
Abstract
This article presents the case of a full-term newborn who underwent tracheal intubation after birth due to rapid breathing and cyanosis of the lips. Ultrasonography, computer tomography (CT), and magnetic resonance imaging revealed the presence of a subglottic cyst. The patient underwent cyst marsupialization via endoscopy under general anesthesia, with successful extubation on the second postoperative day. In the later follow-up, it was shown that the cyst recurred quickly. However, the special feature of this case is that during the follow-up, the size of the cyst remained unchanged, but suddenly disappeared spontaneously in the third year. As for the reason for the disappearance of the cyst, we can only make theoretical speculations. Whether other recurrent cases will also resolve spontaneously, there are currently no relevant reports.
Keywords
Introduction
Subglottic cysts, a rare cause of infantile stridor and respiratory distress, are often observed in children with a history of tracheal intubation and ventilatory support and represent secondary changes. Congenital subglottic cysts are extremely rare, with an incidence of approximately 1.82 to 3.49 per 100,000 live births, and their specific pathophysiological mechanisms remain unclear. 1 Due to the low incidence of congenital subglottic cysts and the complexity of airway surgeries, treatment approaches are largely based on empirical evidence. This case is unique because the recurrent small cyst spontaneously regressed during follow-up. Our clinical approach is to monitor small cysts that do not affect neonatal growth and development, thereby avoiding secondary airway injury.
Case Report
The present case involved a full-term newborn who underwent a typical natural childbirth process. The birth weight was 3.6 kg, and Apgar scores were 8 at 1 minutes and 8 at 5 minutes post-birth. Within the first hour after birth, the infant progressively developed stridor and rapid breathing. Continuous inhalation of 30% oxygen at a flow rate of 0.6 L/minute was administered, but blood oxygen saturation did not reach 95%. Noninvasive oxygen ventilation (pressure-support) via face mask was attempted; however, the infant’s blood oxygen saturation level remained at 60%. The infant gradually developed cyanosis of the lips, which required immediate intubation with a size 3.0 endotracheal tube. During intubation, a suspicious neoplasm was observed below the vocal cords. Moreover, the intubation process encountered difficulties.
Consequently, the patient was transferred to a tertiary pediatric hospital. In the intensive care unit (ICU), the infant was mechanically ventilated with a ventilator setting of 36 breaths/minute, VT of 24 mL, FiO2 of 50%, and positive end-expiratory pressure (PEEP) of +4 cmH2O. Cardiac monitoring revealed the following parameters: heart rate (HR) of 120 beats/minute, BP of 65/32 mmHg, SpO2 of 98%, and temperature of 36.5°C. A neck CT scan revealed a round, low-density lesion characterized by smooth margins located anteriorly to the left of the trachea at the C5 level. The lesion had a CT value of approximately 9 Hounsfield Units (HU), with a maximum cross-sectional dimension of 8.6 mm by 7.5 mm. (Figure 1). Neck magnetic resonance imaging (MRI) revealed a cystic mass anterior to the left side of the trachea at approximately the C5 level, measuring approximately 8 × 7 mm, with elongated T1 and T2 signal shadows (Figure 2). Bedside fiberoptic bronchoscopy conducted by an otolaryngologist revealed a round neoplasm obstructing more than 75% of the subglottic airway, which was classified as Myer-Cotton grade III (Figure 3).
