 days or if a “double worsening” occurs after initial improvement. Most ARS can be managed medically in an outpatient setting with topical decongestion, nasal irrigation, oral antibiotics, and oral steroids. 3 Although hospitalizations related to ARS are less common today than in the past, surgical intervention is more common and length of hospital stay is increasing, suggesting an increase in the severity of these infections over time. 4
Extra-sinus complications can occur when there is orbital, intracranial, or osseous spread of infection. These can be life-threatening and may require urgent otolaryngologic, ophthalmologic, and/or neurosurgical consultation. When these complications are identified, patients often require inpatient admission for intravenous medication administration, continuous vital monitoring, serial assessments, multidisciplinary coordination of care, and surgical intervention. The pathophysiology and risk factors that give rise to these complications will be discussed. In addition, management recommendations will be reviewed.
Methods
Literature Review
A literature review was conducted using the National Institute of Health PubMed online database using the following search criteria: “sinusitis” AND “complications” AND (“orbital” OR “intracranial” OR “osseous” OR “Pott’s puffy tumor”). Additional articles were identified through hand-searching references. The literature review and screening of articles were conducted by the authors M.T.W., J.S.G., and B.A. Articles were categorized and outlined by M.T.W. Final articles were chosen by A.Z.P., J.H.F., C.C.L.T., and M.B.C. Articles were chosen for inclusion in this narrative review based on the following criteria: (1) they are of historical significance based on consensus opinion of the authors, (2) they provide relevant and robust scientific background for reference, (3) they either support or challenge a practice in this field for which there is no current consensus, and/or (4) they are recently published in the last 10 years and present new data or ideas surrounding the management of sinusitis pertinent to an otolaryngology readership. Effort was made to exclude studies that had poor scientific methodology or that support widely-accepted practices without providing added value to the literature.
Figure Generation
Figures that demonstrate common or interesting radiographic findings of orbital, osseous, and intracranial complications of ARS were identified from the clinics of senior authors and the de-identified according to an approved institutional review board study protocol.
Results
Our literature review identified the following categories of extra-sinus ARS complications: orbital, intracranial, and osseous. They are reviewed in turn.
Orbital Complications of Sinusitis
Given the close proximity of the paranasal sinuses to the orbit, and the thin and porous nature of the lamina papyracea, which separates these compartments, orbital complications account for the majority of complex sinusitis (75%-85%).5,6 The Chandler classification system (Table 1) is often used to describe the spectrum of orbital complications and can also be viewed as a sequence of progressively-worsening sequalae culminating in intracranial hematologic spread via the cavernous sinus.7,8 Of note, however, this classification system is not strictly progressive, and early classes do not have to precede later classes in presentation. When orbital involvement is suspected, admission for inpatient care is typically indicated. This allows for expedient workup and management, including appropriate imaging, administration of intravenous antibiotics, close monitoring, and consultation with involved specialists, including otolaryngology and ophthalmology.
Chandler Classification of Orbital Complications of Sinusitis.
