
Abstract
Nasopalatine duct cyst (NPDC) is the most common nonodontogenic cyst originating from the epithelial remnants of the incisive canal in the maxilla. NPDC is treated with complete enucleation via a sublabial or transpalatal approach, and recently tranasnasal endoscopic marsupialization has been gradually used. However, in large and extensive cases, it is difficult to remove the cyst completely, and there is a high risk of postoperative complications, including oronasal fistula. Therefore, tranasnasal endoscopic marsupialization is recommended as an effective treatment modality. Herein, we report a case of a 49-year-old man with a very large NPDC with a maximum diameter of 58 mm. NPDC was successfully managed by transnasal endoscopic marsupialization under general anesthesia without any major problems. No postoperative complications or recurrence occurred until 12 months postoperatively. Transnasal endoscopic marsupialization for large NPDC is minimally invasive and useful.
Introduction
Nasopalatine duct cyst (NPDC), also known as incisive canal cyst, is the most common nonodontogenic cyst in the maxilla. Although the exact etiology or pathogenesis of NPDC remains unknown, it is thought to originate from the epithelial remnants of the nasopalatine duct. It forms in the incisive canal in the alveolar process of the maxillary bone or soft tissue located on the incisive foramen in the palate. 1 Although NPDC can occur spontaneously, various factors, such as trauma, infections, or mucous retention, promote its development. 2
NPDC is conventionally treated through a sublabial or palatine approach, and marsupialization under transnasal endoscopic surgery is another treatment modality. Transnasal endoscopic marsupialization is particularly advantageous in cases of large cysts that carry a higher risk of complications, including infection, injury to tooth roots, and oronasal fistula.3,4 Recently, 9 cases of NPDC treated with transnasal endoscopic marsupialization have been reported.5 -8 Most cases demonstrated good therapeutic results without oronasal fistula, and the size of the lesions ranged from 22 to 31 mm. To date, no definite criteria regarding the size have been established in which marsupialization or complete removal will be advantageous, and surgeons must analyze each patient on a case-by-case basis.5
Herein, we report the successful treatment of a very large NPDC with a maximum diameter of 58 mm by transnasal endoscopic marsupialization. Transnasal endoscopic marsupialization for NPDC is minimally invasive and useful. Therefore, this case report will help surgeons make decisions when patients with similar conditions are encountered.
Case Report
A 49-year-old man was referred to the Otorhinolaryngology-Head and Neck Department at Guro Hospital of Korea University Medical Center with a cystic lesion in the maxilla incidentally detected on a radiographic examination performed prior to dental implantation. The patient reported nasal obstruction on the right side for 4 years but had no other symptoms. He had no relevant comorbidities or history of facial trauma. Nasal endoscopy revealed swelling in the right nasal floor, and the nasal septal deviated to the left (Figure 1A and B). Intraoral examination revealed a diffuse swelling located in the midline of the hard palate (Figure 1C). The lesion was soft, fluctuant, nontender, and without pulsation on palpation, and the overlying mucosa appeared normal in color. A computed tomography (CT) scan of the paranasal sinuses revealed an egg-shaped lesion with a well-defined border centered on the lower half of the nasal cavity and hard palate, 58 × 45 × 42 mm in size (Figure 2). The lesion was thought to originate from the nasopalatine duct. The lesion extended superiorly and inferiorly, with an elevation of the nasal floor, the nasal septum deviated to the left side, and bony destruction of the hard palate. We made a preoperative diagnosis of NPDC based on the clinical and imaging findings. The patient underwent marsupialization of the cystic lesion by transnasal endoscopic surgery under general anesthesia. An incision was made in the cyst through the thin bony wall of the bulging right nasal floor, and yellowish-cloudy pus was drained. The exposed bony wall, nasal floor mucosa, and cyst wall were removed using Blakesley thru-cutting-forceps, and the opening was completely enlarged and trimmed using a microdebrider (Figure 3). Histopathological examination revealed stratified squamous epithelium with dense lymphocyte infiltration, fibrous tissue under the epithelium, and no atypical cells and Staphylococcus epidermidis was isolated from pus in a culture test. These findings are consistent with those of the NPDC.