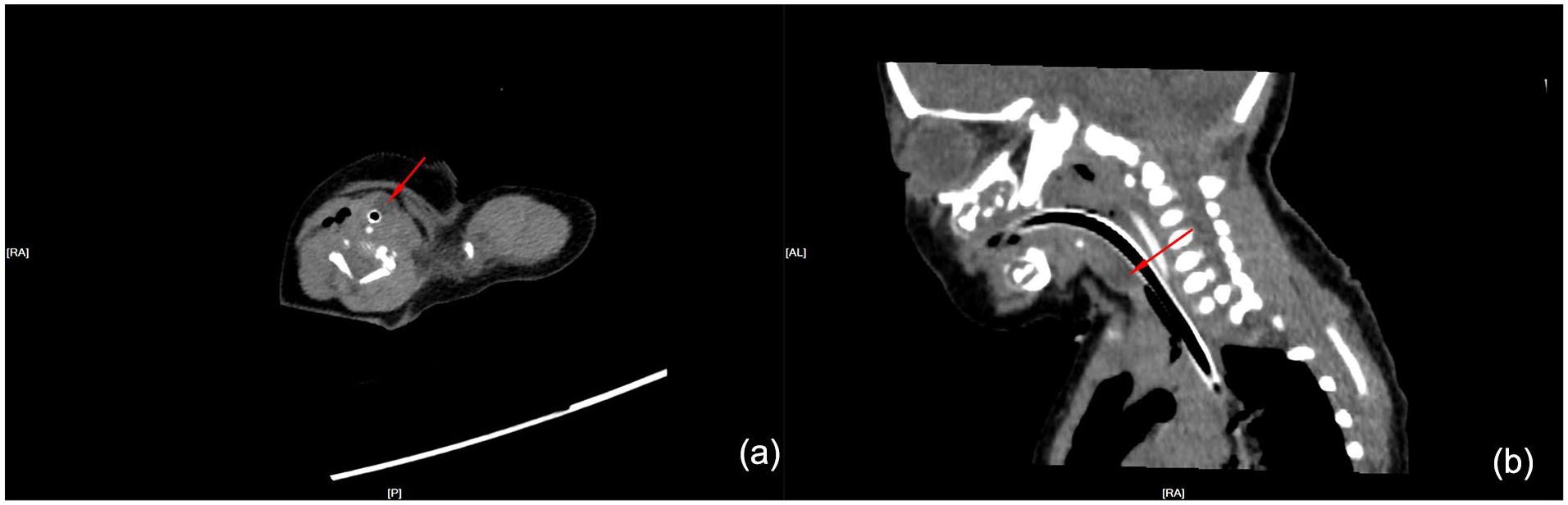
CT axial section (a) and sagittal section (b), arrows indicate a quasi-circular mass.
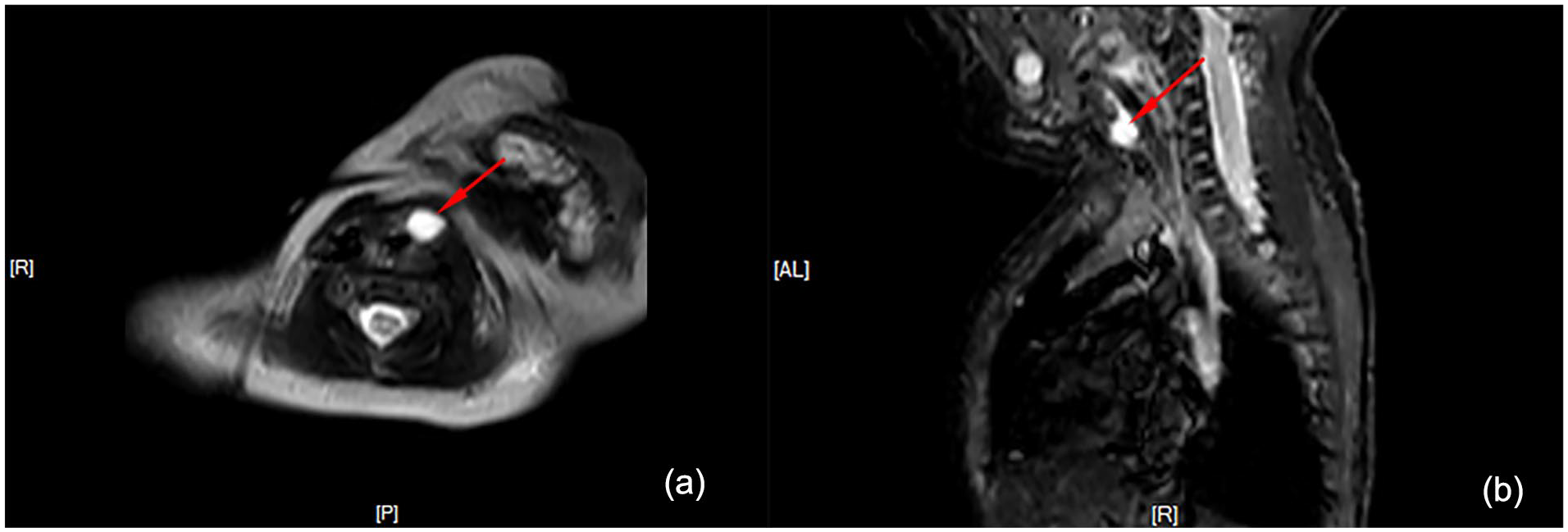
The axial (a) and sagittal (b) sections of the MRI, with arrows pointing to the lesion that exhibited long T1 and T2 signal shadows. MRI, magnetic resonance imaging.
