
Abstract
Introduction
Cough is one of the leading reasons for seeking medical attention worldwide and has been estimated to affect up to 33% of patients. 1 Chronic cough, a complaint often seen by otolaryngologists, is defined as a cough lasting over 8 weeks in adults. 2 Etiology of chronic cough may include underlying respiratory conditions, medication side effects, upper airway cough syndrome, gastroesophageal reflux disease (GERD), or idiopathic origin. 1,2 In addition to signaling potential underlying respiratory conditions, symptoms of pain and discomfort with cough can significantly diminish patients’ quality of life. 1,3
The Cough Severity Index (CSI) is a validated patient questionnaire that allows physicians to understand the perceived impact chronic cough may have upon a patient’s quality of life. It was developed and validated in 2013; it is currently used widely in patient-reported assessment of cough. 4,5 Reflux Severity Index (RSI), Glottal Function Index (GFI), and Voice-Related Quality of Life (VRQOL) are other patient-reported outcome measures (PROMs) used to analyze patient’s symptoms, some of which may be related to chronic cough. Understanding the impact symptoms can have upon a patient’s quality of life can allow physicians to tailor care to patient needs.
It has been posited that chronic cough may have a psychosomatic component in some cases, indicating the need to better understand the role of concomitant mental health diagnoses. 1 -3 Anxiety and depression have been linked to increased patient-reported disease severity of several otolaryngological conditions such as dysphonia, migraines, and reflux. 6,7 Addressing coexisting anxiety or depression may positively impact outcomes. Studies have shown, for example, that within those with benign dysphonia, treatment of anxiety was associated with improvement in Voice Handicap Index-10 scores. 7 Understanding patients’ unique needs and the impact of coexisting mental health conditions is important in providing interdisciplinary care for patients with chronic conditions such as cough.
Of note, though some studies have delved into the impact anxiety and depression may have on patients’ perception of symptoms, 8 often these studies focus on symptoms of anxiety or depression exhibited at presentation. Clinically, however, physicians may rely on the medical record (a previously recorded diagnosis or anxiety or depression) rather than interview about current symptoms when understanding a patient’s current mental health. PROMs are likely understood in the context of prior diagnoses; yet, this may be unfairly biased. Early research is beginning to investigate this, 9 but many questions remain unanswered.
We aim to investigate the association of a diagnosis of anxiety or depression with PROMs of perceived cough severity. We hypothesize that patients with diagnoses of anxiety or depression are likely to score higher on the CSI than patients without a prior mental health diagnosis. Secondary analysis of associations of anxiety and depression status with scores and other measures (RSI, VRQOL, and GFI) will also be conducted.
Materials and Methods
Study Population
We performed a retrospective cohort study of patients who received a diagnosis of chronic cough. Patients were identified by the report of an ICD-10 code (Cough R05.3) at their initial presentation to a laryngology clinic between January 1, 2019 and December 31, 2019 at a tertiary academic clinic. Patients were excluded if they did not have a completed CSI score at their visit or were under the age of 18. The study was approved by the Institutional Review Board (No. 202101136) of Washington University School of Medicine.
Data Collection
Data were collected through a retrospective chart review. A diagnosis of anxiety and depression was determined by one of the three ways. The first was if the patient carried ICD-10 Codes listed for F41.0-F41.9 (Other Anxiety disorders), F33.0-F33.9 (Major depressive disorder), or F32.0-F32.9 (Depressive episode). The second was if a physician’s note listed a clinical diagnosis within the last year. Otherwise, patients were considered to have a diagnosis of anxiety or depression if it was listed in the problem list within the last year. Data on psychotropic medication usage at the time of the appointment were collected. Medications were categorized into selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, tricyclic antidepressants, benzodiazepines, or atypical antidepressants.
The primary outcome measure for the study was the score for the CSI. Secondary outcomes were RSI, GFI, and VRQOL scores that were collected for all patients at the initial evaluation. Each patient underwent laryngeal examination as part of their standard evaluation. Etiology of cough, as determined by laryngologist, was categorized into one of the following: multifactorial/unknown, gastrointestinal (e.g., reflux), pulmonary, neurogenic, behavioral (e.g., paradoxical vocal fold motion), upper airway cough syndrome/post-nasal, or other.