Classes I and II of the Chandler classification system are preseptal and orbital cellulitis, respectively. Preseptal cellulitis is characterized by infection of subcutaneous eyelid tissue anterior to the septum without involvement of the globe, whereas orbital cellulitis involves the soft tissue posterior to the orbital septum. While both conditions can present with overlapping symptoms such as pain, edema, and eyelid erythema, orbital cellulitis may also demonstrate proptosis, chemosis, decreased visual acuity, and ophthalmoplegia. Most often, conservative therapy with broad spectrum oral antibiotics and nasal decongestants can successfully treat preseptal cellulitis.5,9,10 However, orbital cellulitis may require the use of intravenous antibiotics and, in some cases, surgical debridement. As such, orbital cellulitis is generally considered to be more severe than preseptal cellulitis. 11 Notably, if an afferent pupillary defect is observed in the setting of orbital cellulitis, an emergent decompression with canthotomy or cantholysis may also be necessary, as this may be suggestive of a potential optic nerve compression. 9
Classes III and IV of the Chandler classification system are subperiosteal and orbital abscesses, respectively. A subperiosteal abscess forms between the periorbita and the orbital wall. Subperiosteal abscesses most commonly develop along the medial orbital wall to due to the direct spread of infection from the adjacent ethmoid sinuses through the thin lamina papyracea (Figure 1) 12 ; however, subperiosteal abscesses can form along the inferior, superior, and less commonly, lateral, walls as well. If a subperiosteal abscess ruptures or progresses, it can result in the development of an orbital abscess. Intraorbital abscesses can result in a mass effect that can displace orbital structures within the confines of the restricted bony orbit. 9 This displacement often contributes to symptoms of proptosis and restricted ocular mobility. 9 Orbital abscesses, however, often result in more severe proptosis and ophthalmoplegia relative to subperiosteal abscesses and may even result in vision loss. 9 These intraorbital abscesses are strongly associated with underlying sinusitis in at least one sinus, and an estimated 63% of patients have multiple sinus involvement. 13 When treating any intraorbital abscess, a combination of endoscopic surgery, possible orbitotomy, and antibiotic therapy is generally preferred, as a purely-medical approach is associated with high recurrence rates.14,15 Surgically, transorbital and endoscopic approaches to subperiosteal and orbital abscess have similar outcomes,16,17 although longer hospital stays have been reported for external approaches. 18 However, not all abscesses are amenable to an endonasal approach, and those located more superiorly and laterally within the orbit may be best approached via an external or transconjunctival orbitotomy. 19 And while most abscesses have better outcomes with a surgical approach, there are exceptions to this rule. The Garcia-Harris criteria suggest surgical intervention can be avoided for subperiosteal abscesses if all of the following criteria are met: 9 years or younger, no evidence of frontal sinusitis, medial location, small size, no suspicion of anaerobic infection such as presence of gas, no prior attempt at drainage, no suggestion of chronic rhinosinusitis, no visual changes, no evidence of optic neuropathy or retinopathy, and a non-odontogenic infection. 20 For these patients, a treatment algorithm incorporating 24 to 48 hours of medical management with intravenous antibiotics, nasal decongestion, head of bed elevation, and serial examination has been suggested. 21
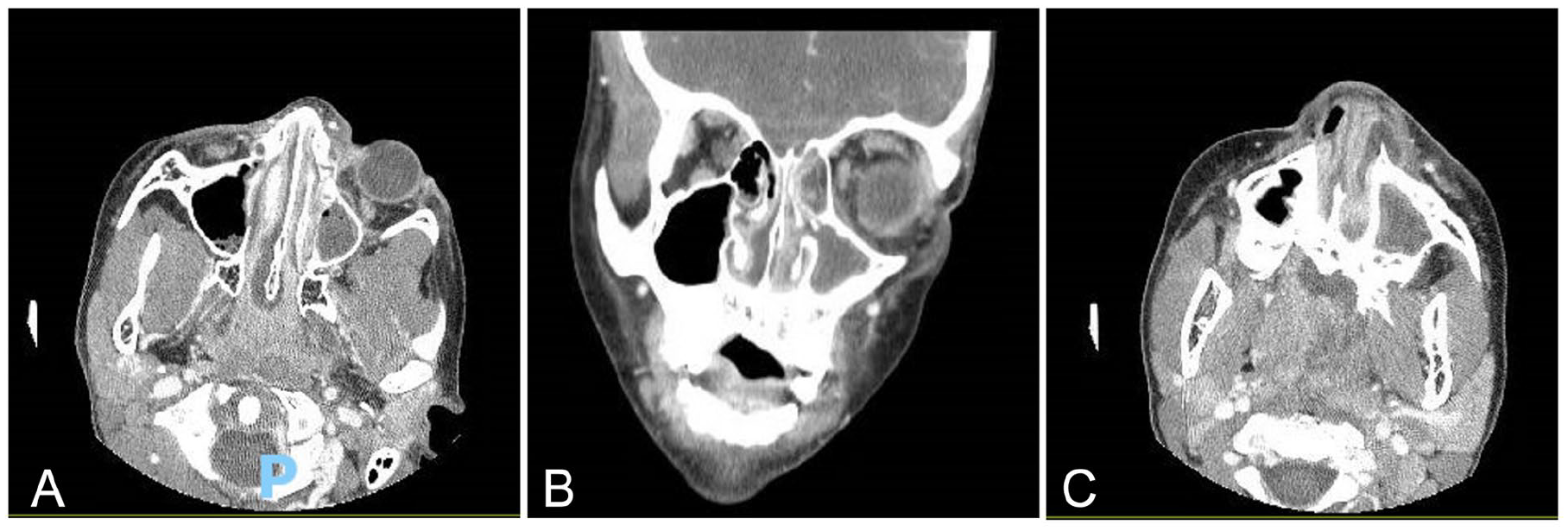
Tweleve-year-old male with history of cavities, periorbital swelling, restricted extraocular movement, and nasal congestion. Coronal computed tomography (CT) maxillofacial with contrast demonstrating near-complete opacification of the left frontal and maxillary sinuses and bilateral ethmoid air cells. There is a small peripherally enhancing fluid collection along the inferior medial left orbital wall and the medial inferior orbital wall consistent with subperiosteal abscess (A and B, axial and coronal images). There is also peripherally-enhancing fluid deep to the left nasal vestibule along the maxilla surrounding the frontal process, within the left maxillary gingiva along the alveolar ridge of the incisors and extending into the nasal cavity (C).