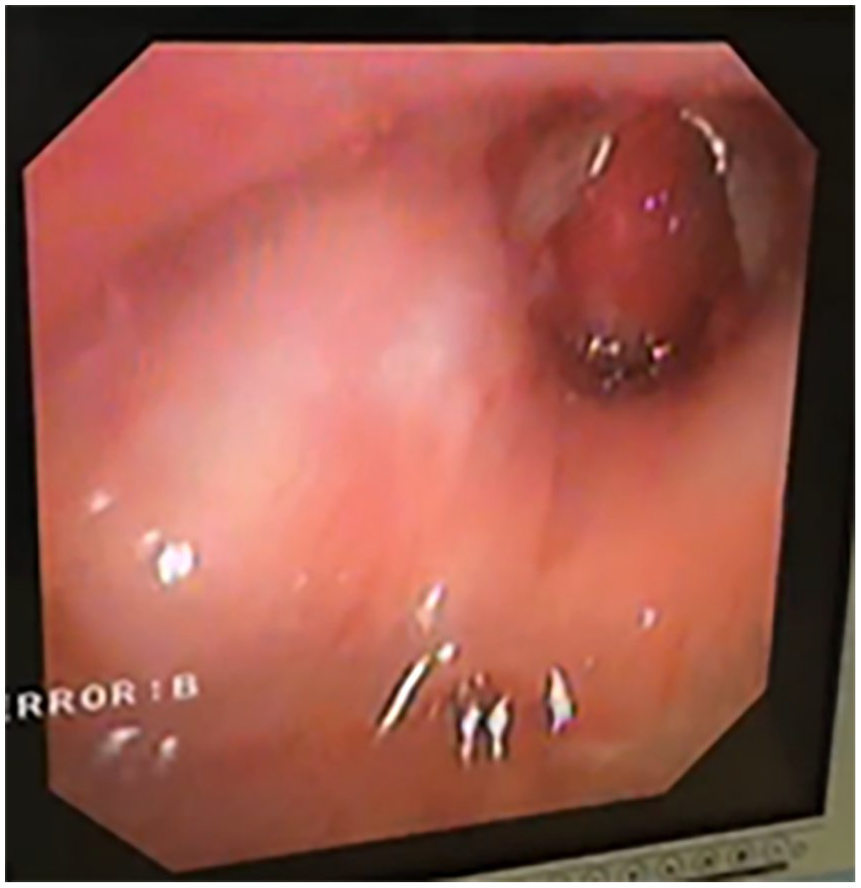
A preoperative bedside laryngoscopy image, indicating airway obstruction of >75% by the cyst.