Statistical Analysis
Frequency and relative frequency were used to summarize the categorical data. For continuous-level data, the normal distribution assumption was explored using histograms and Shapiro–Wilk’s test. When data were normally distributed, mean and standard deviation were used to summarize the continuous-level variable. Median and range were used for data not normally distributed. Kruskal–Wallis test was used to compare the study outcomes between the groups of patients with anxiety, depression, anxiety and depression, and neither anxiety nor depression. Mann–Whitney U test was used for post-hoc pairwise comparisons. Alpha level was preserved using Bonferroni’s correction for multiple comparisons. Robust regression analysis was used to explore the association between study group and outcome measures after controlling for potential confounders. Statistical analysis was performed using STATA 15.0 (Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC.) and alpha level for all analysis was set at .05.
Results and Analysis
Patient Characteristics
Of the 141 chronic cough patients identified in the study, the median age was 64 (20-85). There were 101 (72%) females and 123 (87%) patients were white. The majority of patients (n = 98, 71%) were never smokers, 35 (25%) were former smokers, and 5 (4%) were current smokers. In all, 81 patients (57%) had neither anxiety nor depression, 21 (15%) had anxiety only, 12 (9%) had depression, and 27 (19%) had both anxiety and depression. Distribution of characteristics by anxiety/depression group is presented in Table 1. Origin of cough was multifactorial/unknown in 61 (43%) patients, followed by behavioral causes in 31 (22%) patients and neurogenic in 24 (17%) patients. Five patients (4%) had “other” origin of cough: laryngeal cancer, fungal laryngitis, Zenker’s diverticulum, ulcerative laryngitis, and dysphagia.
Demographics of Chronic Cough Patients by Anxiety or Depression Diagnosis.
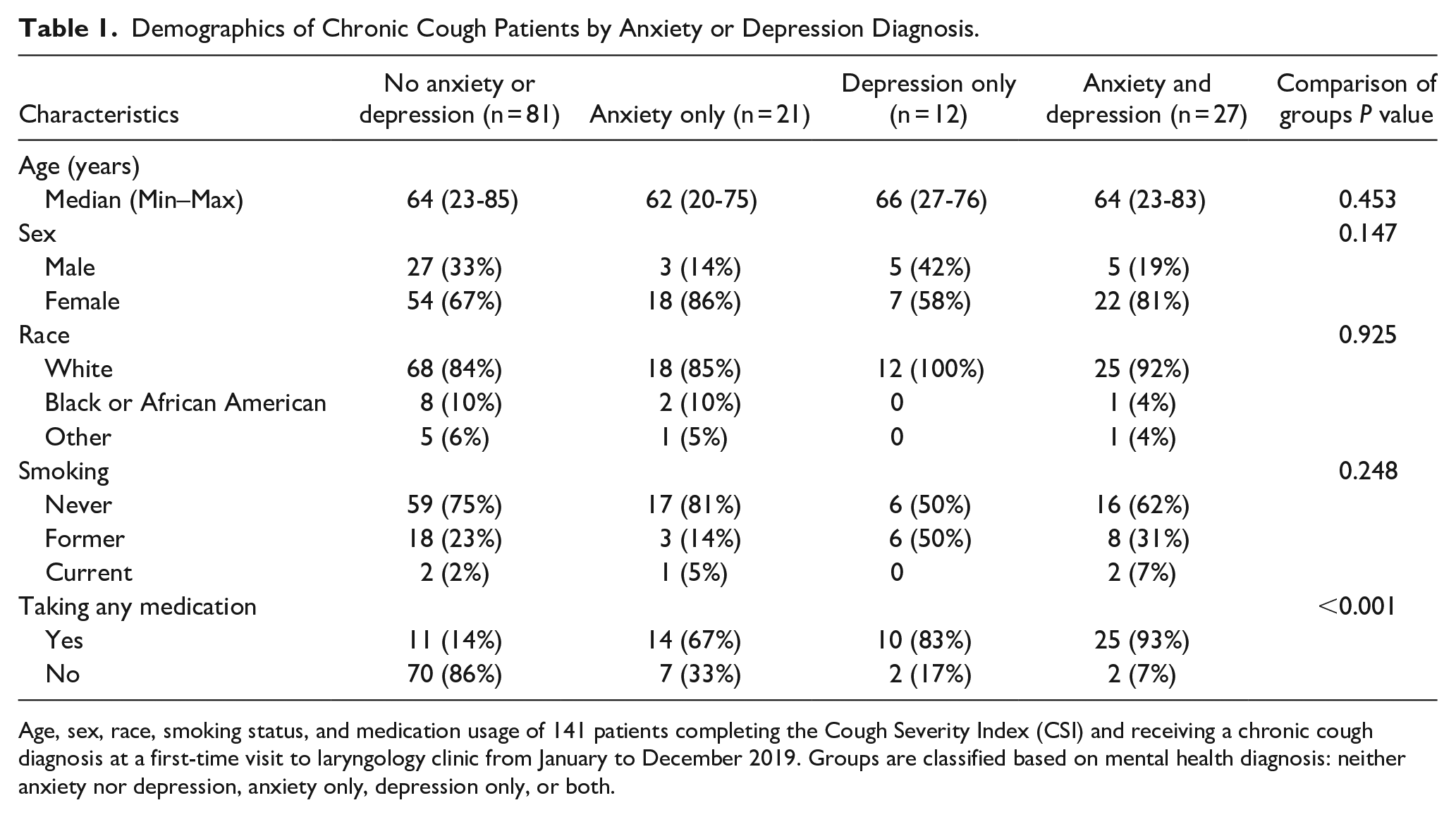
Age, sex, race, smoking status, and medication usage of 141 patients completing the Cough Severity Index (CSI) and receiving a chronic cough diagnosis at a first-time visit to laryngology clinic from January to December 2019. Groups are classified based on mental health diagnosis: neither anxiety nor depression, anxiety only, depression only, or both.