The final class of the Chandler Classification is cavernous sinus thrombosis (CST), a serious complication of sinusitis. Despite its location intracranially, CST is included in the Chandler classification of orbital findings given that orbital infection can directly inoculate the cavernous sinus via the upper and lower valveless ophthalmic veins and because the presenting clinical symptoms often include headache, fever, photophobia, diplopia, and vision loss.22,23 The dural sinuses and cerebral emissary veins lack valves, allowing blood to flow bidirectionally based on pressure gradients within the vascular system. This anatomical feature, combined with extensive vascular connections of the centrally-located cavernous sinuses, makes them particularly susceptible to septic thrombosis originating from infections at sites beyond the sinuses and orbit, as well. 22 Nonetheless, sinusitis, particularly involving the sphenoid and ethmoid sinuses, appear to be the most common source of infection leading to CST, with or without concurrent orbital involvement. Presenting symptoms of CST may be similar to those of orbital cellulitis or intraorbital abscesses, including the presence of proptosis, ophthalmoplegia, and chemosis. However, the presence of ptosis or other cranial nerve palsies is suggestive of CST. 9 Additional findings may include mild papilledema, retinal venous engorgement, and very often, additional neurological sequalae.22,23 These hallmarks of CST stem from cranial nerve III to VI impairment and venous congestion affecting the retinal and orbital vessels, as these neurovascular structures communicate via the cavernous sinuses. Patients with CST are often septic. The infection can rapidly spread to the opposite eye via the inter-cavernous sinuses, often within 24 to 48 hours of initial unilateral periorbital edema. 23
When CST is suspected and diagnosed, prompt medical and surgical attention is paramount. The administration of intravenous broad-spectrum antibiotics is the cornerstone of treatment and may be continued for at least 2 weeks beyond clinical resolution. Anticoagulation is also a pillar of treatment. It is recommended in a scientific statement from the American Heart Association regarding cerebral venous thrombosis 24 and is supported for CST specifically by a large individual patient data meta-analysis. 25 Initial treatment with a rapidly-reversible parental unfractionated heparin is recommended followed by a transition to a long-acting agent once the patient’s condition stabilizes.23,26 The role of corticosteroids in the treatment of CST remains controversial. Although they may reduce vasogenic edema and intracranial hypertension, they have prothrombotic properties. In a prospective study, steroids in the acute phase of cerebral venous thrombosis did not improve outcomes and was associated with worse prognosis in patients with parenchymal lesions. 27 Simultaneously, timely endoscopic surgery to decompress the primary site of infection is critical. 23
Intracranial Complications of Sinusitis
While intracranial complications of sinusitis remain rare, they can have substantial morbidity and occasional mortality, necessitating prompt recognition and management. Among patients with intracranial complications, the average hospital length of stay is 3 to 6 weeks and approximately half of patients require a second surgery. Further, up to one-third are readmitted within 60 days.28-31 Persistent neurologic deficits are seen in 3% to 24% of cases, and the fatality rate ranges from 0% to 16%.31-38 Since the COVID-19 pandemic, there has been a significant increase in the frequency of intracranial complications of ARS in children, 39 which is reflected in increased rates of neurosurgical intervention after March 2020. 40
Early recognition of an intracranial complication is a diagnostic challenge. Headache, fever, vomiting, and altered mental status may be the only presenting signs, even when the underlying etiology is sinusitis.29,32,41-47 Less than half of patients present with an abnormal neurologic examination on admission; however, those that do have a significantly longer length of stay.29,47 Reports vary regarding the most commonly affected sinus, with many citing the frontal sinus and others describing frequent involvement of the ethmoid, maxillary, and sphenoid.37,42,46 Patients with frontal sinus involvement on average require a greater number of surgical procedures. 48 Streptococcal species are most common pathogens leading to intracranial complications of sinusitis.49-51 Infections caused by Streptococcus anginosus result in more severe complications, have higher rates of neurosurgical intervention, are more likely to develop long-term neurologic deficits, and require longer duration of antibiotic therapy. 50 All patients are treated with prolonged courses of antibiotics, with an average duration of around 5 to 7 weeks.47,49 Reported rates of required surgical intervention vary significantly, ranging from 30% to 95% of patients.52-54
The most common intracranial complications of sinusitis are subdural empyemas and epidural abscesses. 55 Other reported complications include intracerebral abscess, meningitis, encephalitis, dural sinus thrombophlebitis, CST (discussed as an orbital complication above given inclusion in the Chandler classification system), and epidural and subdural hematomas.54-56 Mucoceles can also expand and cause erosion or dehiscence with intracranial (or orbital) extension. Although these are rarely the result of an acute sinusitis, an acute pyomucoele may present with acute findings (Figure 2).
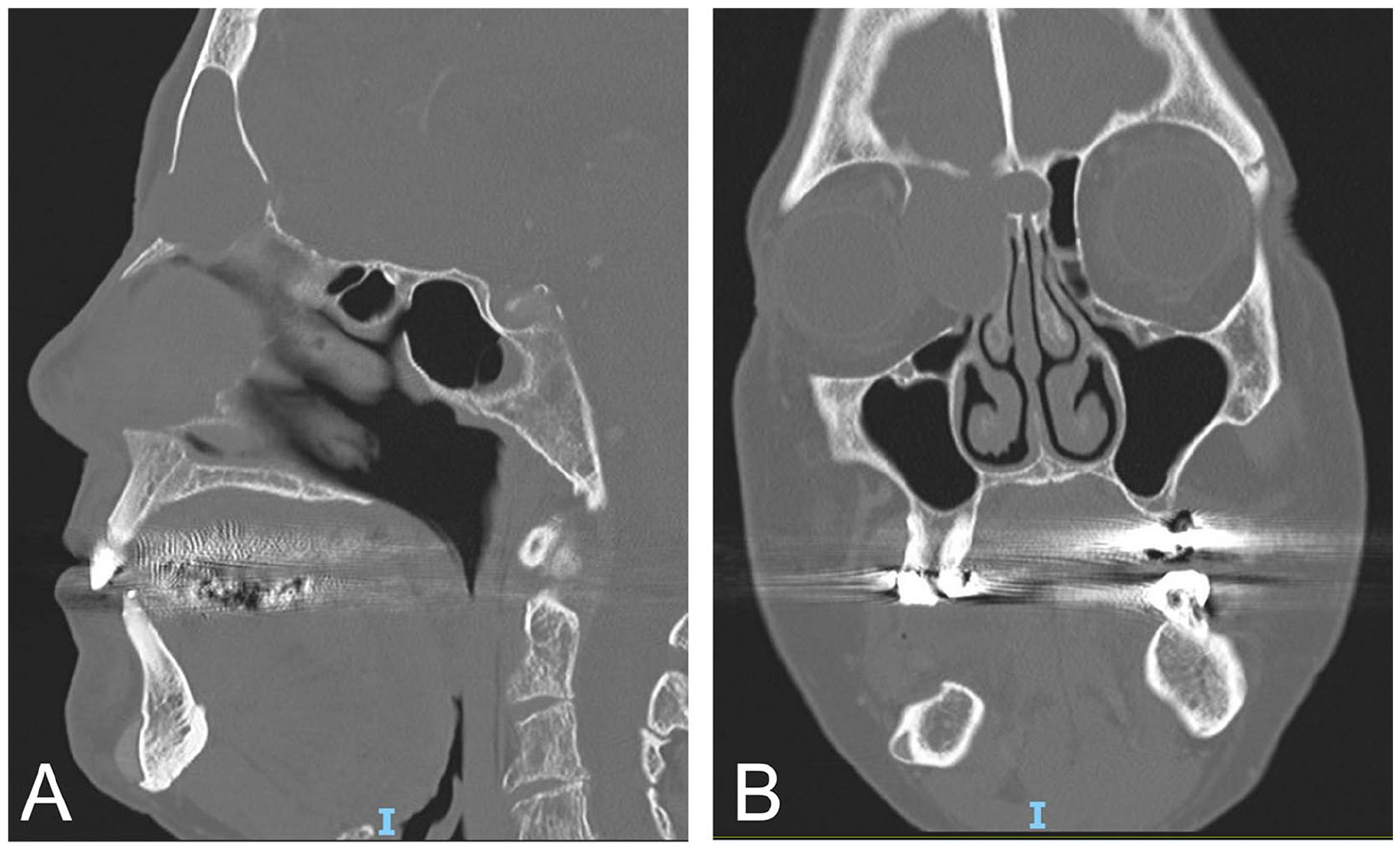
Seventy-six-year-old female with forehead swelling, pain, and pressure. Sagittal (A) and coronal (B) CT maxillofacial images demonstrating an expansile right frontoethmoidal lesion with nonenhancing fluid consistent with mucocele. There is near-complete obliteration of the left frontal sinus lumen with extension into the anterior crista galli and medial extraconal compartment of the right orbit.
Epidural and subdural extension of ARS are often a sequalae of retrograde thrombophlebitis due to direct seeding of these spaces by infectious material via valveless diploic veins. Direct extension of infection through calvarial wall or skull base can also occur. Epidural abscesses make up 23% to 61% of intracranial complications of ARS.54-57 Epidural abscesses occur between the calvarial inner table and underlying periosteum. Clinically, these patients often present with a headache and more indolent course, due to the tight adhesion between the periosteum and inner table. On imaging, epidural abscesses have a lenticular shape and do not cross suture lines. They appear as low-density collections with variable mass effect on CT. On MRI, they appear hyperintense on T2 with variable T1 signal intensity, depending on the presence of proteinaceous or hemorrhagic content. 10 Subdural empyemas are more aggressive and can develop rapidly over 24 to 48 hours if untreated. The frontal sinus is most often the source sinus, and subdural empyemas are often associated with osseus complications such as osteomyelitis and forehead subperiosteal abscess (discussed below).58,59 The medical management of epidural abscesses and subdural empyemas includes intravenous antibiotics, seizure prophylaxis, and interventions that lower intracranial pressure. A craniotomy for surgical drainage has been shown to decrease recurrences in comparison with one or more burr holes. 60
Cerebral abscesses are less common than epidural and subdural collections, accounting for only 3% to 22% of patients with intracranial sinusitis complications.61,62 The clinical presentation typically includes a triad of fever, headache, and focal neurologic findings; however, this is more commonly seen in adult patients than in pediatric patients. These lesions may be preceded by cerebritis, which is evident on MRI T2/FLAIR imaging (Figure 3). Treatment conventionally includes antibiotic therapy and craniotomy for neurosurgical drainage of intracranial abscesses. Interestingly, the role of endoscopic sinus surgery in the setting of an intracranial abscess remains controversial. In a propensity-score-matched study comparing patients who underwent neurosurgical drainage of sinogenic intracranial abscess with and without endoscopic sinus surgery, there was no benefit to the addition of endoscopic sinus surgery seen across multiple outcomes including mortality, readmission, revision neurosurgery, or length of stay. 63 Therefore, serial diffusion-weighted MRI can be useful in monitoring treatment response with endoscopic sinus surgery reserved for those with refractory infections.