To minimize potential airway damage from prolonged intubation or surgical intervention in the neonate, we planned endoscopic marsupialization of the subglottic cyst. Given the substantial size of the cyst, we opted to perform the procedure with the endotracheal tube in place to prevent airway obstruction, despite the reduced operative space. On reaching the operating room, the infant was ventilated with an endotracheal tube. Anesthesia was induced with 3 mg propofol and 3 µg fentanyl administered slowly intravenously, and maintained with 2% sevoflurane at a flow rate of 2 L/minute. Following successful anesthesia induction, the endotracheal tube was exchanged for a size 3.0 PORTEX(c) clear PVC, oral, soft seal cuff south polar preformed tracheal tube positioned at a depth of 10 cm. The patient was placed in the Boyce Jackson position and the epiglottis was lifted using a direct laryngoscope to fully expose the glottis. A 0° endoscope revealed a cystic neoplasm below the vocal cords with a smooth surface, causing significant narrowing in the glottic area. Therefore, laryngeal forceps were used to excise part of the neoplasm and remove as much of the cyst wall as possible. This allowed for better visualization of the base of the cystic cavity. Following the excision of the cystic mucosa, hemostasis was achieved using an adrenaline-soaked cotton ball. Next, dexamethasone solution (5 mg) was injected into the mucosa at the cyst base. Postoperative bedside ultrasound confirmed the disappearance of the cervical cyst. The patient was returned to the ICU with the tracheal tube in place.
For infection control, cefoxitin combined with amoxicillin and sulbactam sodium were administered postoperatively. Postoperative care focused on maintaining circulatory and internal stability, alongside routine endotracheal humidification and sputum suction. The tracheal tube was successfully removed on the second postoperative day. A follow-up neck ultrasound performed 10 days postoperatively revealed a recurrent cyst measuring approximately 5 mm × 2.5 mm. However, the infant showed no stridor, rapid breathing, or swallowing difficulties at rest and only mild stridor was audible during intense crying. To avoid secondary airway mucosal injury from repeated surgeries, observational follow-up was recommended.
Follow-Up
Neck ultrasound at 1 month, 2 months, and 1 year postoperatively showed no cyst growth. A neck ultrasound in the third year postoperatively indicated cyst regression, and a video laryngoscopy revealed no subglottic cysts (Figure 4 and Table 1).
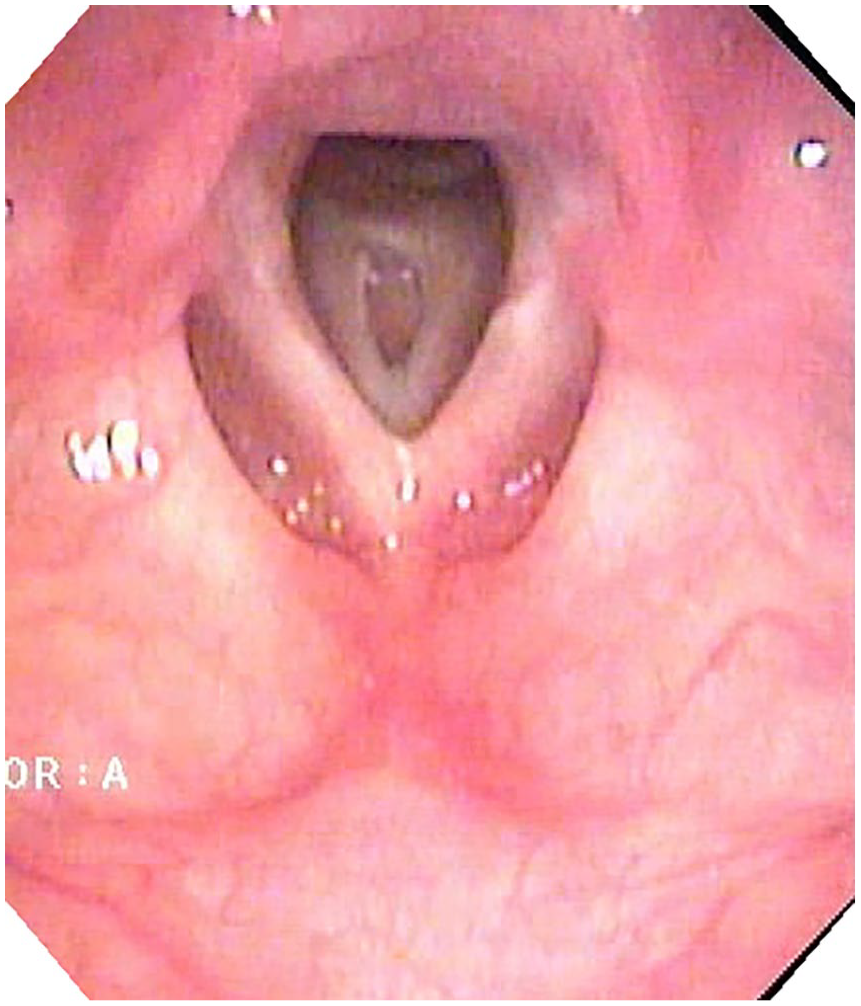
The laryngoscopic view 3 years postoperatively, showing the site of the original cyst excision in the subglottic area.
Timeline: Illustrates the Treatment Timeline for the Child From the Onset of Respiratory Distress to the Conclusion of Treatment, Spanning a Period of 3 Years.
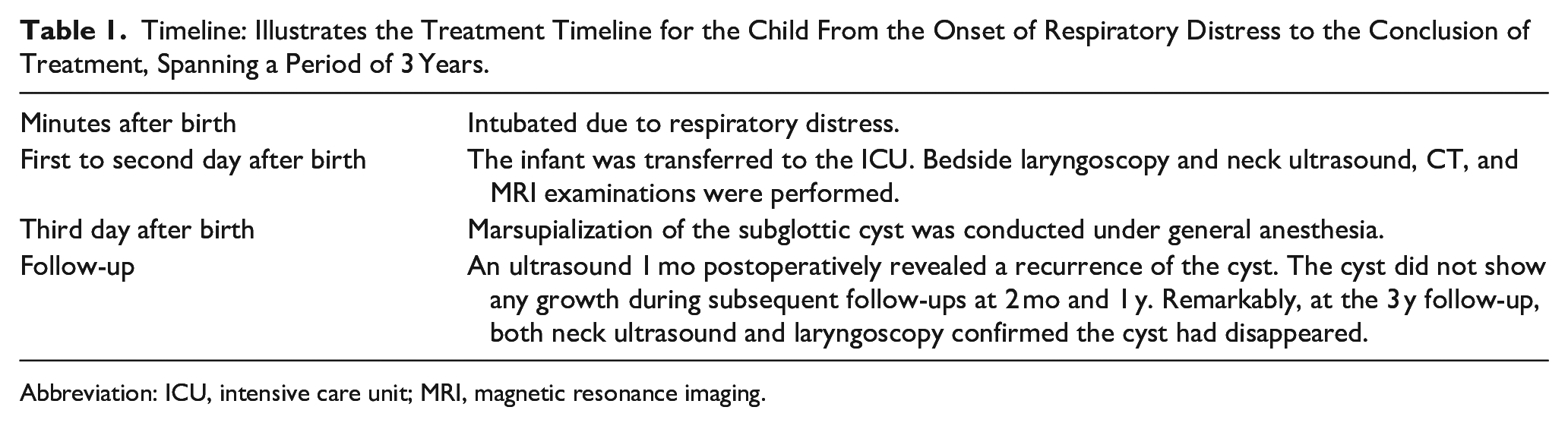
Abbreviation: ICU, intensive care unit; MRI, magnetic resonance imaging.
Discussion
The vague symptoms associated with subglottic cysts can pose a challenge for accurate diagnosis. A high level of clinical suspicion is necessary to ensure that timely and appropriate investigations and interventions are carried out. The common symptoms of subglottic cysts—such as dysphonia, dysphagia, hoarseness, stridor, and dyspnea—are more readily identified in older children. These cysts can be easily misdiagnosed as laryngomalacia, croup, or subglottic stenosis due to overlapping clinical presentations and the relative rarity of congenital subglottic cysts. 2 Consequently, diagnostic laryngoscopy and bronchoscopy are recommended for airway assessment in infants considered at risk.