There was a higher proportion of patients using psychotropic medication among patients with both anxiety and depression (n = 25, 93%) as compared to patients with either depression (n = 10, 83%) or anxiety (n = 14, 67%) individually (Table 1). Ten patients were on tricyclic antidepressants (TCAs) (16% of those on psychotropic medication); four (6%) were on amitriptyline; and six (10%) were on nortriptyline. Among patients with anxiety and depression, only 2 (7%) did not take any medication; this proportion was higher among patients with anxiety only (n = 7, 33%) or depression only (n = 2, 17%).
Outcome Measures
The lowest CSI scores were observed in the group of patients with no anxiety or depression (median = 19, range 1-38) and the group of patients with anxiety only (median = 23, range 0-40). Patients with both anxiety and depression and patients with depression only had the highest CSI scores with median (min–max), respectively: 26 (5-39) and 26.5 (0-40) (Table 2).
Scores to Patient-Reported Outcome Measures by Anxiety or Depression Diagnosis.
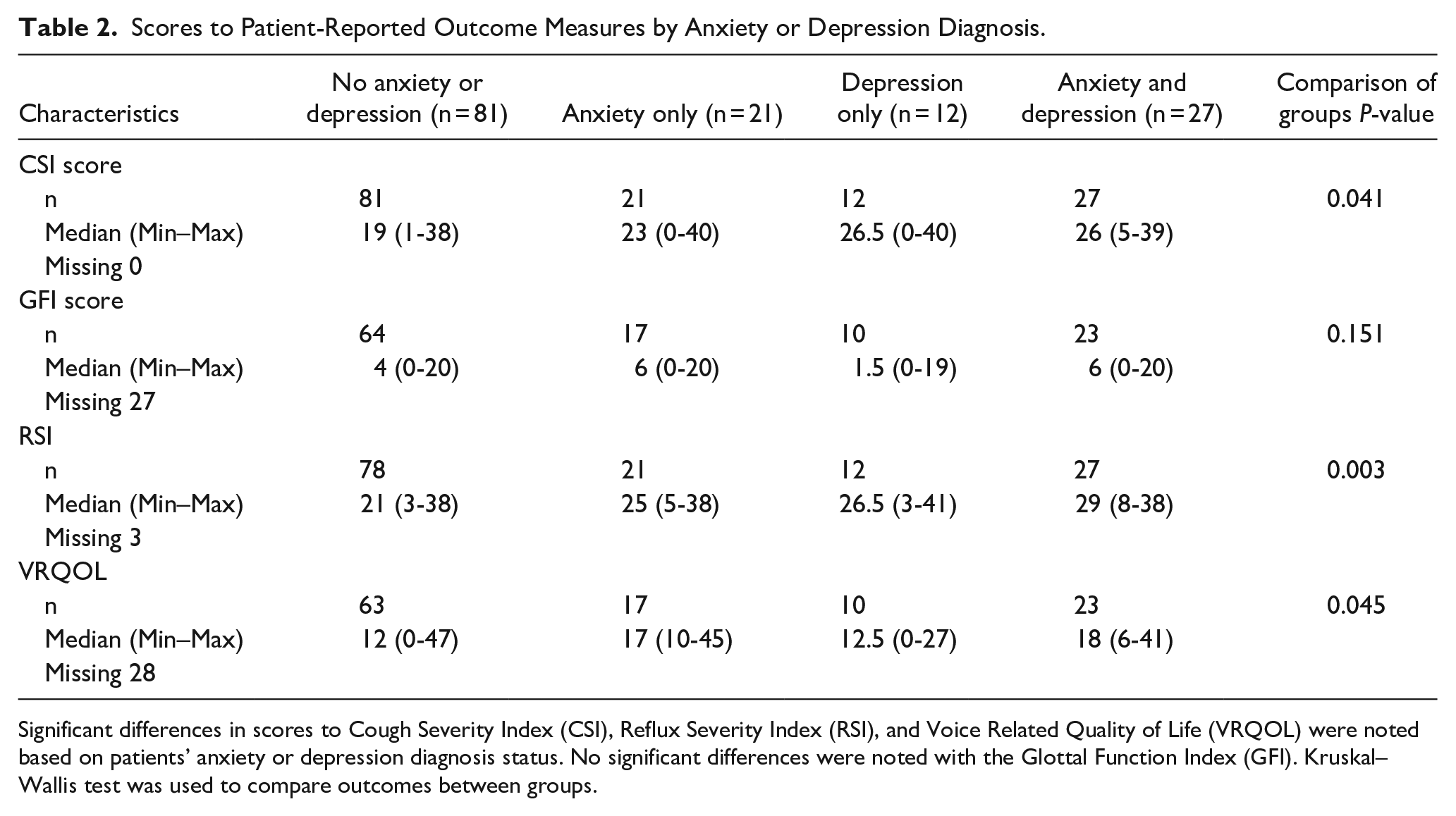
Significant differences in scores to Cough Severity Index (CSI), Reflux Severity Index (RSI), and Voice Related Quality of Life (VRQOL) were noted based on patients’ anxiety or depression diagnosis status. No significant differences were noted with the Glottal Function Index (GFI). Kruskal–Wallis test was used to compare outcomes between groups.
There was a significant difference in CSI scores between the four groups of patients (Kruskal–Wallis P = .041, Table 2). Post-hoc test revealed that CSI scores of patients with both anxiety and depression were significantly higher than CSI scores of patients with no such conditions [median difference = 6, 95% confident interval (CI): 2-11; P = .048]. The next largest difference was between CSI scores of patients with depression and patients with neither anxiety nor depression (median difference = 5, 95% CI: −2 to 11), but this difference was not statistically significant (P = .884).
Robust regression analysis revealed that after controlling for sex and smoking status, only patients with anxiety and depression had statistically significantly different CSI scores from patients with neither condition (difference = 4.70, 95% CI: 0.54-8.87, P = .027). Although not clinically definitive, these results suggest a potentially large difference in the populations (up to 8.87 points). Patients in the depression group had on average higher CSI scores than patients with neither condition (difference = 4.75, 95% CI: −1.52 to 11.02, P = .136). Although not statistically significant, the wide CI does not exclude a potentially large difference in the population for these two groups.