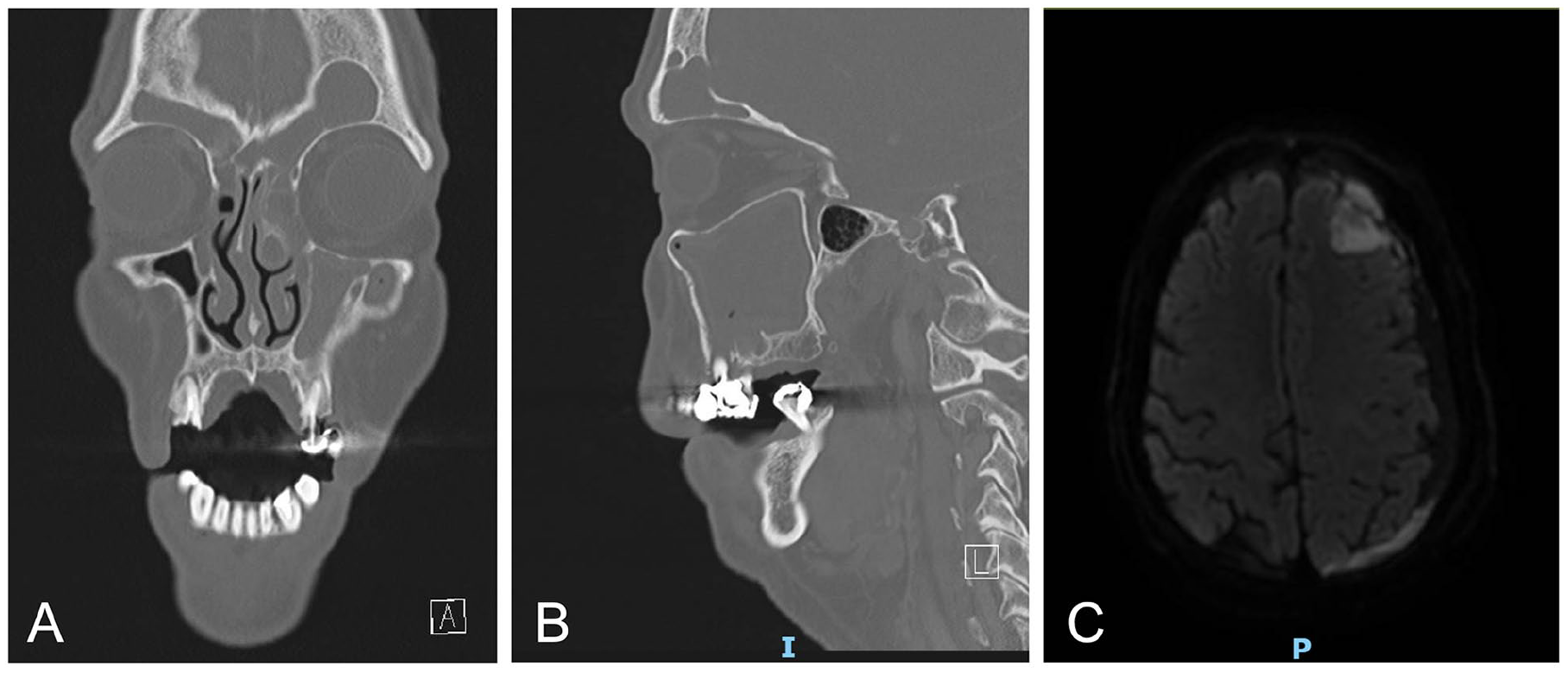
Seventy-year-old male with chronic rhinosinusitis presenting with altered mental status, seizures, and fever. Axial (A) and sagittal (B) CT maxillofacial with contrast demonstrating completed opacified left frontal sinus with wide dehiscence at inner table. Axial MRI brain with contrast (C) demonstrating T2/FLAIR hyperintense signal abnormality in the left frontal lobe subjacent to the subdural fluid collection concerning for cerebritis (developing cerebral abscess).
Meningitis is a rare complication of sinusitis.54,55,57 Meningitis can occur through hematogenous seeding or direct contiguous spread. Hematogenous seeding occurs when bacteria colonize the nasopharynx and enter the bloodstream through mucosal invasion. The bacteria then cross the blood-brain barrier in the subarachnoid space, causing a direct inflammatory and immunologic reaction. Direct contiguous spread is caused by organisms entering the cerebrospinal fluid from adjacent structures, such as in patients with otitis media or sinusitis, congenital malformations, trauma, or during surgery. 64 Clinically, patients present with fever and headache, which may or may not be accompanied by cerebral dysfunction. The presence of meningeal enhancement is a defining feature, which can be seen best on MRI. 10 Treatment of these patients includes antibiotic therapy and corticosteroids in cases of acute deterioration or significant cerebral edema, with some patients undergoing surgery, including endoscopic sinus surgery, craniotomy, and frontal trephination.34,42,43,55,56
Osseous Complications of Sinusitis
Patients may also present with an osseous complication of sinusitis. A common osseous complication is the development of a forehead subperiosteal abscess, known as Pott’s (or Pott) puffy tumor (Figures 4 and 5). 