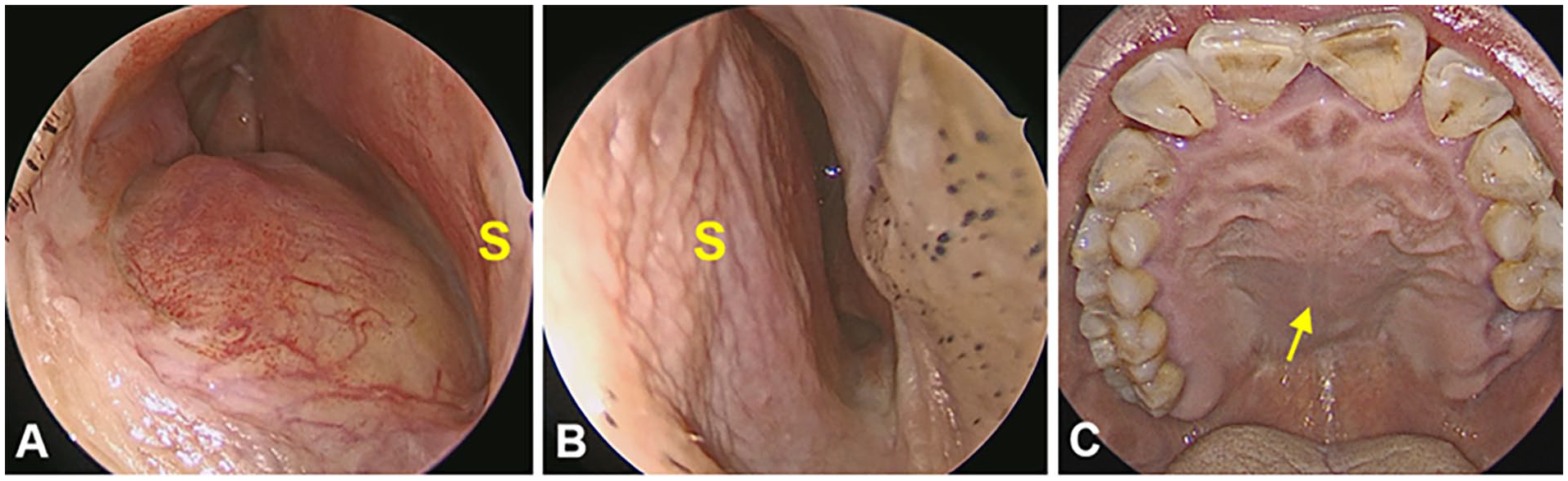
Preoperative nasal endoscopy reveals elevation of the nasal floor in the right nasal cavity (A), and the nasal septum deviated to the left side (B). Preoperative endoscopic view of the oral cavity (C) demonstrates diffuse swelling of the hard palate in the midline (arrow). S, nasal septum.
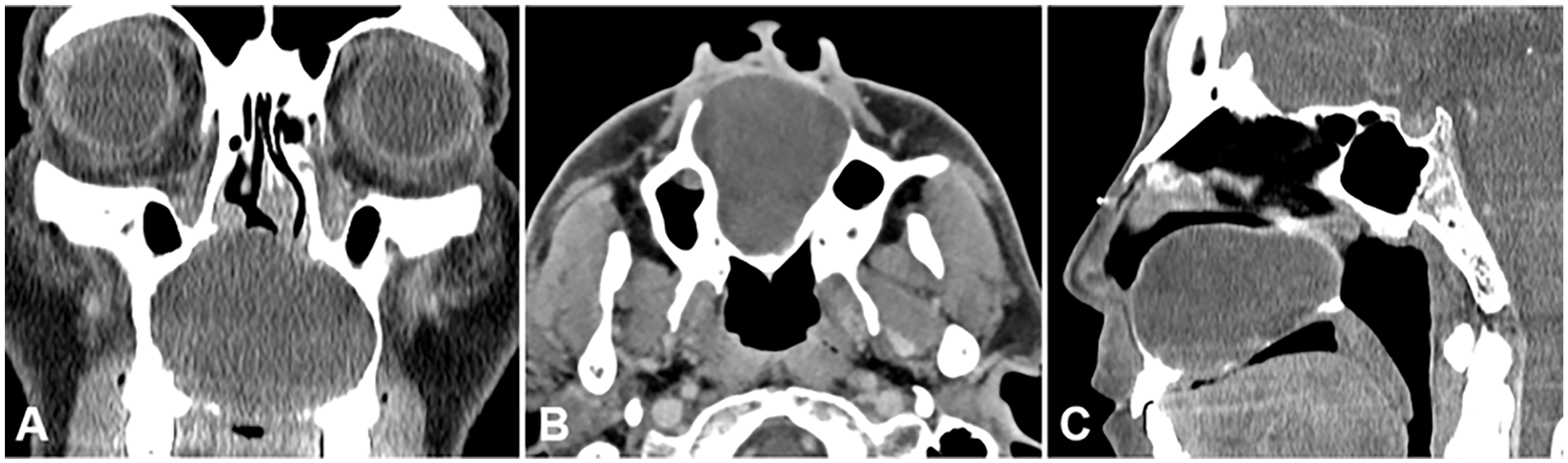
Preoperative CT scans of the paranasal sinuses. Coronal (A), axial (B), and sagittal (C) views demonstrate a huge cystic lesion in the maxilla. The lesion bulges superiorly toward the nasal floor and inferiorly toward the oral cavity with adjacent bone destruction. CT, computed tomography.