Similar trends were seen with RSI scores. The lowest RSI scores were once again observed in the group of patients with no anxiety or depression (median = 21, range 3-38) and the group of patients with anxiety only (median = 25, range 5-38). Patients with both anxiety and depression and patients with depression only had the highest RSI scores with median (min–max), respectively, 29 (8-38) and 26.5 (3-41) (Table 2). Pearson’s correlation coefficient between CSI and RSI scores was r = .495, indicating a large positive relationship. VRQOL scores were the lowest among patients with neither condition and patients with depression only with median (range), respectively, 12 (0-47) and 12.5 (0-27), and higher for patients with anxiety only [median 17, range (10-45)] or with anxiety and depression [median = 18, range (6-41)]. There was no difference in the distribution of GFI scores between the four study groups (P = .151) (Table 2).
Discussion
This study demonstrates important findings regarding prior diagnoses of anxiety and depression and the potential association with PROMs in chronic cough patients. The female predominance and age range of patients in this study strongly reflect the demographics noted in the worldwide Chronic Cough Registry, 10 indicating that our population may be generalizable. The reason for this predominance remains unknown. Hormone-mediated changes in mast cells and eosinophils, as well as increased somatosensory activation leading to cough sensitivity, are posited to play a role in the female predominance. Gender variations also exist in which patients seek medical care, which may also play a role in this case. 11 Regardless of the underlying etiology, the population in this study is reflective of the chronic cough population globally.
Chronic cough remains a complex diagnosis for many patients, as 43% of our patients had a combination of multiple factors or unknown etiology to their cough. Although patients were at their initial visit to a tertiary care laryngology clinic, many were likely at different points in a comprehensive cough workup (pulmonary, gastrointestinal, etc.). If a workup of chronic cough was just beginning, it stands to reason that the diagnosis would be listed as unknown (and future diagnostic tests or referrals may have been ordered). The next most common diagnosis was behavioral (21%). Paradoxical vocal fold motion episodes may cause cough and have historically demonstrated some improvement with a mixed cognitive-behavioral and muscle relaxation therapy. 12
Most patients with mental health conditions in this study were taking psychotropic medication; those with depression or both anxiety and depression were most likely to use medication. Nearly a fifth of the medications prescribed were TCAs. TCAs have multiple uses; these medications may have been prescribed for mental health reasons only, but can also be prescribed for neurogenic cough. There may be overlap of the medical indication, and this cannot be teased apart by retrospective review alone.