65 While Pott’s puffy tumor may be an independent finding, it may also present concurrent to intracranial complications due to the bidirectional spread of thrombophlebitis through the valveless venous system. The unique clinical signs of Pott’s puffy tumor usually include frontal scalp swelling, headache, and frontal sinus tenderness. On imaging, bone destruction of the inner or outer tables of the frontal sinus is best visualized with a CT scan. However, there are most often simultaneous findings of frontal osteomyelitis, which are best demonstrated on MRI with bone marrow edema and enhancement. 10 The treatment of Pott’s puffy tumor includes a prolonged course of intravenous antibiotic therapy, endoscopic sinus surgery, and endoscopic or external drainage of the abscess. Due to the oft-associated osteomyelitis, a prolonged course of intravenous antibiotics, usually 4 to 8 weeks duration for acute cases and up to 6 months for chronic osteomyelitis, is typically recommended. 66 Intranasal or intravenous corticosteroids may be used to reduce inflammation, 67 although to our knowledge, there are no studies that address the use of steroids specifically in Pott’s puffy tumor, and chronic use has been associated with osseous and intracranial spread. 68
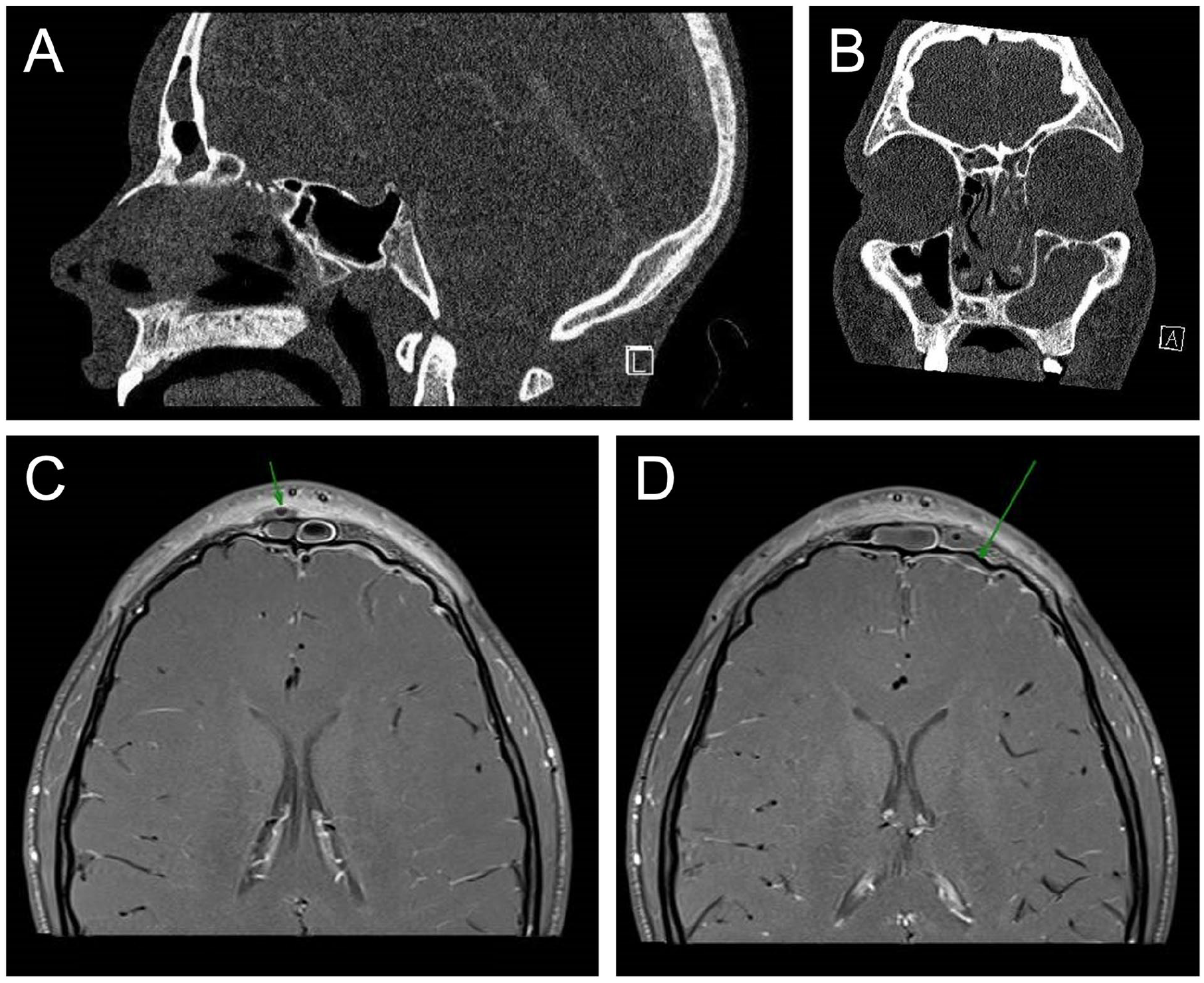
Fifteen-year-old male presenting with headaches, nasal congestion, and periorbital and forehead swelling. Sagittal (A) and coronal (B) CT sinus with contrast demonstrating complete opacification of the left frontal and maxillary sinuses with ostiomeatal narrowing and opacification, anterior thinning of the frontal cortex without obvious dehiscence, and subperiosteal rim-enhancing collection of fluid and gas (not shown). Axial MRI brain and face with contrast images demonstrating subgaleal subperiosteal abscess overlying the right frontal sinus (C) and enhancing dural membranes over both frontal poles with tiny left frontal polar subdural empyema (D) as shown by green arrows.