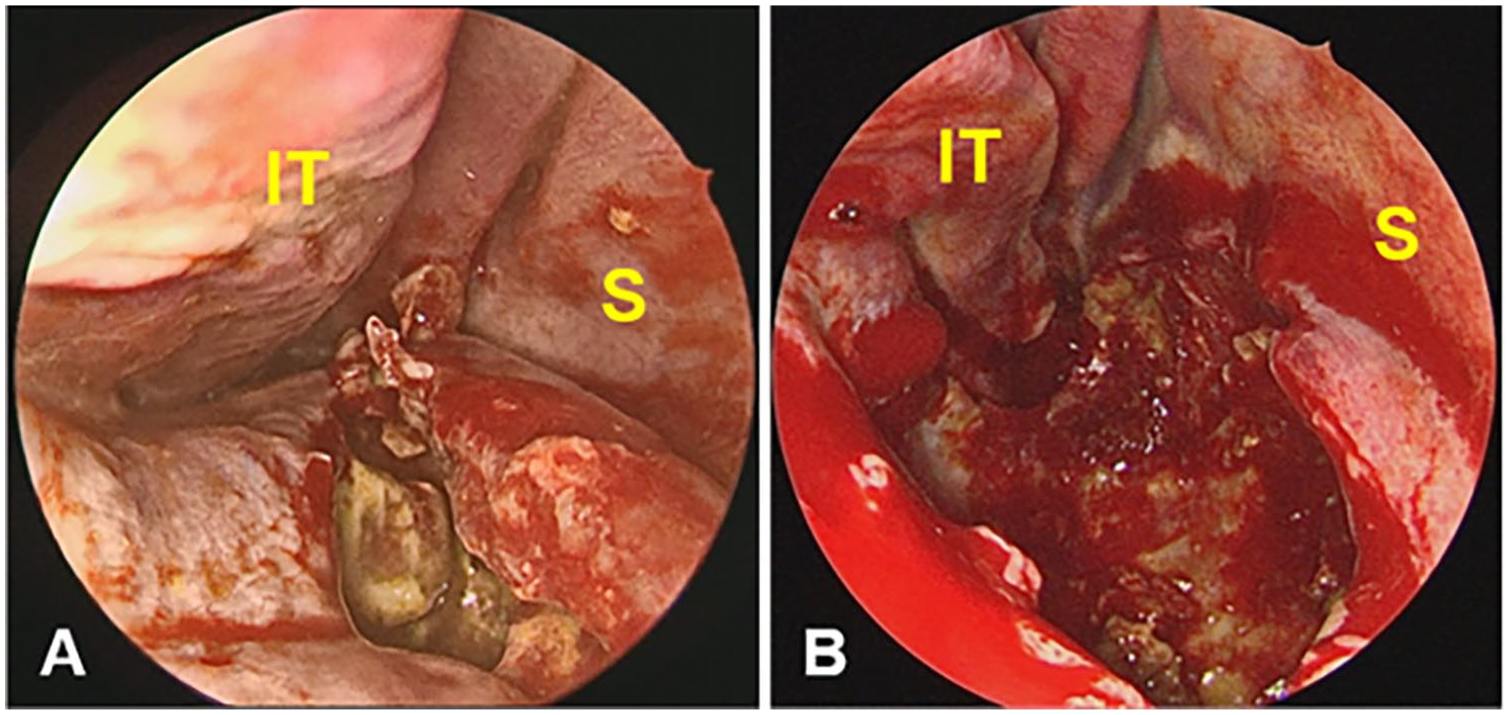
Intraoperative nasal endoscopy. An incision is made in the floor of the right nasal cavity, and yellowish, cloudy discharge is drained (A). Bones of the nasal floor are absent or very thin. Using cutting-forceps and microdebrider, the cystic lesion is opened widely and all the materials inside are removed (B). IT, inferior turbinate; S, nasal septum.