Among the general population, anxiety disorders are seen in 23.2% of adult females and 14.3% of adult men annually; 13 similarly, depression is noted in 9.6% of adult females and 6.0% of adult males. 14 Our study of chronic cough patients noted significantly higher rates of both anxiety and depression, at 34% and 27%, respectively. Chronic cough patients are likely to be at risk for increased mental health conditions due to various risk factors, including older age and physical illness. Chronic cough has been linked to increased sick days and impaired work productivity, which may further contribute to financial or psychosocial stressors. 15 Patients with anxiety disorders have demonstrated hypervigilance to somatic symptoms and increased engagement with healthcare systems, perhaps leading to increased rates of chronic cough diagnoses. 16,17 Any potential relationship between chronic cough and mental health may be bidirectional. Regardless, the higher rates of anxiety and depression highlight the importance of addressing comorbid mental health conditions in the treatment of chronic cough.
Most notably, this study highlights that patients with underlying depression and anxiety may be more likely to have high scores on PROMs, indicating more chronic-cough-related impairment. On both CSI and RSI, combined effect of anxiety and depression was more likely to see high scores in comparison to those with anxiety only, depression only, or neither condition. Literature has demonstrated that comorbid anxiety and depression often lead to persistence of symptoms for a longer duration, decreased quality of life, and impaired social and occupational functioning. 18
A positive correlation was seen between CSI and RSI scores within this patient population. Although patients with purely reflux-associated cough were low in our study, laryngeal irritation from GERD has been postulated to contribute to 25% to 40% of chronic cough patients. 19,20 Preexisting anxiety and depression have been linked to increased GERD symptoms, and in return, decreases in quality of life have been associated with worsening mental health. 21 Of note, increased stress can increase reflux symptoms. 22 -24
Studies of other laryngological conditions highlight that proper understanding and incorporation of mental health into the treatment plan have resulted in improved patient outcomes. 7,25 Providing adequate psychopharmacological and therapy-based control of anxiety and depression may better equip chronic cough patients to cope with psychologic distress related to pain, impaired social functioning, and perceptions of voice quality.
Our study is not without limitations. The small sample size of 141 patients is from 1 year of first-time clinic appointments; further data including more patients are necessary to corroborate findings. Further data may also be impacted by the coronavirus disease 2019 (COVID-19) pandemic, as chronic cough has been a lingering symptom for many. 26 Etiology of chronic cough (i.e., reflux, neurogenic) is determined subjectively; providers use their best clinical judgment but may have variations in criteria for different diagnoses. Furthermore, anxiety and depression diagnoses were determined from what was listed in the medical record; it does not account for disease severity, control of patients’ anxiety and depression, non-pharmaceutical management or whether these may be outdated diagnoses carried forward in the chart.
Previous studies of laryngological conditions have focused on concurrent symptoms of anxiety and depression; our study uses prior documentation of diagnosis, which may not as accurately reflect as a patient’s mental health status at the time. Despite this limitation, the data are very generalizable to what a physician may see in a clinic: a quick glance over the past medical history is often the depth into which providers delve into mental health, rather than focused or directed questioning. It is important to note that this study shows an association between anxiety and depression with severity of chronic cough, not a causality; chronic-cough-related impairment may both pre-date and exacerbate mental health symptoms. Prospective studies on changes in CSI scores after medication- or therapy-based management of anxiety and depression may help delineate how much of patients’ self-reported outcomes are due to treatable psychosocial elements.
Providers should be cautioned not to assume anxiety or depression diagnosis “explains” the severity of patient’s symptoms. Mental health is one component of a patient’s symptomatology but should not deter a provider from completing a thorough workup. By understanding patients’ mental health background, however, care providers may be able to more holistically understand and treat patients’ concerns.
Footnotes
Acknowledgements
No additional acknowledgment.
Authors’ Note
COSM 2022 Annual Meeting—American Laryngological Association Spring Meeting Dallas, Texas, USA; April 28–30th, 2022
Data availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from Washington University School of Medicine (No. 202101136).
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because this was a retrospective chart review.
Statement of Human or Animal Rights
This article does not contain any studies with human or animal subjects.