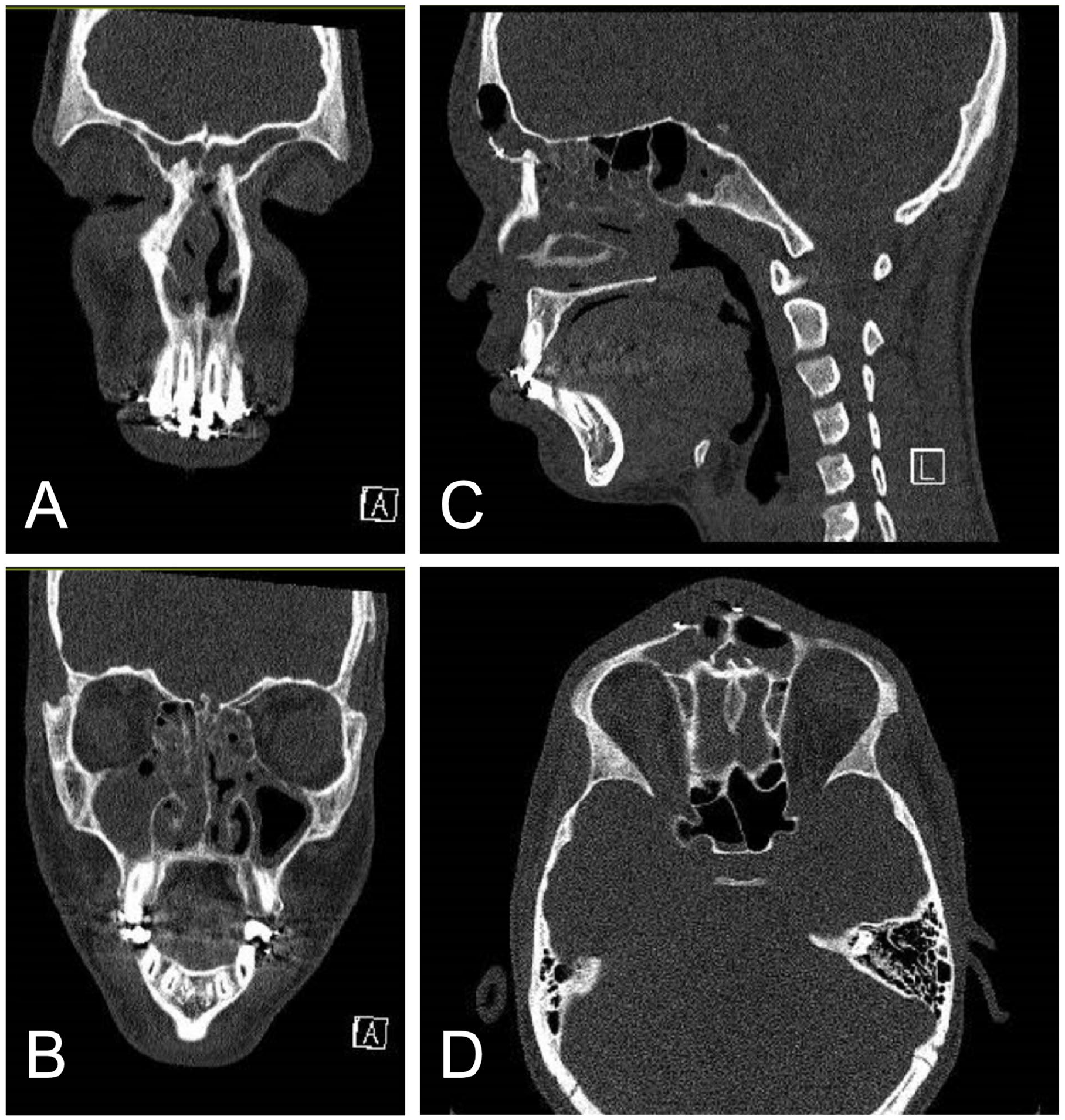
Thirteen-year-old male with a history of frontal bone plating after motor vehicle accident presents with upper respiratory symptoms and forehead swelling. Coronal CT maxillofacial with contrast demonstrating complete opacification of bilateral frontal sinuses and right maxillary sinus with significant ethmoid involvement bilaterally (A and B). Sagittal (C) and axial (D) images showing bony defect in the anterior wall of the right frontal sinus near previous plate-screw fixation of fractures involving the anterior wall of the frontal sinus and nasal bridge with focus of gas extending from the left frontal sinus, through the bony defect, into the left frontal scalp soft tissues.
Regarding the need and extent of required surgery, a large recent review of the literature that encompassed 184 reported patients revealed that only 7 (3.8%) patients did not undergo surgery. 69 A combined endoscopic and external approach was more likely performed in cases involving intracranial complications, 69 and some studies show that intracranial extension does not necessarily require neurosurgical intervention if there is sufficient external or endoscopic drainage. 70 Data regarding the extent of endoscopic sinus surgery necessary and sufficient are not readily reported, 71 but it is generally recognized that in cases of extensive osteomyelitis, more complete removal of infected bone is warranted.10,34,41 For example, a Draf III frontal sinusotomy creates the maximal possible frontal drainage pathway and has been shown to be effective for treating Pott’s puffy infections even in the setting of large obstructing Kuhn type IV frontal cells, 72 but this surgery requires specialized training that might not be readily available and may not always be necessary.
Discussion
Risk Factors for Orbital and Intracranial Complications
While the majority of ARS resolves with appropriate medical management, several factors can predispose an individual to orbital and intracranial complications from ARS. These include age, involved sinus distribution, and medical comorbidities.
Younger patients are more at risk of orbital complications than older patients. 71 While age does not necessarily affect the risk of intracranial complications, intracranial complications in children are not typically associated with any significant comorbidities, and the underlying sinusitis is often subclinical, unlike in adults,34,43,46 so there must be a lower threshold to suspect intracranial involvement in pediatric ARS. Similarly, many advocate the use of both MRI brain and orbital imaging, in addition to CT sinus scans, in patients presenting with orbital findings in order to detect any concomitant intracranial findings that may be missed initially. 73 Regarding the distribution of involved sinuses, a case-control study comparing complicated and uncomplicated ARS in adult patients, ethmoid sinusitis and a short duration of symptoms were found to statistically associate with orbital complications. 74 In a large review of adults and pediatric patients with ARS, the majority of orbital complications occurred in pediatric patients with ethmoidal disease, whereas in adults pansinusitis was more common. 75 In a retrospective review of 118 patients with isolated sphenoid rhinosinusitis, visual changes including diplopia, extraocular muscle limitation, ptosis, and visual deficits were the most common orbital complications, often associated with facial pain and headache but not nasal congestion or obstruction. 76
In addition to age and anatomic considerations, patient medical comorbidities are important risk factors. Diabetes mellitus, malignant neoplasm, and bony dehiscence were significant predictors of orbital complications of ARS. 76 Further, in a review of a large centralized database of health reimbursements, it was shown that in over 700,000 cases of ARS, a history of illicit drug use, previous head injury, previous skull surgery or malformations, or immunocompromised state were statistically associated with increased risk of hospitalization and severe complications including the orbital and intracranial sequalae mentioned above as well as sepsis. 77
Chronic Rhinosinusitis as a Factor in ARS Complications
Though chronic rhinosinusitis (CRS) is a chronic inflammatory process, acute infectious exacerbations of CRS are associated with male sex, higher BMI, and higher asthma and allergic rhinitis rates as well as eosinophil count and nasal polyp burden. 78 These episodic changes, on top of the underlying chronic bone remodeling and thinning of the skull base and lamina papyracea, can predispose an individual with CRS to orbital and intracranial complications of acute exacerbations. In a study examining complications after endoscopic transsphenoidal surgery, underlying CRS was shown to be significantly associated with postoperative ARS and meningitis, but not with other complications such as epistaxis or cerebrospinal fluid (CSF) leak. 79 These data suggest that CRS can predispose a patient to a complicated ARS if there is an acute insult to the sinuses as mimicked by transsphenoidal surgery. It is conceivable that bacteria can be transmitted more easily through a chronically thinned or dehiscent lamina papyracea or sphenoid roof leading to orbital and central nervous system infections.