Follow-up nasal endoscopic examinations and CT of paranasal sinuses have been performed with no sign of recurrence 1 year after surgery and fenestration of the cyst remains open (Figure 4). The patient reported crust formation in the nasal cavity, but there was no other discomfort, and the sensation of the upper incisor region remained intact.
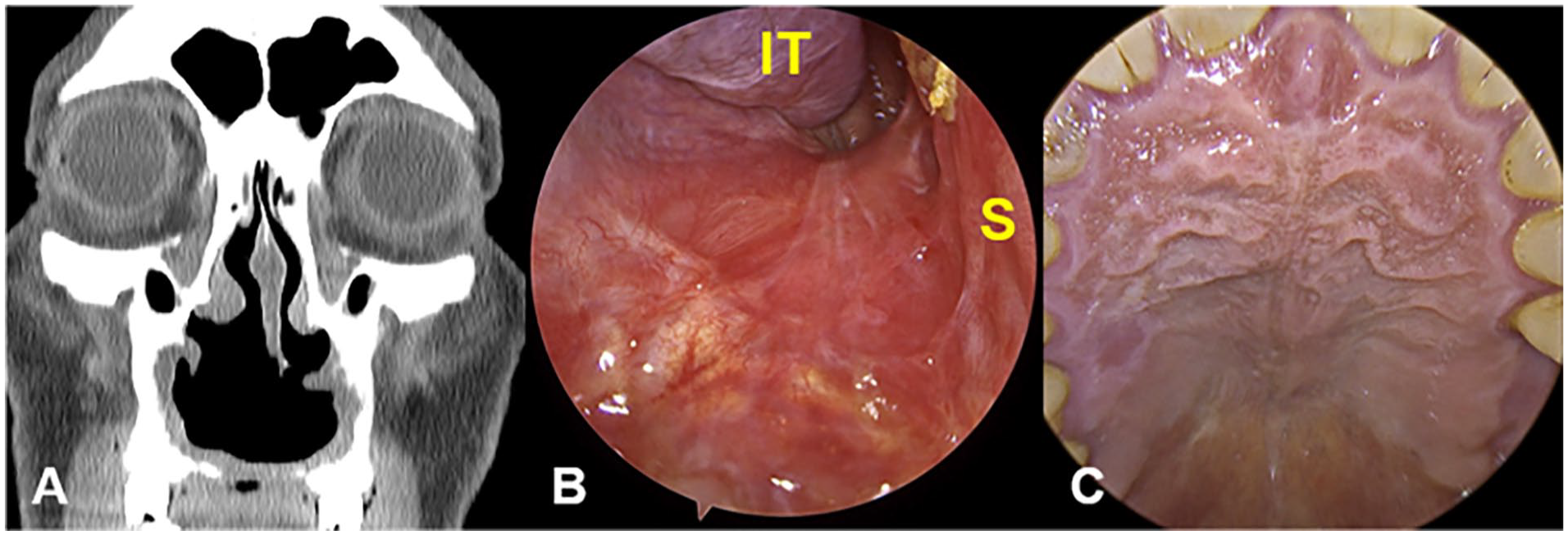
PNS CT scan and nasal endoscopy 12 months after surgery. The patency of the lesion after marsupialization was well-maintained (A). The wound was completely epithelialized without recurrence or any other major complications (B), and the swelling of the hard palate also disappeared (C). IT, inferior turbinate; S, nasal septum; PNS, paranasal sinus; CT, computed tomography.