However, certain historical and physical examination findings can help clinicians distinguish between these conditions. Stridor indicates an obstruction at some level within the laryngotracheal tract. Monitoring the response to treatment can provide valuable diagnostic clues. Inflammatory conditions like croup often respond well to epinephrine and corticosteroids. PEEP or continuous positive airway pressure can be particularly effective in cases of dynamic obstruction, such as tracheobronchomalacia. Laryngomalacia, the most common cause of neonatal stridor, often worsens during feeding, crying, or when the infant lies on their back. 3
The pathophysiology of both congenital and secondary subglottic cysts, collectively termed cysts in the subglottic area, remains unclear to this day. Secondary cysts are more common in children with a history of tracheal intubation and ventilatory support, whereas congenital cysts occur in children without previous airway interventions. 4 Congenital subglottic cysts are exceedingly rare, with an incidence rate of 1.82 to 3.49 per 100,000 live births. The choice of surgical method currently lacks evidence for optimal treatment, but the main principle is to minimize secondary airway injury as much as possible. 5 Endoscopic marsupialization using cold steel instruments is a common treatment for subglottic cysts. Alternative modalities such as CO2 laser, coblation, and microdebridement are employed with caution to prevent circumferential scarring in the already narrow airways of neonates and infants. Due to the rarity of congenital subglottic cysts, there is no established consensus for their treatment. Nevertheless, the primary goal remains the same: to ensure a patent airway, alleviate symptoms, minimize residual scarring, and prevent recurrence. 6 According to a 2022 study by Ünsaler et al on 15 cases of subglottic cysts, endoscopic marsupialization is effective for cysts with thin and transparent walls, showing a low recurrence rate. Simple endoscopic marsupialization often fails to yield good results for thick-walled or submucosal cysts associated with subglottic stenosis and may require more complicated procedures, including balloon dilation or even laryngotracheal reconstruction. 7 Due to the large size of the cyst, we performed the surgery with tracheal intubation under general anesthesia to avoid the risk of airway obstruction. A size 3.0 PORTEX(c) clear PVC, oral, soft seal cuff south polar preformed tracheal tube was selected for anesthesia to ensure the safety of the surgery. Due to the presence of the tube, the operative space was limited, leading to the preservation of more cystic wall mucosal tissue, which could have resulted in cyst recurrence, as shown by ultrasound only 10 days after surgery. The literature on cyst recurrence often speculates that it is related to the retention of cystic mucosa during surgery. Therefore, we recommend removing the tracheal tube after cyst marsupialization and excising as much of the cystic wall tissue as possible while maintaining spontaneous breathing under anesthesia. This technique is similar to the approach used for removing tracheal foreign bodies. The goal is to preserve normal tracheal mucosal tissue to reduce the risk of recurrence. 8 In congenital cysts cases, repeated surgeries involving general anesthesia and intubation could lead to secondary airway stenosis, manifesting as secondary cysts or scarring. Therefore, it is crucial to minimize the number of surgical interventions as much as possible.
Secondary cysts are generally believed to result from tracheal mucosal injury and ulceration, followed by subepithelial fibrosis and obstruction of the mucous gland ducts. 2 However, the pathophysiological mechanism of congenital cysts remains unclear. Observation and follow-up are usually sufficient for smaller cysts in the absence of stridor. During the 3 year follow-up period, the cyst did not expand further. In the third year, neck ultrasound unexpectedly showed that the cyst had disappeared. There are 2 speculated reasons for the resolution of subglottic cysts post-surgery: (1) The cyst wall ruptured due to external forces such as violent coughing after becoming thinner post-surgery. (2) It is possible that the cystic fluid was reabsorbed on its own. Due to the limited number of cases, more studies are needed to provide a comprehensive understanding of the pathophysiology of congenital subglottic cysts.
Footnotes
Author Contributions
Xiaoxu Zhang: propose the idea and write the article. Qiulan Shi: review the article and revise the article. Both authors have read and approved the final manuscript.
Consent for Publication
All authors have read and approved the article for submission to your respected journal.
Data Availability Statement
All authors declare that raw data and other materials are available on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Children’s Hospital of the Nanjing Medical University, and written consent was obtained from the patients’ guardians.