Do Antibiotics Reduce ARS Complication Rates?
Interestingly, antibiotic prescriptions were associated with increased hospitalization but did not reduce the rate of sinogenic complications, indicating that there was no clear benefit of oral antibiotics in preventing downstream ARS complications. 77 This finding is consistent with several prior retrospective studies showing that the usage of antibiotics for ARS does not seem to prevent the occurrence of subperiosteal abscesses.80,81 Nevertheless, oral antibiotics—namely, amoxicillin, and amoxicillin-clavulanate—are recommended for ARS by the American Academy of Otolaryngology – Head and Neck Surgery, with a treatment failure rate of only 3.1%.3,82
While oral antibiotics may not prevent the development of a complicated sinusitis, antibiotics can prevent morbidity of orbital, intracranial, or osseous complications. The value of antibiotics is evident when comparing the current mortality rate from orbital cellulitis (1%-2%) to that of the pre-antibiotic era, which was 19%. Likewise, significant morbidities such as permanent vision loss was reduced from 20% to near 0%, although 3% to 11% can still have decreased visual acuity after an episode of orbital cellulitis. 83 A broad-spectrum antibiotic coverage that includes gram-positive, gram-negative, and anaerobic bacteria with adequate penetration into the orbit and central nervous system is important, further guided by culture-directed narrowing. 84 Common antibiotics used empirically include vancomycin in combination with cefotaxime and metronidazole or clindamycin. Other options include piperacillin-tazobactam, ticarcillin-clavulanate, and ceftriaxone. In penicillin-allergic individuals, a fluoroquinolone in combination with vancomycin can be used. 84 In placebo-controlled studies, complication rates of ARS are similar regardless of the initial management with oral antibiotics, demonstrating the value of intravenous therapy in the management of these complications.85,86
Adjuvant Treatment With Steroids and Nasal Irrigation
The use of glucocorticoids in the medical management or preoperative management of orbital and preseptal cellulitis remains controversial due to concerns over suppressing the host immune system. However, it has been shown to reduce mucosal inflammation and cytokine expression in children with subperiosteal abscesses and conceptionally could help promote sinonasal drainage and resolution of sinusitis. 87 Importantly, corticosteroids do not appear to have a negative impact on subperiosteal abscess outcomes. 88
The value of high-volume, low-pressure nasal saline irrigations to remove obstructive mucus and promote mucociliary flow should be considered, as they may help prevent the sequalae of preseptal and orbital cellulitis.89,90 In a prospective study of children with ARS, randomization to normal saline nasal irrigation was associated with an improvement in Pediatric Rhinoconjunctivitis Quality of Life and acute sinusitis symptoms. 91 In adults, a systematic review and meta-analysis for adult ARS patients treated with nasal saline, disease-specific quality of life scores and composite symptoms scores were only improved in patients with viral ARS and for those using high-volume rinses, indicating the need for high-volume rinses in comparison with low-volume nasal saline spray particularly in the setting of bacterial sinusitis. 92 In the setting of CRS, nasal saline irrigation is recommended based on a preponderance of low-level evidence, but high-level evidence and recommendations regarding optimal delivery method and solution composition remain lacking.93,94 Although these studies do not specifically evaluate the role of saline irrigations with respect to complicated sinusitis, early resolution of symptoms would suggest a decrease in complication rate or, in the event of a complication, a quicker recovery. The American Academy of Otolaryngology – Head and Neck Surgery clinical practice guidelines recommend nasal irrigation as an option for viral and bacterial ARS based on grade B evidence. 3
Conclusion
Sinusitis may be complicated by orbital, intracranial, or osseous infection. The spread of infection into these neighboring cavities must always be considered, particularly when patients do not improve with standard medical therapies. CT imaging of the sinus and MRI imaging of the brain and orbits are important tools to aid in diagnosis when there is clinical suspicion. The correct diagnosis is paramount in allowing for timely treatment and to promote resolution and prevent further infectious complications. Intravenous antibiotics, nasal decongestion, nasal irrigation, and in some cases, surgical intervention are the pillars of management when complex sinusitis is identified. Future areas of study should focus on de-escalation of aggressive surgical management for Pott’s puffy tumor, as has been shown in the case of intracranial complications, and the potential role of adjunctive topical or systemic steroid treatments. With modern tools of diagnosis and multidisciplinary team approaches to treatment, long-term outcomes are very good and long-term morbidity associated with complex sinusitis is low.
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.