Discussion
NPDC accounts for approximately 5% of all cystic lesions in the maxillofacial region and occurs in approximately 1% of the population.1,7 Most patients with NPDC present without symptoms, and NPDCs are observed incidentally during general physical examinations and imaging studies. The most common clinical manifestation is swelling of the anterior hard palate or labial gingiva and pain or pus drainage when infected. Cysts can be discovered in various sizes but typically have an average diameter of approximately 15 mm. 9 If the cyst enlarges extensively and involves the nasal cavity, patients may have nasal symptoms, including nasal obstruction.3,6
NPDC is diagnosed based on clinical symptoms, physical examinations, and imaging studies and can be confirmed through histopathologic findings. Imaging findings of NPDC typically show a well-defined radiolucent lesion in the midline of the anterior maxilla or a heart-shaped radiolucent lesion in the presence of anterior nasal spines. These findings can help differentiate NPDCs from other cysts that occur in the maxillary region, such as nasolabial and periapical cysts.1,5 Other diseases to be differentiated include an enlarged nasopalatine duct, central giant cell granuloma, osteitis fistulizing in the palatine direction, or bucconasal communication. 10 Histologically, NPDCs comprise various epithelial cell types that vary according to the distance between the cyst and nasal cavity. 1 The respiratory and squamous epithelia may be observed, individually or in combination, based on the anatomic location. The respiratory epithelium is mainly observed in cysts near the nasal cavity, whereas the squamous epithelium is more commonly found in lesions adjacent to the oral cavity.2,10
Surgical treatment is required if NPDC is accompanied by symptoms such as swelling or pain. Surgical treatment is also recommended even if an NPDC is only a small cyst or is asymptomatic because a secondary infection can cause perforation or fistula of the maxilla. A rare case of a malignant maxillary tumor originating from an NPDC has been reported.11,12
To date, the standard treatment for NPDC has been complete surgical removal using a sublabial or palatine approach. Surgical treatment includes complete cyst enucleation via a transoral sublabial or palatal approach and marsupialization with the transnasal endoscopic approach. Complete enucleation has been widely used and has demonstrated excellent prognosis and low recurrence rates. In particular, if the size of the cyst is so small that the location of the cyst cannot be determined by nasal endoscopy, a complete removal is recommended rather than marsupialization. 7 However, for large-sized NPDCs, complete enucleation is difficult, and there is an increase in the possibility of postoperative complications, such as submucosal hematoma, wound dehiscence, surgical site infection, oronasal fistula formation, and damage to the root or tooth and nasopalatine neurovascular bundles.1,3 As technology and skill-associated endoscopic nasal surgery have improved, marsupialization of NPDC via the transnasal endoscopic approach has been accepted as an effective treatment, especially in the case of large cysts with acceptable surgical outcomes.
In previous case reports, 9 patients were treated for NPDCs by transnasal endoscopic marsupialization.5 -8 These NPDCs were large, ranging from 22 to 31 mm, and were accompanied by swelling of the nasal floor or bony defects in the hard palate near the nasal cavity. Perforations of the inferior nasal septum were reported in 2 cases, but no other serious complications have been reported. No disease recurrence was observed. For large NPDCs or those with nasal involvement, transnasal endoscopic marsupialization is widely used as a safe and effective treatment.
In the present case, the maximum diameter of the NPDC was approximately 58 mm, much larger than that of cysts previously treated by marsupialization. The enucleation of an NPDC of this size is highly likely to result in postoperative complications. In another case report in which a 60 mm NPDC was treated with total enucleation via a sublabial approach, a secondary infection occurred because of the bone graft that was used to fill the dead space. 13
We performed transnasal endoscopic marsupialization instead of enucleation to prevent wound infection or fistula formation, and there was no surgical site infection or recurrence of the disease. We successfully used this approach for a very large NPDC. However, this type of surgery may be associated with an increased risk of recurrence when the NPDC is insufficiently open. Therefore, the nasal floor was resected as wide as possible to widen the cyst in front of the choana. The nasal floor wound healed well without surgical site infection or oroantral fistula, and patency after marsupialization was observed by nasal endoscopy 12 months after surgery. A large NPDC protruding into the nasal cavity can be easily and efficiently managed with transnasal endoscopic marsupialization as a substitute for complete enucleation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/Consent Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki.